
記住我
Alpha-1 antitrypsin deficiency (AATD) is described as an autosomal codominant genetic disorder characterized by a reduction in circulating levels of alpha-1 antitrypsin (AAT) protein. This condition causes a loss of systemic balance between protease and antiprotease, and the lack of a fundamental anti-inflammatory acute-phase factor.1
Alpha-1 antitrypsin is a protein belonging to the family of serine protease inhibitors and is encoded by the Serpina1 gene, whose locus is located on chromosome 14q32.1. Hepatocytes and bronchial epithelial cells mainly synthesize AAT to grant tissue protection and provide a reliable modulation of the inflammatory response through the signal pathway induced by the binding with scavenging receptor LRP1, also known as AAT-Rec. The identification over the years of more than 100 genetic mutations has allowed several allelic variants to be described. Among these, the Z variant resulting from an aminoacidic substitution GLU342LYS has the most severe clinical consequences, affecting especially its synthesis sites with cirrhosis, emphysema, Chronic Obstructive Pulmonary Disease (COPD) and asthma. The Z variant causes the synthesis of a defective form of AAT with a marked tendency to generate precipitating polymer aggregates leading to cellular engorgement and subsequent tissue damage.2,3
In recent decades, research has devoted most of its efforts to finding correlations between AATD and the principal liver and respiratory diseases and in searching for replacement therapies to balance the low serum AAT levels.4–6 However, we cannot ignore that AAT, when released into the bloodstream, carries out its protective and anti-inflammatory action at a systemic level.7 Therefore, it can be considered both an anti-inflammatory acute-phase protein and a useful disease evolution biomarker. For all these reasons, the role of AAT and its deficiency impact on the onset and worsening of local and systemic conditions cannot be overlooked. Among these, vascular ones represented a controversial field, rich in studies reporting conflicting results.
On these bases, this review aims to shed light on the relationship between AATD and vascular pathologies and provide the most up-to-date insights on the topic.
Findings Head and neck district Cervical arteries dissectionsFirst insights into the relationship between AATD and/or low AAT serum levels have been provided in the 2003 case–control study of Vila et al.8 analysing 22 patients with spontaneous cervical artery dissection (sCAD). However, in 2004 and 2005, two case–control studies by Grond-Ginsbach et al.9 and Konrad et al.10 enriched the knowledge in this field with a genetic segregation analysis conducted on larger samples (74 and 80 patients, respectively) that disproved the former hypothesis.
Nevertheless, it is possible to apprehend a general consensus on the protective and anti-inflammatory role of AAT and how its lowering below physiological values contributes to protease-mediated arterial tissue damage.9,10 As further evidence, there is a retrospective study by Schievink et al.11 dated 1994, wherein thickening and disorganization of muscular and connective tissues of the middle tonaca and intimal fibroplasia were reported in samples from individuals with AATD and fibromuscular dysplasia (FMD).
Intracranial aneurysmsThe first reports date back to 1995, when a study by Baker et al.12 compared the elastase:AAT ratio in 19 patients with unruptured intracranial aneurysms and 41 with ruptured aneurysms vs. control. The elastase:AAT ratio was doubled in both the groups compared with controls. However, the higher ratio was primarily related to the increase in elastase levels rather than low AAT levels.12
In the following year, a study by Schievink et al.13 evaluated the prevalence of different AATD phenotypes in 100 patients with intracranial aneurysms. The study documented a higher prevalence of heterozygous and homozygous AATD phenotypes (PiMS, PiMZ and PiZZ) than the general population.13 This was the first study confirming a relationship between AATD and intracranial aneurysms.
