
記住我


Tardive dyskinesia (TD) is a debilitating and potentially irreversible condition that usually occurs in patients with mental illness during or after cessation of treatment with dopamine-receptor antagonists or partial agonists (mainly antipsychotic medications). It is characterized by involuntary hyperkinetic movements in the oral/lingual/buccal area, trunk, or extremities. Although the social stigma caused by TD is obvious,1 in some cases, TD also leads to impaired speech or swallowing, dental damage, and difficulties with gait and posture that affect activities of daily living.2–4 As a consequence, patients with TD experience significantly impaired health-related quality of life and increased morbidity compared with non-TD patients with mental illness.2,3,5–7
In a recent meta-analysis, the overall mean global prevalence of TD was estimated to be 25% among patients receiving antipsychotic medications; however, prevalence estimates vary from approximately 8% to 30% according to background treatment, age, region, and other factors.8 In addition, incidence increases cumulatively with duration of antipsychotic treatment up to 68% in patients with 25 or more years of antipsychotic use.9 The risk of TD may be lower with second-generation antipsychotics (SGAs) compared with first-generation antipsychotics (FGAs), with annualized incidence rates of 2.6% and 6.5%, respectively,10 and the use of SGAs has become more widespread than the use of FGAs. In fact, expanded drug indications and increased off-label prescription of SGAs have placed more patients than ever at risk for TD.11
The significant health care burden associated with mental illnesses such as schizophrenia (SCZ), bipolar disorder (BP), and major depressive disorder (MDD) is well established12,13; however, less is known about the incremental burden incurred by patients who develop TD. In these patients, additional health care resource requirements may be impacted both because of the dyskinesia and also because of changes in the management of the underlying mental illness, such as optimization of antipsychotic medication14 and the risk of psychotic relapse and rehospitalization associated with these optimization attempts.14–16 Retrospective claims database studies confirm significantly increased health care utilization and costs associated with TD17–19; however, additional data from diverse patient populations are required to improve understanding of the health care burden associated with TD. We have therefore performed a retrospective database analysis to assess the patient characteristics, treatment patterns, and the economic burden associated with TD in Israel.
MATERIALS AND METHODS Study Design and Data SourceThis was a retrospective analysis of data from the Maccabi Healthcare Services (MHS) database, a nationwide health plan (payer-provider) containing longitudinal data on a stable population of 2.3 million individuals in Israel (representing 25% of the national population with a >99% annual retention rate). The MHS database includes comprehensive medical data (diagnoses, laboratory data from a single central laboratory, full pharmacy prescription and purchase data, and demographic characteristics) and uses the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding systems alongside self-developed coding systems that provide more granular diagnostic information beyond the ICD-9-CM codes. Medications were coded according to the Israeli coding system with translations to the anatomical therapeutic chemical coding system where available. Procedures were coded using Current Procedural Terminology codes. The study was approved by the institutional ethics committee of MHS. All data were anonymously analyzed; thus, patient consent was not required.
Study PopulationThe study population included adult patients (aged ≥18 years) within the MHS database who had a diagnosis for TD, identified by the ICD-9-CM codes 333.85 or 333.82, and the corresponding MHS internal codes (TD patients) and matched patients without a diagnosis for TD (non-TD patients; see Statistical Analysis section for more information). Patients were required to have 12 or more months of continuous enrollment in the MHS database before a diagnosis of TD based on an active (chronic) diagnosis, hospital discharge report, preauthorization for drug approval, or 2 diagnoses or more from any health care professional.
Eligible patients who were alive between 2013 and 2018 were included in the analysis of treatment patterns to capture current therapeutic regimens. Treatment patterns were assessed from 2000 to 2018 for the identified population. All medications were available in Israel since 2000. To have at least 1 full calendar year of data, health care resource utilization and cost analyses included TD patients who were alive on January 1, 2018.
