
記住我










Objectives: To summarize cases of venous thromboembolism (VTE), including pulmonary embolism (PE) and deep vein thrombosis (DVT) among coronavirus disease (COVID-19) patients and discuss their symptoms, diagnostic method, clinical features, and prognosis.
Methods: All major databases were searched for relevant studies published between December 1, 2019 and May 5, 2021.
Results: A total of 233 articles were identified, 22 describing 48 patients were included. A total of 79.1% had PE and 20.9% had DVT. Most patients were men, with a mean age of 56 years. Comorbidities were present in 70.8%, and 85.4% had at least one risk factor of VTE. 56.3% had received anticoagulation therapy. Most patients were treated in the general ward. Complications occurred in 27.1% of the patients, and recovery was achieved in 80.4%.
Conclusion: Venous thromboembolism must be suspected even in patients who had received prior anticoagulant regimens or in stable cases, especially in males, the elderly, and patients with comorbidities and high D-dimer levels.
Keywords:Coronavirus disease (COVID-19) is a condition induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The clinical characterization of COVID-19 varies widely, ranging from symptomless to life-threatening illnesses.1
Coronavirus disease is linked to a serious illness course in approximately 23% of infected people and death in approximately 6% of those affected. Individuals with comorbidities and clinical symptoms related to COVID-19 severity should be regularly evaluated, and high-risk groups should be the focus of preventative efforts.2 Inflammation and coagulation malfunction were found to be risk factors for a complicated disease course.3 Pulmonary embolism (PE) and deep veinous thrombosis (DVT) are examples of venous thromboembolism (VTE), which has been addressed frequently as a common cardiovascular complication among patients with COVID-19. However, higher levels of thrombotic markers have been discovered to be linked to poor clinical outcomes.4
A recently published meta-analysis5 revealed that the combined incidence rates of VTE, PE, and DVT in hospitalized COVID-19 patients were 21%, 15%, and 27%, accordingly. These rates were higher among patients in the intensive care unit (ICU), and the findings suggest that anticoagulant use was not related to a reduced risk of mortality. Thus, evaluation of the prophylactic and therapeutic anticoagulation roles of COVID-19 is required.5 Another meta-analysis of 1,988 patients revealed a significant prevalence rate of thromboembolic disorders among COVID-19 patients. In these patients, the prevalence rates of VTE was 31.3%, DVT was 19.8%, and PE was 18.9%. This highlights the importance of appropriate screening methods and antithrombotic implantation to avoid fatal and severe consequences.6
The intrinsic pathophysiology of COVID-19-associated hypercoagulability and coagulation disorders is not fully understood. However, several hypotheses have been proposed to explain possible pathophysiological mechanisms, including receptor binding, complement activation, cytokine storm, and direct viral endothelial damage.7,8
The purpose of this meta-case summary is to review and summarize published cases of VTE, either PE or DVT, in patients with COVID-19 and to discuss their symptoms, diagnostic method, clinical features, and prognosis. Also, to shed light on different management practices for VTE.
MethodsWe carried out a search on major data bases such as Web of Science, PubMed, Medline, and Scopus to identify all relevant articles published between December 1, 2019, and May 5, 2021. The search algorithms were “COVID” or “coronavirus” or ‘SARS-CoV-2” and “venous thromboembolism (VTE)” or “pulmonary embolism (PE)” or “deep vein thrombosis (DVT)”. The search was not limited by publication date or language.
Clinical studies with the following criteria were considered for inclusion were patient with confirmed diagnosis of COVID-19 and VTE has been detected. There were no limits on the type of publication, both case reports and case series were included. Studies that did not report cases of VTE, DVT, or PE, and animal studies were excluded. Two researchers independently screened titles and abstracts, and any inconsistencies were resolved by a discussion. The data was obtained into a standard format, that included: patient features, duration and severity of coronavirus infection, type, and symptoms of VTE, investigations, management, and prognosis. The studies were classified according to the type of VTE treatment and the severity of the coronavirus infection. The qualities of the studies were assessed using the Newcastle-Ottawa scale, a validated measure for case reports and case series.
Statistical analysisFindings are summarized in tables and in a meta-summary. Flowcharts of the included studies are presented in diagrams and in a summary of pooled VTE cases. In the meta-summary, patients with verified VTE cases were presented in compared to patients with potential instances of the disease. Frequency and percentage are used to present categorical variables. Mean, standard deviation (SD), median and interquartile range were used to represent the continuous variables. Statistical analysis carried out using Statistical Package for Social Sciences, version 25.0. (IBM Corp. Armonk, NY).