Several years later, in 2004, the same hypothesis was overturned by an extended population study conducted by Yoneyama et al.14 Genotyping for seven defective AAT allelic variants in 195 Japanese and 189 Korean individuals affected by ruptured intracranial aneurysm vs. control showed no significant differences.14
In the end, a 2019 work by Tyagi et al.15 studied, through RT-PCR and immunohistochemistry techniques, the expression levels of four genes, including the SERPINA gene, by sampling the vascular wall of 35 patients with intracranial aneurysm. These expression levels have been compared with control levels quantified from the extracranial artery wall of the same subjects. The study documented AAT levels 1.46 times higher than the control, showing how high protease activity in aneurismatic vascular walls increases AAT production. Also, the role of AAT as an acute-phase protein able to counter the proteases/antiproteases imbalance and modulate the subsequent inflammatory processes has been underlined. However, from a pathological perspective, AAT alone cannot prevent aneurysm development or size increase, as the augmented protease levels lead to an irreversible process of vessels’ extracellular matrix (ECM) remodelling.15
StrokeAvailable sources for this condition are few and contradictory. A 2006 work by Burghaus et al.,16 studying 81 white children recovering after a stroke acute phase, documented that AAT concentrations above the 90th age-dependent percentiles were related to a four times increased risk of arterial ischemic stroke (AIS). However, no SERPINA1 alleles genotyping has been conducted in this study. On the basis of these data, AAT could be suggested as a candidate acute-phase biomarker for the AIS onset, but further studies on this topic are needed.
The opposite opinion was provided in 2014 by a comparative work from Moldthan et al.,17 wherein it was documented how therapy with human AAT in mouse models with an induced ischemic stroke condition improved their outcome and had a protective effect against stroke-associated neurodegenerative processes.
Once again, a 2017 commentary by Meschia18 on a study provided the same year by Malik et al.19 focused on AAT as a risk factor for the development of large arteries stroke (LAS). Specifically, they documented a 22% risk increase for LAS development in patients carrying the M1 allelic variant. Following these findings, the author hypothesized that the gene–environment interaction of the M1 variant with cigarette smoke could explain this risk increase. Cigarette smoking is an important risk factor for stroke development and seems to reduce the modulatory AAT activity towards neutrophil elastase.18,19
Finally, a recent study of 2020 by Mahta et al.20 brought some order to this matter. First, the author points out how stroke, by definition, is an extremely heterogeneous clinical condition characterized by different pathogenic mechanisms. Atherosclerotic stroke is the most frequent, and in this picture, AAT plays an important anti-inflammatory and cytoprotective role, capable of slowing down the vascular remodelling processes. Therefore, finding high levels of AAT in individuals affected by stroke could be an acute-phase neuroprotective mechanism to limit acute damage and inflammation of the central nervous system. Another interesting suggestion is the need to identify AAT concentrations suitable for future pharmacological employments to stop vascular remodelling processes and provide valuable preventive therapeutic support.20
Pulmonary and cardiovascular system AneurysmsSimilar to the previously described clinical conditions, there is a very contradictory debate on the role of AAT and AATD in pneumo and cardiovascular diseases. In 2010, a study by Schachner et al.21 showed how AAT serum levels in individuals affected by dissection of the ascending aorta were lower than in healthy individuals, highlighting its protective role against proteolytic damage. Subsequently, in 2012, Vizzardi et al.,22,23 studying a sample of 33 AATD individuals, demonstrated an increased stiffness, reduced distensibility and abnormal strain of the aortic wall, pointing them out as markers of pathological alterations of the elastic tissue. In the same year, a study by Kilickesmez et al.24 related the ascending aorta dilation to AAT and metalloprotease-9 serum levels in individuals with bicuspid aortic valve condition.
Validation of what previously documented was provided by Muhammad et al.25 in 2017 and Fisk et al.26 in 2018, who in an observational study on 2338 individuals and a prospective cross-sectional study on 121 patients (85 with COPD due to smoking, 12 with COPD + AATD and 24 controls equally divided into smokers and nonsmokers), respectively, demonstrated the protective and anti-inflammatory role of AAT as an acute-phase reactant to counter the elastin degradation processes induced by proteases, which in time lead to an increase in aortic stiffness. The documented results made the authors suggest that AAT serum levels quantification could be a useful predictor of aortic dilatation.