Patients' socioeconomic status was categorized into low (1–4), medium (5–6), and high (7–10) based on scores calculated from Points Location Intelligence using geographic information systems and data such as expenditures related to retail chains, credit cards, and housing. This score is highly correlated with socioeconomic status as measured by the Israel Central Bureau of Statistics.20
OutcomesOutcome measures included (1) the physician specialty at first diagnosis of TD, (2) the proportion of patients receiving medications for TD (Supplemental Table 1, https://links.lww.com/JCP/A820, which shows all medications considered), (3) the relative TD treatment coverage calculated by dividing the period of treatment for TD by TD duration from diagnosis to end of follow-up, (4) temporary discontinuation of TD treatment defined as a gap between purchases greater than the number of days of medication supplied by the last purchase plus a grace period of 120 days, and (5) permanent discontinuation of TD treatment defined as a gap between last purchase and end of follow-up greater than the number of days of medication supplied by the last purchase plus a grace period of 120 days.
All patient characteristics were measured on January 1, 2018. Chronic comorbidities were identified using previously validated MHS automated chronic disease registries (cardiovascular disease,21 diabetes,22 hypertension,23 cancer, and chronic kidney disease24). If a patient had an entry date to a registry before January 1, 2018, they were considered to have the comorbidity. Treatment patterns were assessed for the entire period before January 1, 2018. Health care resource utilization was collected for all patients alive on January 1, 2018. Hospitalizations (not including day visits), emergency department (ED) visits, and outpatient visits (including general physician, psychiatrist, neurologist, orthopedist, physiotherapist, and speech therapist visits) were also collected. Costs are reported in total (ie, health care [hospitalization, ED visits, outpatient visits] and medications, excluding procedures) and individually for each component. Costs were extracted from the January 1, 2018, Israel Ministry of Health price list and are reported in US dollars (conversion factor according to Purchasing Power Parities in 2018, US $1 = 3.752 ILS).
Statistical AnalysisPatients without TD who were alive on January 1, 2018, were randomly matched to patients with TD in a 3:1 ratio by underlying disorder (BP, SCZ, MDD, or other mental disorders), birth year, and sex. If a patient had 1 of the 3 major disorders (SCZ, MDD, or BP) and another disorder, the major disorder was considered the main disorder. If a patient had more than one major disorder, the more recent disorder was regarded as the main disorder. Patients with only “other mental disorder” were matched to patients without TD with “other metal disorder” and not by specific individual disorder.
Hospitalizations were analyzed as number of hospitalizations and days of hospitalization, and ED visits were analyzed without regard for the requirement for subsequent hospitalization by TD status. Outpatient visits by TD status were also collected.
Baseline demographics and characteristics were analyzed using descriptive statistics (mean [standard deviation], median [interquartile range ]), and P values are presented for comparisons between TD and non-TD populations. An independent t test was used for continuous variables and a χ2 test for categorical variables.
Clinical and economic burdens by TD status were assessed using generalized linear models were used to assess the difference in health care resource utilization and costs incorporating a negative binomial with log link distribution for health care resource utilization and a γ distribution with log link for cost analyses. Models were adjusted for any variables found to be different at baseline. Because patients with “other mental disorder” were not matched by specific individual disorder, healthcare resource utilization and costs sensitivity analyses were performed using the data for the 3 major mental disorders (SCZ, BP, MDD).