ResultsDuring the search, 233 articles were identified. The 208 articles were eliminated according to their titles and abstracts. Three full-text articles were eliminated due to a lack of VTE description in the remaining 25 publications. Thus, 22 studies9-30 representing 48 cases were included in the meta-summary. Fourteen studies were carried out in the United States,9,10,15-19,21-24,28-30 7 in Europe,11-14,20,25,26 and one was carried out in the United Arab Emirates.27 Of the studies, 12 were case reports and 10 were case series. Figure 1 illustrates an overview of the article selection process.
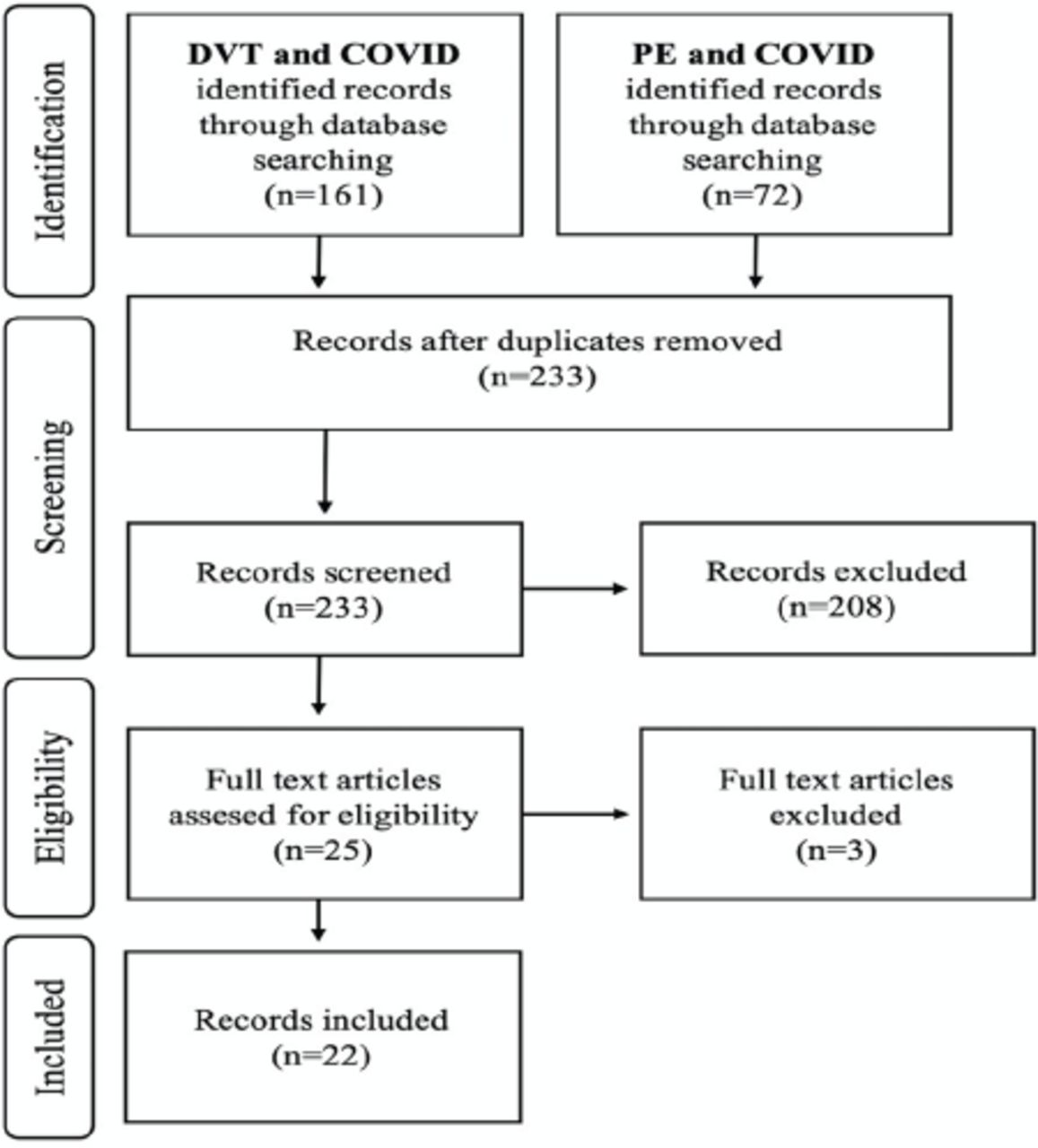 Figure 1
Figure 1 - Flow chart of study selection.