The most recent work dates back to June 2021. Dako et al.,27 through a retrospective CT-scan case–control study, analysed the ascending aorta mean diameter of individuals with AATD-related emphysema vs. controls with emphysema alone. A pathological association between AATD and aortic wall distension with a subsequent increased risk for aneurysm development has been documented. At the same time, the author proposed including the measurement of aortic diameter in AATD patients in the diagnostic routine. Conversely, the dosage of AAT levels and eventual genotyping in individuals with aortic wall distension and/or aneurysm has been suggested.27
A 2018 article by Guo et al.28 set out to assess the role played by the imbalance between protease and antiprotease in individuals with idiopathic pulmonary hypertension (IPAH), showing that AAT levels did not differ between individuals with IPAH and controls. However, it should be noted that this study did not focus on AATD individuals but only on the balance assessment of the protease–antiprotease axis in IPAH individuals. Although there is no specific evidence in the literature on the relationship between AATD and IPAH, a 2004 work by Aldonyte et al.29 showed that AAT defective forms, during their polymerization phase, are deposited along the pulmonary vascular endothelium, suggesting that cellular AAT polymers, subsequent cellular and tissue damage, and the loss of inflammatory modulation could be determining factors for IPAH development.
Cardiac diseases, atherosclerosis and cardiovascular riskSeveral studies tried to characterize the AATD impact on cardiac diseases. In 2003, Engström et al.30 documented a correlation between the increase in inflammation-sensitive acute-phase proteins, including AAT, and myocardial infarction in individuals with no cardiovascular risk factors.
Almost 10 years later, the study of Kanai et al.31 on plasma factors potentially involved in the onset and progression of Kawasaki disease identified peaks of AAT, assuming that they could play an important but not mandatory role in protecting vascular epithelial tissues in individuals with Kawasaki disease-related aneurysmatic disease. Confirming this hypothesis, there is a 2015 study by Feng et al.32 wherein AAT is shown to play a cytoprotective role in the vascular endothelium when affected by hypoxia and subsequent reoxygenation processes, thus suggesting that replacement therapies with AAT may limit the damage resulting from the ischemia and reperfusion phases in tissues damaged by myocardial infraction. An empirical demonstration of this hypothesis comes from several studies developed in the following years. In 2015, Abbate et al.33 showed that in 10 patients with ST-segment elevated myocardial infraction (STEMI), infusion within 12 h of hospital admission of AAT 60 mg/kg intravenously (i.v.) combined with conventional therapeutic protocols turned out to be well tolerated and capable of reducing the inflammatory-processes underlying the cardiac event. In 2016, Toldo et al.34 confirmed Feng's theory by applying recombinant human plasma-derived AAT-Fc in murine models with an induced acute myocardial inflammatory injury, proving its property to reduce the size of the ischemic area and preserve the systolic function independently of the previous neutrophil elastase's effects. More recently, in 2018, Abouzaki et al.35 in a post-hoc analysis of Abbate's work, showed that Prolastin C administered hours after myocardial reperfusion reduces the time to peak and the area under the curve for CK-MP compared with controls, suggesting that it can reduce the duration of the injury related to the ischemia-reperfusion in STEMI patients.
Lastly, in 2016, Turhan Caglar et al.36 studied the serum AAT levels in 50 patients with coronary artery ectasia (CAE) and 46 negative controls, demonstrating an inverse relationship, thus confirming the role of AAT in preserving arterial wall integrity.
The principle of the elastase/antielastase imbalance as one of the mechanisms underlying the destructive processes of vascular connective tissue is reiterated in a 2001 work by Stakisaitis et al.37 aimed to assess the role of AAT in individuals affected by coronary atherosclerosis. This work showed how AAT levels in individuals with coronary atherosclerosis were higher than in controls. Therefore, it was concluded that congenital conditions such as hyperlipidaemia or carrying defective allelic AAT forms, such as PiZZ, along with acquired conditions such as ageing or cigarette smoking, correlate with an increased progression of coronary atherosclerosis due to a strong protease/antiprotease imbalance.37
One year later, Dahl et al.38 conducted an important case–control study in which 1131 and 2221 patients enrolled from the Copenhagen City Heart Study and the Copenhagen University Hospital affected by ischemic cerebrovascular disease (ICVD) and ischemic heart disease (IHD), respectively, were evaluated in terms of AAT genotyping, blood pressure measurement and cardiovascular risk assessment and then compared with 7963 adult Danish control individuals to demonstrate whether AATD is associated with a reduction in blood pressure, increased risk for ICVD and IHD, and longevity. Data obtained in this study allowed Dahl et al.38 to state that PiZZ and PiMZ genotypes are related to reduced blood pressure in IHD patients. Also, the PiMZ genotype is associated with a reduced risk for ICVD and IHD.38
In 2003, the abovementioned study by Stakisaitis et al.37 was confirmed by the association analysis performed by Talmud et al.39 Their study proved how coronary disease progression, documented with the minimum luminal diameter measurement, was associated with AAT defective allelic S and Z forms and low serum AAT levels.39 Apart from being a protein capable of slowing the progress of coronary atherosclerosis, the study by Towler40 suggested a new role for AAT as a therapeutic molecule able to reduce the deposition of calcific plaques caused by an increased protease activity.