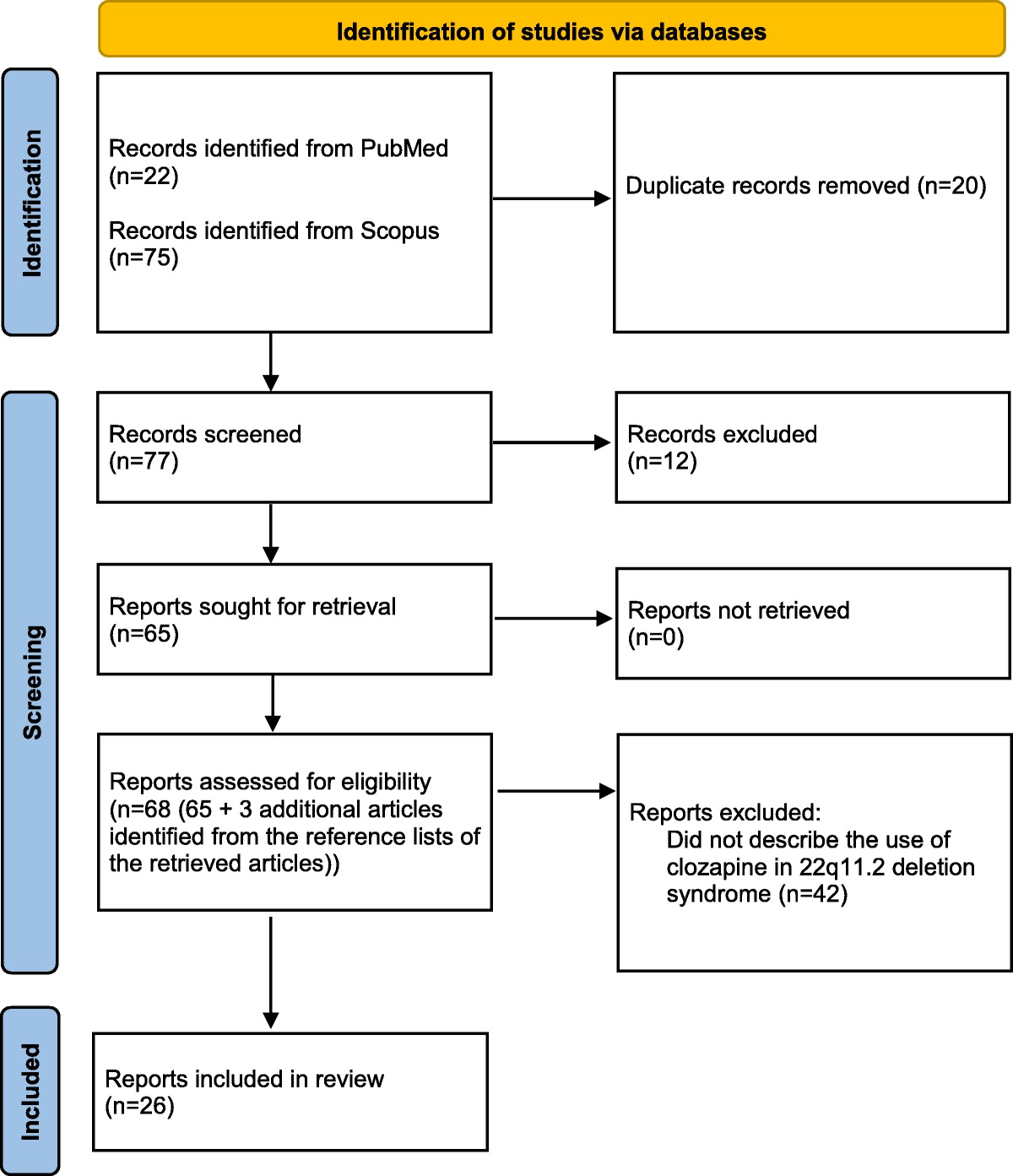
RESULTS PatientsA total of 581 adult patients with 1 or more diagnoses of TD between 2000 and 2018 were identified within the MHS database. From this population, 546 incident cases had 1 or more years of continuous enrollment in the MHS before the first diagnosis of TD (Fig. 1). Of these, 454 patients were alive between 2013 and 2018 and included in the assessment of TD treatment patterns, and 333 patients who were alive on January 1, 2018 were matched to 999 non-TD patients from the MHS database for assessment of health care resource utilization and costs.
 FIGURE 1:
FIGURE 1: Patient disposition.
Treatment PatternsOf the 454 TD patients alive between 2013 and 2018, the median age at diagnosis was 63 years (IQR, 48–74 years), 172 (37.9%) were male, and 113 (24.9%) had low socioeconomic status (Supplemental Table 2, https://links.lww.com/JCP/A821, which shows patient demographic characteristics). Before first TD diagnosis, patients were in the MHS database for a median (IQR) time of 10.6 years (3.7–14.6 years). The median (IQR) length of follow-up after first diagnosis of TD was 5.4 years (2.7–9.6 years). Schizophrenia, MDD, and BP were diagnosed in 178 (39.2%), 85 (18.7%), and 48 (10.6%) patients, respectively, and 442 (97.4%) patients had a second or other diagnosis for a mental health disorder. A total of 287 patients (63.2%) had used an antipsychotic medication at any time before or after TD diagnosis. Of the 251 patients (55.3%) who used antipsychotic medications before diagnosis of TD, approximately 30% were treated for more than 1 year, and of the 244 patients (53.7%) who used antipsychotic medications after diagnosis of TD, approximately 35% were treated with antipsychotic medications for more than 1 year. Before diagnosis of TD, 84 patients (18.5%) had used a long-acting antipsychotic medication and 32 (7.0%) had used a long-acting antipsychotic medication after TD diagnosis.
