Background
Atrial fibrillation catheter ablation (AFCA) should be considered as a strategy to avoid pacemaker (PM) implantation for patients with bradycardia–tachycardia syndrome (BTS), but lack of evidence is remarkable.
Methods
Our aim was to conduct a random-effects model meta-analysis on safety and efficacy data from controlled trials and observational studies. We compared atrial fibrillation (AF) recurrence, AF progression, procedural complication, additional procedure, cardiovascular death, cardiovascular hospitalization, heart failure and stroke in patients undergoing AFCA vs. PM implantation.
Results
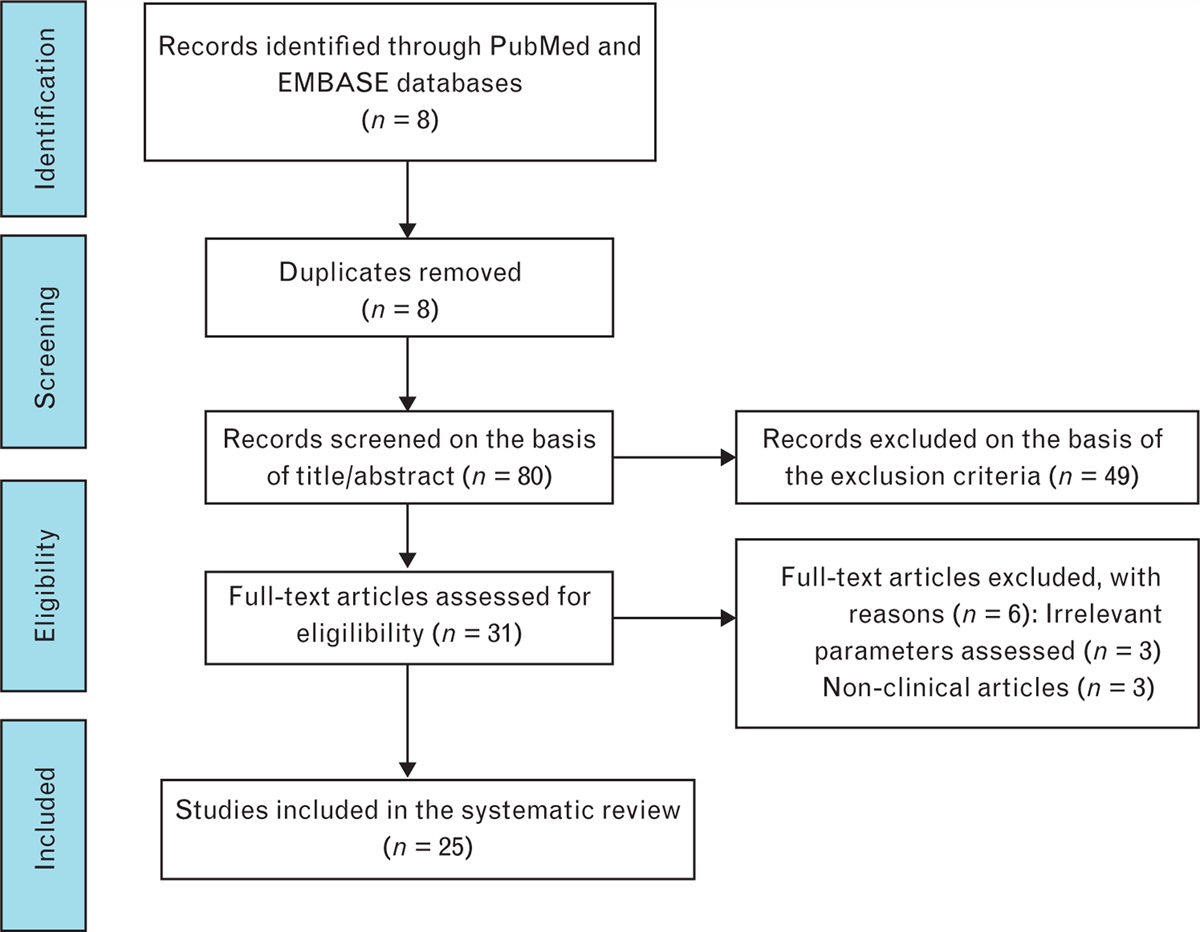
PubMed/MEDLINE, Cochrane Database and Google Scholar were screened, and four retrospective studies were selected. A total of 776 patients (371 in the AFCA group, 405 in the PM group) were included. After a median follow-up of 67.5 months, lower AF recurrence [odds ratio (OR) 0.06, confidence interval (CI) 0.02–0.18, I2 = 82.42%, P < 0.001], AF progression (OR 0.12, CI 0.06–0.26, I2 = 0%, P < 0.001), heart failure (OR 0.12, CI 0.04–0.34, I2 = 0%, P < 0.001), and stroke (OR 0.30, CI 0.15–0.61, I2 = 0%, P = 0.001) were observed in the AFCA group. No differences were observed in cardiovascular death and hospitalization (OR 0.48, CI 0.10–2.28, I2 = 0%, P = 0.358 and OR 0.43, CI 0.14–1.29, I2 = 87.52%, P = 0.134, respectively). Higher need for additional procedures in the AFCA group was highlighted (OR 3.65, CI 1.51–8.84, I2 = 53.75%, P < 0.001). PM implantation was avoided in 91% of BTS patients undergoing AFCA.
Conclusions
AFCA in BTS patients seems to be more effective than PM implantation in reducing AF recurrence and PM implantation may be waived in most BTS patients treated by AFCA. Need for additional procedures in AFCA patients is balanced by long-term benefit in clinical end points.

留言 (0)