To conclude, three recent articles produced by Fähndrich et al.,41 Curjuric et al.42 and Nakanishi et al.43 in 2017, 2018 and 2020, respectively, assessed the cardiovascular risk in patients with AATD. Unlike what has been previously documented, Fähndrich et al.41 found a lower prevalence of cardiovascular comorbidities in a registry of 2645 COPD patients. This contrasts with the findings of previous authors. However, it cannot be excluded that patients involved in the study by Fähndrich et al.41 had a lower prevalence of cardiovascular comorbidities due to the lifestyle adaptations implemented for their AATD condition and increased clinical follow-up visits over time.41 Curjuric et al.,42 in turn, using data from the Swiss population-based SAPALDIA cohort (2614 adult individuals), demonstrated a possible association between AAT deficiency and carotid intima-media thickness (CIMT) and arterial hypertension.42 Lastly, Nakanishi et al.43 claimed that PiMZ individuals present a reduced cardiovascular risk.43 It emerges how the data of Fähndrich et al.41 and Nakanishi et al.43 contradict what has been documented by previous authors. However, the role of AAT as a cytoprotective element for coronary vascular walls is undeniable. For this reason, further clinical and molecular biology studies are mandatory to provide more clarity.
Aortic districtDespite some contradictory findings, a considerable number of studies suggest a relationship between AATD and abdominal vascular disease. However, provided data results are contradictory. The first hypothesis dates back to 1988, with a work by Tilson and Roberts,44 but in the 1990s, the interest started to rise.
Two studies by Cohen et al.45 dated 1990 and Schardey et al.46 dated 1998 agree that deficient allelic AAT forms correlate with a higher incidence of abdominal aortic aneurysm (AAA) development than the general population. On the contrary, numerous studies supported the opposite theory, defining AATD alone as a condition unable to develop abdominal aneurysms.47–50 The only work that sought to mediate between these two positions was the 1997 study conducted by Ahlgren et al.51 determining whether there were changes in aortic wall stiffness, assessed by echo-tracking sonography, in 19 men and 17 women with AATD. The study found no significant differences in abdominal aortic wall stiffness compared with control subjects. The only significant evidence was the altered aortic wall distensibility in male subjects as a potential sign of early vascular alteration.51 This finding leads to the hypothesis that AATD vascular effects may occur at the earliest stages of disease, causing vascular wall abnormalities that contribute to the AAA onset along with other risk factors.
The conflicting and often discouraging results led to a progressive lack of interest in this topic. In the 2000s, two articles by Knapik-Kordecka et al.52 and Vega de Céniga et al.53 documented the role of AAT as an independent biomarker of cardiovascular risk during acute inflammation phases, capable of promoting AAA development and growth. At the beginning of the last decade, Pulinx et al.54 confirmed the presence of increased AAT serum levels in patients with AAA, although they did not find a direct correlation with the increase in aneurysmal diameter. Several years after, Pini et al.55 brought back the attention with a study involving 138 patients hospitalized for nontraumatic AAA rupture, documenting a higher prevalence of the S deficient AAT allele compared with the general Italian population, pointing to the AATD condition as a candidate risk factor for AAA development.
Other evidenceRegarding the relationship between AATD and other vascular issues, the study conducted in the 2000s by Gaglio et al.56 demonstrated an increased risk of rupture of splenic artery aneurysms in patients with AATD.
The last field of research that again produced contradictory results is the role of AATD in individuals with FMD of the renal artery. The 2000s study by Bofinger et al.57 suggested that the AATD leads to the development of more severe forms of renal artery FMD. However, 6 years later, Perdu et al.,58 studying polymorphisms associated with PiM1, PiZ and PiS allelic variants, documented no correlation with any FMD form.