Initial TD diagnoses were made most frequently by a neurologist (n = 163, 35.9%) or general physician (n = 141, 31.1%), with fewer diagnoses made by a hospital physician (n = 71, 15.6%), psychiatrist (n = 56, 12.3%), or other provider (n = 23, 5.1%; Fig. 2A). After diagnosis of TD, most patients (n = 386; 85.0%) had 1 or more purchases for a benzodiazepine medication, whereas purchases of tetrabenazine (n = 167, 36.8%) and amantadine (n = 62, 13.7%) were less common (Fig. 2B). Of those who initiated treatment, 142 (85%), 214 (55.4%), and 52 (83.9%) had either permanently or temporarily discontinued tetrabenazine, benzodiazepines, and amantadine, respectively. Throughout the whole disease period, the median (IQR) proportions of disease covered were 9.1% (2.9%–40.8%), 69.3% (18.8%–100.0%), and 7.1% (2.2%–29.8%) for tetrabenazine, benzodiazepines, and amantadine, respectively. The proportion of patients using amantadine, tetrabenazine, and benzodiazepines before and after first TD diagnosis is shown in Figure 2C.
 FIGURE 2:
FIGURE 2: Diagnosis and medication use in the treatment patterns population (n = 454). GP, general physician. The treatment patterns population included all patients with a TD diagnosis who were alive between 2013 and 2018.
Health Care Resource Utilization and CostsFor the analysis of health care resource utilization, 333 patients with TD who were alive on January 1, 2018, were matched with 999 non-TD patients according to year of birth, sex, and underlying psychiatric diagnosis (Table 1). Demographics and disease characteristics were generally similar between these populations; however, the patients with TD had generally lower socioeconomic status, and higher proportions of patients had chronic kidney disease and antipsychotic medication use compared with the non-TD population. A total of 34 patients in the health care resource utilization analyses did not complete the study in 2018 due to death (TD, n = 13; non-TD, n = 21).
TABLE 1 - Baseline Characteristics of the TD and Non-TD Patients Included in the Healthcare Resource and Costs Analyses Population TD Patients (n = 333) Non-TD Patients (n = 999) P* Age in 2018, mean (SD), y 63.6 (17.3) 63.6 (17.3) 0.999 Sex, male, n (%) 124 (37.2) 372 (37.2) Underlying psychiatric disorder, n (%) Schizophrenia 105 (31.5) 315 (31.5) Bipolar disorder 20 (6.0) 60 (6.0) 1 MDD 39 (11.7) 117 (11.7) Other mental health disorder 169 (50.8) 507 (50.8) Socioeconomic status, n (%) Low 85 (25.5) 235 (23.5) Medium 145 (43.5) 347 (34.7) 0.003† High 103 (30.9) 417 (41.7) Cardiovascular disease, n (%) 56 (16.8) 144 (14.4) 0.33 Diabetes, n (%) 92 (27.6) 253 (25.3) 0.448 Hypertension, n (%) 172 (51.7) 505 (50.6) 0.776 Cancer, n (%) 55 (16.5) 138 (13.8) 0.261 Chronic kidney disease, n (%) 154 (46.2) 359 (35.9) 0.001† Antipsychotic medication, n (%) FGA 16 (4.8) 50 (5.0) SGA 100 (30.0) 173 (17.3) FGA and SGA simultaneously 100 (30.0) 102 (10.2) <0.001† FGA and SGA ever 71 (21.3) 86 (8.6) None 46 (13.8) 588 (58.8)*Independent t test for continuous variables and χ2 test for categorical variables.
†P < 0.05.
Compared with patients without TD, those with TD made significantly more visits to the general physician, neurologist, psychiatrist, physiotherapist, and ED (P < 0.05 for all comparisons; Fig. 3). The estimated mean number of hospitalizations per patient per year was higher in the TD than the non-TD population (0.50 vs 0.34 per year) but did not achieve statistical significance; however, the mean length of hospital stay was 6.8 days (95% confidence interval, 6.1–7.6) in hospitalized patients with TD and 4.4 days (95% confidence interval, 4.1–4.7) in the non-TD population (P = 0.003).