The features of the published cases of COVID-19-associated VTE are presented in Table 1. The patients varied in age from 20 to 92, with a mean of 56 years. Males accounted for 70.8% of the total number of patients. The following were the most prevalent comorbidities: hypertension (39.6%), diabetes mellitus (27.1%), and dyslipidemia (22.9%). Most patients presented with risk factors of VTE, such as advanced age (79.2%), overweight/obesity (12.5%), and prior VTE events (6.2%).
Table 1- Characteristics of published cases of coronavirus associated venous thromboembolism (N=48).
Table 1- Characteristics of published cases of coronavirus associated venous thromboembolism (continuation).
Coronavirus disease-19 was most associated with the following symptoms: fever (60.4%), cough (60.4%), shortness of breath (50%), fatigue (18.8%), myalgia (18.8%), headache (12.5%,), diarrhea (12.5%), and chest pain (10.4%). Other reported symptoms included chills, nose congestion, nausea or vomiting, sore throat, and loss of taste or smell.
Of the 48 patients, 79.1% had confirmed cases of PE, and 68.4% were males. The most common presenting symptoms of PE were dyspnea (62.5%) and chest pain (18.8%), whereas the most common signs were hypoxia (18.8%) and tachycardia (4.2%). The remaining 10 patients (20.9%) were confirmed to have DVT, most of whom were men (80%). The most common presenting symptoms of DVT were unilateral swelling of the lower extremity (8.3%) and leg pain or tenderness (6.2%). Only 3 patients developed PE after DVT diagnosis.
Of the 48 patients with confirmed COVID-19 infection, 15 were treated with hydroxychloroquine; 6, azithromycin; 5, steroids (dexamethasone); 5, cefepime; 5, convulsant plasma; 4, amoxicillin clavulanate; 3, linezolid; and 2, oseltamivir.
Most patients were treated in the general ward, with a mean length of hospital admission of 4.90±4.45 days. Only 20.8% of the patients were transferred to the ICU. The average duration of ICU admission was 3.3±8.25 days. Recovery or hospital discharge was achieved in 80.4% of patients with COVID-19, whereas 19.6% died.
The investigation results and imaging characteristics of the confirmed cases of COVID-19-associated VTE are presented in Table 2. D-dimer levels were found to be increased in 78.9% of patients with PE and 90% of those with DVT. Troponin levels (troponins I or T) were found to be high in 13% of the patients. The N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) level was underreported and raised in 7% of the patients. In most patients, other inflammatory indicators such as white cell count, ferritin, and C-reactive protein levels were raised.
Table 2- Imaging characteristics of confirmed cases of coronavirus associated venous thromboembolism.
Chest radiography was performed for most of the patients, of whom 52.1% had signs of pneumonia, such as consolidation, ground-glass opacities, and infiltration. Echocardiography results were reported in only 11 patients, 10 of whom had abnormalities consistent with moderate to severe pulmonary embolism. Features included dilated right ventricle, systolic septal flattening, hypercontractile apex, and right ventricle dysfunction. An electrocardiography result was reported in only 4 patients, most of whom had a normal sinus rhythm.
The diagnosis of PE was confirmed using computed tomography (CT) and pulmonary angiography (CTPA), while the diagnosis of DVT was confirmed with duplex ultrasonography, compression ultrasonography (CUS), or CT venography in most cases. The most common CTPA finding was bilateral PE, followed by right- and then left-sided pulmonary embolism.
The types of anticoagulants used to treat the confirmed cases of COVID-19-associated VTE are presented in Table 3. Of the 48 patients, 56.3% had received anticoagulant therapy prior to VTE diagnosis (either for the treatment of a preexisting medical condition or as a prophylaxis during hospitalization). Of the patients, 51.9% were taking low-molecular-weight heparins (LMWHs) such as nadroparin and enoxaparin, 25.9% were taking heparin, and 22.2% were taking novel oral anticoagulants (NOACs) such as apixaban and rivaroxaban. During hospital admission, after VTE diagnosis, the most used medications were LMWHs (62.5%), intravenous heparin (22.9%), tissue plasminogen activators (14.6%), NOACs (10.4%), and venoarterial extracorporeal membrane oxygenation (4.2%). Upon discharge, NOACs and LMWHs were prescribed to 58.3% and 18.8% of the patients, respectively. The other medications prescribed included warfarin and acetylsalicylic acid. The discharge plans of the remaining patients (22.9%) were unclear owing to either death or car withdrawal, or because they were not fully reported.
Table 3- Anti-coagulation type used to treat confirmed cases of coronavirus associated venous thromboembolism.