Inflammatory and autoimmune diseasesAATD could generate issues at a systemic level, as shown in a work of 1996 by Mazodier et al.59 describing the clinical cases of eight Swedish individuals suffering from AATD and systemic necrotizing vasculitis. Among them, six had systemic vasculitis characterized by microscopic polyangiitis, while the other two were affected by Wegener's granulomatosis and Schonlein-Henoch's purpura, respectively.59
Savige et al.60 in 1995 and Callea et al.61 in 1997 documented how low AAT serum levels are associated with more severe and widespread forms of vasculitis, suggesting that AATD leads to a PR3 protease inhibition impairment and an increase in cANCA production. These data raised reflections on the usefulness of AAT as a screening biomarker in individuals with cANCA-positive vasculitis and vice versa.
These findings generated a growing interest in the scientific community. Since the mid-1980 s, an increasing number of dedicated studies can be found. Among these, a 1985 study by Wakefield et al.62 on a sample of 25 patients attempted to correlate AATD with the onset and/or progression of retinal vasculitis. Although unsuccessful, the study still documented increased AAT levels during acute retinal vasculitis phases.62 A later 2001 work by Audrain et al.63 in a population of 191 PiZZ patients vs. PiMM controls reported an increased ANCA, although not directed against the MPO and PR3 antigens. Therefore, the author emphasized the role of AATD only as an additional condition able to contribute to the onset of ANCA-positive vasculitis.
The open perspectives in this field are numerous and highly diversified. There is still much to discover about the role played by the AATD in autoimmune diseases and even more about its impact on small and medium vessels, whose response may differ from what is already known for the large ones.
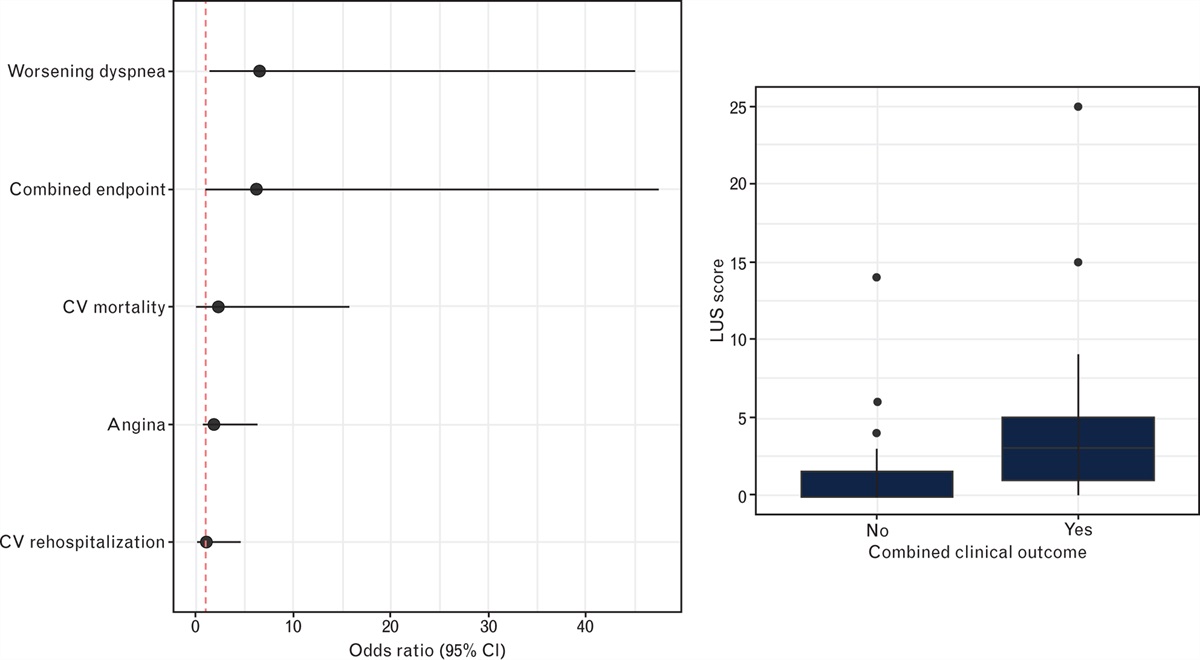
DiscussionData from the literature mainly documented vascular alterations in individuals with AATD, especially PiZ ones. However, overall, the results proved to be highly contradictory. A few statistically significant correlations between AATD and vascular diseases have been documented, even rarely with a direct cause–effect association (Table 1 and Fig. 1).