 FIGURE 3:
FIGURE 3: Estimated mean number of visits to health care practitioners in patients with and without TD in 2018. *P < 0.05. ***P < 0.0001. Estimated means and significance levels were calculated using generalized linear models with negative binomial with log link distribution. The adjusted model included socioeconomic status, chronic kidney disease at baseline, and antipsychotic medication group.
The mean total health care and medication costs per person were significantly higher in the TD population compared with the non-TD population ($11,079 vs $7145, P = 0.018; Fig. 4A). At least one outpatient visit was made by 324 patients (97.3%) with TD and 966 patients (96.7%) without TD. The mean costs per patient associated with outpatient visits were significantly higher in the TD population compared with the non-TD population ($6613 vs $4498, P < 0.0001; Fig. 4B). Similarly, medications were purchased by 329 patients (98.8%) with TD and 952 patients (95.3%) without TD. The mean costs per patient associated with medication purchases among patients with 1 or more medication purchases were also significantly higher in the TD population compared with the non-TD population ($3206 vs $1859, P < 0.0001). A greater proportion of patients with TD had a hospitalization or ED visit (n = 137, 41.1%) compared with patients without TD (n = 296, 29.6%). However, costs per patient associated with hospitalization or ED visits were similar between groups ($13,548 vs $12,228, P = 0.785). Sensitivity analysis excluding patients with “other mental disorder” alone showed similar results (Supplemental Table 1, https://links.lww.com/JCP/A820; Supplemental Fig. 1, https://links.lww.com/JCP/A823; and Supplemental Fig. 2, https://links.lww.com/JCP/A824).
 FIGURE 4:
FIGURE 4: Health care and medication costs (2018 US dollars). aAnnual costs included the costs from all outpatient clinic visits, hospitalizations, ED visits, and medication purchases during 2018. **P = 0.018. ***P < 0.0001. Significances and estimated means were calculated using generalized linear models with γ distribution with log link distribution. The adjusted model included socioeconomic status, chronic kidney disease at baseline, and antipsychotic medication group.
DISCUSSIONBecause of the debilitating nature of TD and its associated impairment on quality of life, function, and social withdrawal,6 an understanding of the economic burden of TD is imperative to inform future decisions regarding the effective use of health care resources and optimized patient care in this setting. Results from the present analysis demonstrate the significant increase in health care resource utilization and costs associated with the onset of TD in Israel. Overall, visits to the general physician, neurologist, psychiatrist, physiotherapist, and ED were all each significantly higher in patients with TD compared with non-TD patients. In addition, the mean costs of outpatient visits and medication purchases were also higher in the TD population.
Before the current study, data on the burden of TD in Israel were scarce. Findings from this study suggest low awareness of treatment options among patients with TD. Only 37% of TD patients had initiated treatment with tetrabenazine, the only available treatment indicated for TD in Israel at the time of the study, with a median disease coverage of only 9%. This low disease coverage may be due to the high proportion of patients (approximately 85%) who permanently or temporarily discontinued treatment. Potential reasons for treatment discontinuation include resolution of TD, ineffective treatment, or tolerability issues with medication. The chronic and debilitating nature of TD highlights the need for efficacious, well-tolerated, and continuous treatments for these patients, as concerns regarding efficacy or tolerability with available treatments can occur. The impact of increased awareness regarding TD, timely diagnosis, and adherence to treatment on health care resource utilization and costs should also be further investigated.