Complications such as stroke, respiratory failure, shock, acute kidney injury, ventilator-associated pneumonia, bleeding in the oropharynx, and multiorgan dysfunction were found in 27.1% of the patients during admission and were associated with older age and poor prognosis.
DiscussionThis meta-analysis, which included 48 patients, revealed that VTE occurred in a significant number of patients with COVID-19, regardless of whether they were treated in the general ward or admitted to the ICU. Pulmonary embolism episodes were more common than DVT episodes. Our results support the potentially higher incidence rates of COVID-19-associated VTE in males, the elderly, and those with hypertension, diabetes mellitus, dyslipidemia, and elevated D-dimer levels. However, despite some complications during admission, most patients had a good prognosis and were discharged alive. This study also discussed diagnostic procedures and management plans for patients with COVID-19, including antiviral medicines and various anticoagulant regimens.
Pulmonary embolism is usually triggered by DVT, alhtough the presence of PE does not always indicate the existence of DVT. Thus, the detection of both acute PE and DVT in patients with COVID-19 is essential. The diagnosed of PE in COVID-19-affected patients may have a concomitant lower-extremity DVT occurrence in less than 50% of cases. Even though lower limb DVT is the predominant type, a recent retrospective review of 257 moderate-to-severe COVID-19 patients found that upper extremity deep vein thrombosis (UEDVT) occurred in approximately 10.9% of the patients (9% CI, 7.1-14.7) especially when other risk factors like venous catheters or venous stasis existed. Furthermore, when compared to individuals who did not require ventilation, using continuous positive airway pressure (CPAP) raised the incidence of UEDVT by 6 times. The presence of UEDVT has been linked to a poor prognosis and death.31
In patients with COVID-19, abnormal coagulation results such as disseminated intravascular coagulation and markedly elevated levels of D‐dimer and fibrin degradation products are linked with poor outcomes and death.32 A published systematic review assessed the diagnostic precision of D-dimer tests for PE and found that D-dimer levels >500 and >1000 µg/L showed high sensitivity (96% and 91%, respectively) but low specificity (10% and 24%, respectively) in the diagnosis of PE in patients with COVID-19, which is equivalent with the sensitivity of D-dimer levels in patients without COVID-19.33
On the other hand, a multicenter retrospective analysis that included 451 hospitalized patients with COVID-19 who underwent an ultrasonographic evaluation revealed that 14% of the patients had acute DVT. The D-dimer level was the most important influencing factor of the risk of DVT, and D-dimer levels > 5000 ng/mL were considered beneficial for predicting DVT. Therefore, in the early stages of COVID-19, regular D-dimer monitoring may be beneficial.34 In our summary, most patients with PE and DVT had a positive D-dimer test result (>500 µg/L; Table 1). However, in consideration of the high range of occurrence of VTE in patients with COVID-19, a high standard of doubt is essential, regardless of the D-dimer value.
A recent systematic review was conducted to identify the lung histopathological features of COVID-19 and to see how they relate to another previous viral pandemic. The review revealed that the presence of microthrombi in capillaries, small and medium vessels was a frequent histopathological pattern in lung pathologies in patients with COVID-19 (57%) and SARS (58%) in comparison to those with H1N1 influenza (24%). This points to a link between coronaviruses and microthrombi.35
In a recent retrospective study in Italy, 476 hospitalized COVID-19 patients from the first (n=316) and second (n=160) COVID-19 waves were compared. There were no significant variations in baseline features, admission biomarkers, severity metrics, or lethality between the first and second COVID-19 waves of patients admitted to a particular hospital and undergoing standard-dose thromboprophylaxis. However, a larger percentage of patients in the second wave had acute respiratory distress syndrome (46.3%) compared to the first wave (29.1%). The median length of hospitalization was longer in the second wave (17 days) compared to the first wave (10 days). In addition, the second wave had a greater rate of VTE. Possible explanations include a longer stay in the hospital, more diagnostic testing, and increased knowledge of thromboembolic problems. This emphasizes the fact that VTE identification is not completely reliant on the presence or absence of common signs and symptoms; rather, more frequent imaging is linked to more VTE incidents diagnoses.36
Several studies have indicated the risk of VTE since the COVID-19 epidemic started in both inpatient and outpatient patients with COVID-19. According to the recommendations of the VAS European Independent Foundation in Angiology/Vascular Medicine, patients who undergo home therapy for COVID-19 should begin thromboprophylaxis with LMWH, rivaroxaban, or betrixaban. For hospitalized patients, thromboprophylaxis should be administered with weight-adjusted intermediate doses of LMWH. For the treatment of VTE or hypercoagulability during hospital admission, LMWHs are preferable to unfractionated heparins or NOACs. After discharge, prolonged thromboprophylaxis with LMWH, rivaroxaban, or betrixaban is recommended.37 National Institute for Health and Care Excellence (NICE) recommendations which were recently released, suggested administering LMWH at a therapeutic dosage for people with COVID-19 who need oxygenation without an increased risk of bleeding.38 We found that LMWHs (enoxaparin, dalteparin, and nadroparin) were the most frequently used medications for prophylaxis and the treatment of hospitalized patients, whereas NOACs (apixaban and rivaroxaban) were the most frequently used medication after discharge.