Table 1 - Literature evidence on the relationship between alpha 1-antitrypsin deficit and/or changes in alpha 1-antitrypsin serum levels and major vascular and autoimmune diseases Year Ref. Evidence Cervical artery dissection 2003 Vila et al. 8 ↑ Risk in AATD 2004 Grond-Ginsbach et al. 9 No evidence 2005 Konrad et al. 10 No evidence Fibromuscular dysplasia 1994 Schievink et al. 11 ↑ Risk in AATD Intracranial aneurysms 1995 Baker et al. 12 Elastase/AAT ratio doubled 1995 Schievink et al. 13 ↑ Risk in AATD 2004 Yoneyama et al. 14 No evidence 2019 Tyagi et al. 15 ↑ AAT levels Stroke 2006 Burghaus et al.16 Four times higher risk in patients with↑ AAT levels 2014 Moldthan et al. 17 Improved outcome with AAT replacement therapy 2017 Meschia18 ↑ Risk in M1 variant + cigarette smoking 2020 Mahta et al. 20 AAT anti-inflammatory and cytoprotective role Aortic aneurysms 2010 Schachner et al. 21 ↓ AAT levels in pts with Ascending Aorta Dissection 2012 Vizzardi et al. 22,23 ↑ Aortic stiffness 2012 Kilickesmez et al. 24 Ascending aorta dilation related with AAT and MP9 levels 2017 Muhammad et al. 25 AAT as an acute-phase reactant 2018 Fisk et al. 26 AAT as an acute-phase reactant 2021 Dako et al.27 ↑ Risk in AATD Idiopathic pulmonary hypertension 2004 Aldonyte et al. 29 Defective AAT polymers in pulmonary vascular endothelium 2018 Guo et al. 28 No evidence Myocardial infraction 2003 Engström et al. 30 ↑ AAT levels in patients with myocardial infraction 2015 Feng et al. 32 Improved outcome with AAT replacement therapy 2015 Abbate et al. 33 Improved outcome with AAT replacement therapy 2016 Toldo et al. 34 Improved outcome with AAT replacement therapy 2016 Turhan Caglar et al. 36 AAT as an arterial wall protector 2018 Abouzaki et al. 35 Improved outcome with AAT replacement therapy Kawasaki disease 2012 Kanai et al. 31 ↑ AAT levels in patients with Kawasaki disease Coronary artherosclerosis 2001 Stakisaitis et al.37 ↑ Risk in AATD 2002 Dahl et al. 38 PiZZ and PiMZ had ↓ BP in IHD patients 2003 Talmud et al. 39 ↑ Coronary disease progression and ↓ AAT levels in PiS and PiZ patients 2015 Towler40 AAT reduces calcific plaques deposition Cardiovascular risk 2017 Fähndrich et al. 41 ↓ prevalence of CV comorbidities in AATD patients 2018 Curjuric et al. 42 Association between AATD and CIMT 2020 Nakanishi et al. 43 ↓ CV risk in PiMZ individuals Abdominal aortic aneurysms 1997 Ahlgren et al.51 Early vascular alteration in AATD male patients 1998 Cohen et al. 45 ↑ Risk in AATD 2000 Knapik-Kordecka et al. 52 AAT levels as marker for AAA 2000 Vega de Céniga et al.53 AAT levels as marker for AAA 2011 Pulinx et al.54 AAT levels as marker for AAA 2021 Pini et al. 55 ↑ Risk in AATD PiS Splenic artery aneurysms 2000 Gaglio et al. 56 ↑ Risk in AATD Renal artery FMD 2000 Bofinger et al. 57 ↑ severe FMD forms in AATD patients 2006 Perdu et al. 58 No evidence Vasculitis 1995 Savige et al. 60 Worse vasculitis forms in AATD patients and/or ↓ AAT levels 1996 Mazodier et al. 59 Systemic necrotizing vasculitis in AATD patients 1997 Callea et al. 61 Worse vasculitis forms in AATD patients and/or ↓ AAT levels Retinal vasculitis 1985 Wakefield et al. 62 ↑ AAT levels in patients with RV 2001 Audrain et al.63 ↑ ANCA production in PiZZ patients Fig. 1:
Fig. 1: Overview of the main vascular diseases examined.