Several other studies have also reported substantial increases in health care resource utilization and costs associated with the development of TD in the United States.17–19 In a retrospective study of Truven MarketScan commercial and Medicare claims data, Carroll and Irwin17 reported an increase in health care resource utilization in the 12 months after diagnosis of TD compared with the 12 months before a diagnosis of TD (inpatient admissions: 55.5% vs 40.0%, P < 0.001; ED visits: 61.5% vs 54.4%, P = 0.003). Rates of health care resource utilization and costs were also substantially higher in patients with TD after diagnosis compared with propensity score–matched patients without TD, with notable differences in inpatient admissions (55.5% vs 26.1%, P < 0.001) and ED visits (61.5% vs 40.6%, P < 0.001). Total health care and medication costs were $54,656 for patients with TD and $28,777 for those without TD (P < 0.001), which was driven by higher inpatient admissions, outpatient services, and outpatient pharmacy costs in the TD population.17 In a similar claims database analysis using Medicaid claims, patients with TD had significantly more all-cause and mental disorder–related inpatient and ED visits both before and after TD diagnosis compared with matched controls.18 Mental disorder–related outpatient visits were also significantly higher in patients with TD compared with patients without TD in both prediagnosis and postdiagnosis periods. Claims for drugs to treat TD or extrapyramidal symptoms were also higher in cases compared with controls both before and after diagnosis of TD.18 In a retrospective cohort study using electronic health record (EHR) data from the Optum EHR database, patients with TD compared with patients with antipsychotic medication use but no TD had a higher proportion of ED (49.5% vs 40.5%) and inpatient stays (37.3% vs 29.3%).19 Taken together, these studies indicate a significant increase in health care burden associated with a diagnosis of TD compared with patients with mental health conditions who do not have TD within large US-based claims and EHR database populations.17–19
The current analysis also provided some insight into the general characteristics of patients with TD in Israel, including the lower socioeconomic status (as also identified in other studies25) and the higher prevalence of chronic kidney disease compared with non-TD patients with mental illness. It is worth noting that the rate of chronic kidney disease is high in both the TD and non-TD groups (46% and 36%, respectively), potentially related to the similarly high prevalence of diabetes in both groups. The higher prevalence of chronic kidney disease in the TD group might be related to the underlying disease or to increased susceptibility to chronic kidney disease in patients with TD potentially because of increased lithium exposure26 (although lithium exposure was not captured in this analysis, it stands to reason that exposure to lithium may have been greater in the TD group, similar to the observation that antipsychotic agent exposure was greater in the TD group vs the non-TD group), myoglobinuria,27 or other mechanisms. Of note, differences in the baseline prevalence of chronic kidney disease were adjusted for in the analyses. Further studies are needed to explore the relationship between TD and chronic kidney disease, compared with non-TD patients with mental illness. Most diagnoses of TD were made by a neurologist or general physician, and 85% of patients with TD purchased 1 or more benzodiazepine medication after diagnosis. In the current study, patients with and without TD were matched according to age; however, a previous study of patients from Israel noted the older age and longer duration of antipsychotic drug use in patients with TD compared with patients with mental illness and no TD.28
Our study population also has several similarities to patients with TD included in the US claims database analysis by Carroll and Irwin.17 In both studies, the mean age was 63 years, approximately two thirds of patients were female, and most were taking SGAs (60% of patients in the present study were receiving SGAs either alone or in combination with an FGA). However, some differences in the populations were also apparent. In the present study, patients with bipolar disease or MDD comprised 18% of the population with TD, whereas in the study by Carroll and Irwin, these patients made up more than 70% of enrolled patients. In the current study, patients with SCZ comprised 31.5% of the study population, whereas only 18% of the population reported by Carroll and Irwin17 had a diagnosis for SCZ. A previous study using the MHS database reported crude prevalence rates for BP and SCZ of 5 per 1000 individuals and 3 per 1000 individuals, respectively.29
This study has certain limitations. First, we were able to identify TD by ICD-9-CM codes and a self-developed MHS code. However, because of known underdiagnosis and underdocumentation of TD,30,31 we decided not to present the prevalence and incidence rates in this population. The age distribution among MHS members is similar to the general Israeli population; however, membership of MHS is low in non-Jewish cities and relatively high among new immigrants.29 Furthermore, approximately 50% of individuals aged 18 to 21 years in Israel are enlisted in the army and therefore receive medical care from military health care services. As a result, this age group is underrepresented within health maintenance organizations in Israel, such as MHS. Moreover, patients who previously consulted private psychiatrists may not have records in the MHS indicating antipsychotic usage before TD diagnosis. Care should therefore be exercised when generalizing results from the present study to the wider Israeli population. In addition, indirect costs associated with the development of TD were not evaluated; therefore, these results potentially do not capture the full extent of the burden associated with TD. For example, data from the RE-KINECT study indicate that TD places a significant burden on caregiver daily activities, productivity, and ability to socialize.32 These findings also do not account for recent advances in the treatment of TD, notably the approval of vesicular monoamine transporter 2 inhibitors in the United States.33 While these agents have been shown to be clinically effective, it remains to be determined whether their use will impact the associated economic burden. Finally, as with any administrative database analysis, errors in data coding and data entry may impact the results.