In a recently published prospective cohort study with almost 6195 patients with COVID-19, 598 patients were hospitalized upon diagnosis, and 5597 were managed as outpatients. Of the outpatients, 2.9%received outpatient anticoagulation (OPAC). The likelihood of being admitted to the hospital was lowered by 43% in the patients who were receiving OPAC before the diagnosis of COVID-19. Unfortunately, owing to the small number of users, the precision of the effect of the type and dosage of the anticoagulants used, such as warfarin, NOACs, and enoxaparin, were inadequate. Furthermore, in hospitalized COVID-19 patients, failure to start anticoagulation or to continue OPAC was linked to a greater mortality risk.39 In 89.6% of the cases in our summary, the COVID-19 signs and symptoms lasted for 7.91±7.03 days, and VTE was discovered 10.30±7.92 days after diagnosis. This emphasizes the significance of initiating thromboprophylaxis upon diagnosis.
Owing to the ongoing pandemic, it is essential to promote awareness of VTE as a possible complication of COVID-19 infection. Many approaches have been used to reduce the likelihood of VTE occurrence and to control confirmed cases. However, failure of thromboprophylaxis and the presence of VTE in patients with COVID-19 admitted to ICUs imply that rather than a broad treatment plan, a customized approach tailored to the severity and stage of the disease should be used.40 In France, a comprehensive multi-center retrospective study was carried out to investigate the impact of intermediate-dose compared to standard prophylactic anticoagulation (AC) in COVID-19 patients admitted to medical wards. In-hospital mortality was not considerably different.41 In our meta-case summary, 56.3% of the patients had received anticoagulant therapy prior to hospitalization. However, it did not reduce the incidence rate of VTE, or complications found upon admission, which suggests a prophylaxis failure.
Novel oral anticoagulants are among the commonly used anticoagulants and have demonstrated acceptable efficacy/safety features; nonetheless, some studies have shown drug-drug interactions between NOACs, and specific antiviral drugs used in patients with COVID-19.38 A recent study compared 13,003 patients with COVID-19 who received NOAC therapy (dabigatran, apixaban, rivaroxaban, or edoxaban) without any other accompanying anticoagulation for at least one year prior to COVID-19 diagnosis and were still receiving this therapy at the time of diagnosis with another 13,003 patients with COVID-19 who did not take any anticoagulant therapy (either oral or parenteral). Surprisingly, the authors found that prolonged use of NOAC therapy up to the time of COVID-19 diagnosis was not related to better clinical outcomes or reduced hospitalization/rehospitalization rates than those in patients with COVID-19 who were not treated with oral anticoagulants.42
Study limitationsThe present meta-analysis has some limitations that must be addressed. The qualities of the included studies had low levels of evidence. Most of them were case reports and case series which may not be representative of all cases. Some of the collected data were incomplete, posing a high risk of prejudice in information. The study comprised a limited number of studies, and each study had its own patient selection bias.
In conclusion, this meta-summary of cases of VTE associated with COVID-19, we identified 10 cases with DVT diagnosed using duplex ultrasonography, compression ultrasonography, or CT venography, and 38 cases with PE based on CTPA with high D-dimer levels and evidence of strain on echocardiography. Patients with VTE often developed common COVID-19 symptoms, including fever, cough, chest pain, fatigue, and shortness of breath. In general, both acute and chronic presentations of VTE are common; however, in individuals with COVID-19, acute VTE can cause serious illness and death.
A high index of suspicion among COVID-19 patients is essential, irrespective of whether they are treated in the general ward or in ICU settings or with anticoagulant therapy prior to or during COVID-19 diagnosis. Our review provides a glimpse into the current management practices used in individual cases of VTE practices and warrants future investigations in larger number of cases.
AcknowledgmentThe authors gratefully acknowledge Scribendi (www.scrobendi.com) for the English language editing.
FootnotesDisclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
Received April 15, 2022.Accepted June 13, 2022.Copyright: © Saudi Medical JournalThis is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
留言 (0)