Still, it is undeniable that AAT acutely modulates cellular damage and vascular tissue inflammation caused by the increased expression levels in protease factors, especially neutrophil elastase. The mechanisms underlying the AATD condition, such as the presence of constant subacute tissue inflammation, due to the lowering or loss of AAT as an anti-inflammatory factor, together with the elastase/antielastase imbalance, and the defective AAT polymers intracellular deposition, unavoidably lead to progressive degeneration of the arterial vascular walls, increasing their thickness, reducing elasticity, enhancing the deposition of calcific endothelial plaques and altering the overall cellular intima and media tonaca organization (Fig. 2). For these reasons, we can assume that AATD alone is not a sufficient cause for the new onset of vascular diseases, but it mainly acts as a cofactor.
 Fig. 2:
Fig. 2: Main mechanisms of tissue damage in individuals with alpha 1-antitrypsin deficit.
Ultimately, we cannot exclude the possibility that primary AATD consequences in the lungs and liver could indirectly impact preexisting vascular conditions. However, in this field, further targeted studies are needed.
This review suggests that AATD could be considered among the several clinical conditions able to contribute to the onset of inflammatory processes and vascular epithelium structural alteration. Another topic is the high heterogeneity of the vascular diseases in which AATD can be implicated. It is impossible to exclude the AATD contribution in tissue or organ alterations from the largest vessels to the lowest branches. In this context, more refined characterizations of the AAT role within molecular dynamics and pathological vascular mechanisms should be encouraged.
Similarly, from a clinical perspective, screening for AATD by serum AAT dosage and genotyping could be an important screening and monitoring tool in patients requiring surgical procedures or long-term follow-up for vascular diseases. On the contrary, screening ultrasound for the most frequent vascular disorders could be considered in patients affected or with a positive familial clinical history of AATD.
ConclusionNowadays, the role played by AATD in vascular diseases attracts little interest in the scientific community. The low disease frequency in the general population and conflicting results from various literature data have prevented a clear relationship between AATD and vascular disorders. Therefore, research has been directed mainly at the hepatic and pulmonary area, where the evidences are more defined and promising. In this picture, a dedicated meta-analysis would be very informative to provide clarity and, therefore, should be encouraged.
Nevertheless, there is still a large lack of knowledge on this topic. This review showed that AATD, combined with other risk factors, enhances the progression of both cardiovascular and autoimmune disorders. Therefore, it would be useful to investigate the molecular mechanisms of vascular AATD-related damage. Moreover, new insights could be provided by promoting prevalence studies in high cardiovascular risk populations or those affected by autoimmune vascular diseases and vice versa.
Another issue worthy of investigation, often proposed in various clinical studies over the years, is the putative introduction of AAT serum dosage and genotyping for screening and/or interventional purposes to proactively set replacement therapies aimed at reducing the risk of short- and long-term vascular and surgical complications and slowing their progression.
Conflicts of interestThere are no conflict of interest.
References 1. Kelly E, Greene CM, Carroll TP, McElvaney NG, O’Neill SJ. Alpha-1 antitrypsin deficiency. Respir Med 2010; 104:763–772. 2. Janciauskiene S, Welte T. Well known and less well known functions of alpha-1 antitrypsin: its role in chronic obstructive pulmonary disease and other disease developments. Ann Am Thorac Soc 2016; 13: (Suppl 4): S280–S288. 3. Pini L, Tiberio L, Arici M, et al. Z-alpha 1-antitrypsin polymers and small airways disease: a new paradigm in alfa-1 antitrypsin deficiency-related COPD development? Monaldi Arch Chest Dis 2021; 91:489–493. 4. Pini L, Paoletti G, Heffler E, et al. on behalf of Asthma and Alpha 1-Antitrypsin Research Group. Alpha 1-antitrypsin deficiency and asthma. Curr Opin Allergy Clin Immunol 2021; 21:46–51. 5. Pini L, Tiberio L, Venkatesan N, et al. The role of bronchial epithelial cells in the pathogenesis of COPD in Z-alpha 1 antitrypsin deficiency. Respir Res 2014; 15:112. 6. Maren
留言 (0)