In conclusion, the results of this retrospective, claims database analysis extend the current understanding regarding the implications of TD on health care resource utilization in patients with mental illness. These data show that the development of TD is associated with increased health care resource utilization and higher medical costs compared with non-TD patients in Israel. These findings are in broad agreement with previous studies highlighting the burden of TD and may assist clinicians and decision makers to better quantify the burden of TD in Israel.
ACKNOWLEDGMENTSThe authors thank Alaina Mitsch, PhD (Cello Health Communications/MedErgy with funding from Teva Pharmaceuticals) for editorial assistance in the preparation of this manuscript.
AUTHOR DISCLOSURE INFORMATIONY.B. and G.C. are employees of Maccabi Institute for Research and Innovation, which has received payments from Teva Pharmaceutical Industries, Ltd, in relation to this study. R.R., A.Y., R.M., Q.A., and J.L. are employees of Teva Pharmaceuticals. D.A. has received lecturing fees from Teva Pharmaceuticals. R.E. declares no conflicts of interest.
This study was funded by Teva Pharmaceutical Industries, Ltd, Tel Aviv, Israel.
DATA AVAILABILITY STATEMENTThe data sets generated during and/or analyzed during the current study are not available to share for confidentiality reasons. Queries about the data should be directed to the corresponding author.
REFERENCES 1. Ayyagari R, Goldschmidt D, Mu F, et al. An experimental study to assess the professional and social consequences of tardive dyskinesia. Clin Psychopharmacol Neurosci. 2022;20:154–166. 2. Lerner PP, Miodownik C, Lerner V. Tardive dyskinesia (syndrome): current concept and modern approaches to its management. Psychiatry Clin Neurosci. 2015;69:321–334. 3. Jackson R, Brams MN, Citrome L, et al. Assessment of the impact of tardive dyskinesia in clinical practice: consensus panel recommendations. Neuropsychiatr Dis Treat. 2021;17:1589–1597. 4. Jain R, Correll CU. Tardive dyskinesia: recognition, patient assessment, and differential diagnosis. J Clin Psychiatry. 2018;79:nu17034ah1c. 5. Caroff SN, Yeomans K, Lenderking WR, et al. RE-KINECT: a prospective study of the presence and healthcare burden of tardive dyskinesia in clinical practice settings. J Clin Psychopharmacol. 2020;40:259–268. 6. McEvoy J, Gandhi SK, Rizio AA, et al. Effect of tardive dyskinesia on quality of life in patients with bipolar disorder, major depressive disorder, and schizophrenia. Qual Life Res. 2019;28:3303–3312. 7. Ballesteros J, Gonzalez-Pinto A, Bulbena A. Tardive dyskinesia associated with higher mortality in psychiatric patients: results of a meta-analysis of seven independent studies. J Clin Psychopharmacol. 2000;20:188–194. 8. Carbon M, Hsieh CH, Kane JM, et al. Tardive dyskinesia prevalence in the period of second-generation antipsychotic use: a meta-analysis. J Clin Psychiatry. 2017;78:e264–e278. 9. Glazer WM, Morgenstern H, Doucette JT. Predicting the long-term risk of tardive dyskinesia in outpatients maintained on neuroleptic medications. J Clin Psychiatry. 1993;54:133–139. 10. Carbon M, Kane JM, Leucht S, et al. Tardive dyskinesia risk with first- and second-generation antipsychotics in comparative randomized controlled trials: a meta-analysis. World Psychiatry. 2018;17:330–340. 11. McEvoy JP, Kremens DE. Early recognition and treatment of tardive dyskinesia in patients with mood disorders and schizophrenia. J Clin Psychiatry. 2020;81:NU18041AH5C. 12. Zhang W, Amos TB, Gutkin SW, et al. A systematic literature review of the clinical and health economic burden of schizophrenia in privately insured patients in the United States. Clinicoecon Outcomes Res. 2018;10:309–320. 