
記住我
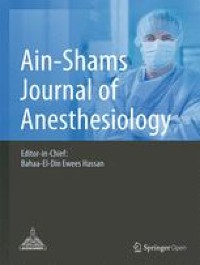
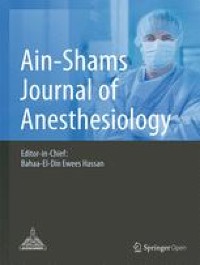

A 10-year-old female child, weighing 20 kg, was referred for closure of acquired tracheoesophageal fistula (TEF) at C7 (Figs. 1 and 2) and D2 level (Fig. 3), persistent even 4 months after completion of chemotherapy course (6 cycles, EURONET protocol) for nodular sclerosis type of Hodgkin’s lymphoma (stage 3 B + E). This case was previously reported, after 4 cycles of chemotherapy while being conservatively managed associated with improvement in systemic symptoms and subjective improvement in overall health with 2 kg weight gain (Munikoty et al. 2017). However, she continued spitting saliva with episodes of respiratory distress. There was poor right vocal cord movement. The child had been on nasogastric tube feed for 11 months as the family had refused a gastrostomy. There was constant fear of aspiration and poor quality of life.
Fig. 1
Tracheoesophageal fistula after chemotherapy at C7 vertebra level with dimensions of 2.2 cm × 2.5 cm × 2.4 cm
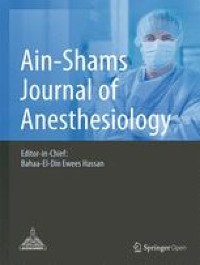
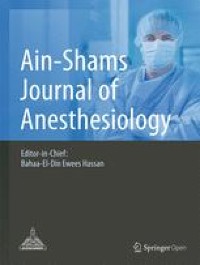
Fig. 2
Fistula at C7 vertebra level
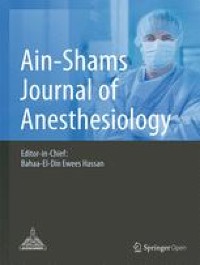
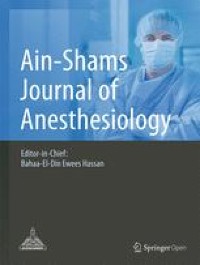
Fig. 3
Tracheoesophageal fistula at D2 vertebral level
The pre-anesthetic evaluation revealed no history suggestive of any systemic illness other than the lymphoma. The general physical, systemic, and airway examination revealed no abnormality. The baseline hemogram, serum electrolytes, renal function tests, and coagulogram were within normal limit. The child was fasted overnight and started on 60 ml/kg of Ringer lactate maintenance fluid during the fasting period. Aspiration prophylaxis in the form of injection pantoprazole 20 mg and injection metoclopramide 3 mg was administered on the morning of surgery. Before taking the child inside the operation theater, she was premedicated with 80 μg glycopyrrolate. No sedative premedication was administered.
Intraoperative monitoring consisted of ECG, NIBP, SpO2, end-tidal CO2, nasopharyngeal temperature, and urine output. Intravenous induction was carried out using 2 mg of morphine, 40 mg of propofol, and atracurium 20 mg followed by maintenance on propofol infusion. Under general anaesthesia, rigid bronchoscopy was performed initially and a Fogarty catheter passed across the fistula. Thereafter, trachea was intubated with a Kimberly Clark 5.5 mm microcuff pediatric endotracheal tube (ETT) (Fig. 4) which has a high-volume, low-pressure cuff which is less traumatic with better sealing of anesthetic gases, using CMAC® video laryngoscope. ETT position was also confirmed using fiber-optic bronchoscope besides bilateral chest auscultation and fixed at 18.5 cm. The child was ventilated with inspiratory pressure of 14 cmH2O and PEEP of 5 cmH2O, and respiratory rate was adjusted to maintain ETCO2 between 35 and 40 mmHg. An 18G intravenous cannula and a 22G left radial arterial cannula were secured. Anesthesia was maintained with isoflurane in a mixture of air and oxygen. Surgery was performed in left lateral position. In spite of extensive fibrosis, making separation of trachea from esophagus difficult, the two were adequately mobilized and closed, with a sternocleidomastoid muscle interposition graft. A gastrostomy, feeding jejunostomy, and tracheostomy were placed. Serial intraoperative ABGs were within normal limits. Perioperative analgesia consisted intravenous morphine (2 mg), fentanyl (40 mcg), paracetamol (300 mg), and intercostal nerve block with 0.1% ropivacaine before closure of wound. Ondansetron (2 mg) was also given for prevention of postoperative nausea and vomiting. Patient was shifted and intubated to surgical intensive care unit for elective mechanical ventilation for better graft healing and uptake.
Fig. 4
5.5 mm microcuffed endotracheal tube
She was sedated and electively mechanically ventilated to allow for the graft to heal and allow its proper uptake, following which she was gradually weaned off the ventilator by the eleventh postoperative day. The postoperative period was uneventful. Oral feeds were gradually started following a contrast esophagogram on day 14. She was discharged home with tracheostomy in situ and decannulation done a month later. At more than 1-year follow-up, she is on solid diet with no dysphagia. She has mild stridor, the hoarseness of voice has improved, and she is now able to speak a few words and attends school.
留言 (0)