13. Bessonova L, Ogden K, Doane MJ, et al. The economic burden of bipolar disorder in the United States: a systematic literature review. Clinicoecon Outcomes Res. 2020;12:481–497. 14. Caroff SN. Overcoming barriers to effective management of tardive dyskinesia. Neuropsychiatr Dis Treat. 2019;15:785–794. 15. Caroff SN, Mu F, Ayyagari R, et al. Hospital utilization rates following antipsychotic dose reduction in mood disorders: implications for treatment of tardive dyskinesia. BMC Psychiatry. 2020;20:365. 16. Zichlin ML, Mu F, Leo S, et al. The impact of antipsychotic dose reduction on clinical outcomes and health care resource use among Medicare patients with schizophrenia. Clin Drug Investig. 2021;41:853–863. 17. Carroll B, Irwin DE. Health care resource utilization and costs for patients with tardive dyskinesia. J Manag Care Spec Pharm. 2019;25:810–816. 18. McEvoy J, Park T, Schilling T, et al. The burden of tardive dyskinesia secondary to antipsychotic medication use among patients with mental disorders. Curr Med Res Opin. 2019;35:1205–1214. 19. Loughlin AM, Lin N, Abler V, et al. Tardive dyskinesia among patients using antipsychotic medications in customary clinical care in the United States. PLoS One. 2019;14:e0216044. 20. The State of Israel. Characterization and classification of geographic units by the socio-economic level of the population 2008. 2013. Available at: https://www.cbs.gov.il/he/publications/DocLib/2013/1530/pdf/e_print.pdf. Accessed July 14, 2022. 21. Shalev V, Chodick G, Goren I, et al. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int J Cardiol. 2011;152:345–359. 22. Chodick G, Heymann AD, Shalev V, et al. The epidemiology of diabetes in a large Israeli HMO. Eur J Epidemiol. 2003;18:1143–1146. 23. Weitzman D, Chodick G, Shalev V, et al. Prevalence and factors associated with resistant hypertension in a large health maintenance organization in Israel. Hypertension. 2014;64:501–507. 24. Coresh J, Turin TC, Matsushita K, et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA. 2014;311:2518–2531. 25. Patel RS, Mansuri Z, Chopra A. Analysis of risk factors and outcomes in psychiatric inpatients with tardive dyskinesia: a nationwide case-control study. Heliyon. 2019;5:e01745. 26. Van Alphen AM, Bosch TM, Kupka RW, et al. Chronic kidney disease in lithium-treated patients, incidence and rate of decline. Int J Bipolar Disord. 2021;9:1. 27. Lazarus AL, Toglia JU. Fatal myoglobinuric renal failure in a patient with tardive dyskinesia. Neurology. 1985;35:1055–1057. 28. Sabbag R, Fridman B, Heresco-Levy U. Prevalence, severity and characteristics of tardive dyskinesia among schizophrenia patients in an Israeli psychiatric center. Curr Psychopharmacol. 2014;3:79–85. 29. Kodesh A, Goldshtein I, Gelkopf M, et al. Epidemiology and comorbidity of severe mental illnesses in the community: findings from a computerized mental health registry in a large Israeli health organization. Soc Psychiatry Psychiatr Epidemiol. 2012;47:1775–1782. 30. Weiden PJ, Mann JJ, Haas G, et al. Clinical nonrecognition of neuroleptic-induced movement disorders: a cautionary study. Am J Psychiatry. 1987;144:1148–1153. 31. Lohr JB. Commentary: is tardive dyskinesia disappearing? In: Factor SA, Lang AE, Weiner WJ, et al., eds. Drug Induced Movement Disorders. 2nd ed. Malden, MA: Blackwell Publishing; 2005:302–310. 32. Cutler AJ, Caroff SN, Tanner CM, et al. Caregiver-reported burden in RE-KINECT: data from a prospective real-world tardive dyskinesia screening study. J Am Psychiatr Nurses Assoc. 2021;10783903211023565. 33. Solmi M, Pigato G, Kane JM, et al. Treatment of tardive dyskinesia with VMAT-2 inhibitors: a systematic review and meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2018;12:1215–1238.
留言 (0)