
記住我










We thank Dr Buckley1 for the interest in our report on interleukin-6 receptor blockade with subcutaneous tocilizumab in patients with severe COVID-19 pneumonia receiving supplemental oxygen without mechanical ventilation and hyperinflammation.2 We acknowledge that the recently published results from the RECOVERY trial showed reduced mortality in patients treated with dexamethasone (6 mg daily up to 10 days) in addition to usual care, with the benefits being greater in critically ill patients receiving mechanical ventilation (41% vs 29%), while considerably reduced in severe patients on supplemental oxygen without mechanical ventilation (18% vs 14%).3 We also read with interest the results of the CHIC study showing that high-dose intravenous tocilizumab (8 mg/kg body weight, single infusion) may increase the benefits of high-dose methylprednisolone (250 mg on day 1, followed by 80 mg on days 2–5) in patients with severe COVID-19 pneumonia and cytokine storm syndrome requiring supplemental oxygen, mostly through nasal cannulas or mask.4 It is therefore of utmost importance to determine whether the combination of systemic corticosteroids and another anti-inflammatory drug such as tocilizumab may further improve outcomes in selected patients with COVID-19.
Although answering this clinical question was beyond the purpose of our study, we conducted a post hoc analysis to assess whether the benefits observed with subcutaneous tocilizumab (324 mg, given as two simultaneous 162 mg doses) may be attributable to concurrent corticosteroid treatment in the subgroup of patients with severe COVID-19 and hyperinflammation receiving both drugs.2 In our study, corticosteroid use was defined as intravenous administration of methylprednisolone 20 mg or 40 mg twice daily for ≥1 day during hospitalisation. Corticosteroids were prescribed after tocilizumab in all patients who received both drugs in the tocilizumab plus standard of care group. A total of 49 (61.25%) patients received corticosteroid treatment, 26 (65.0%) in the tocilizumab plus standard of care group and 23 (57.5%) in the standard of care only group. Overall, corticosteroid therapy was associated with an increased mortality (log-rank Mantel-Cox χ2 5.918, p=0.015). When stratifying patients according to corticosteroid use, subcutaneous tocilizumab was associated with reduced mortality in the stratum on corticosteroid therapy (log-rank Mantel-Cox χ2 8.445, p=0.004) (figure 1A), and not in patients who did not receive corticosteroids (figure 1B), suggesting that the combination of corticosteroids and tocilizumab may increase the clinical benefits observed in the tocilizumab plus standard of care group.
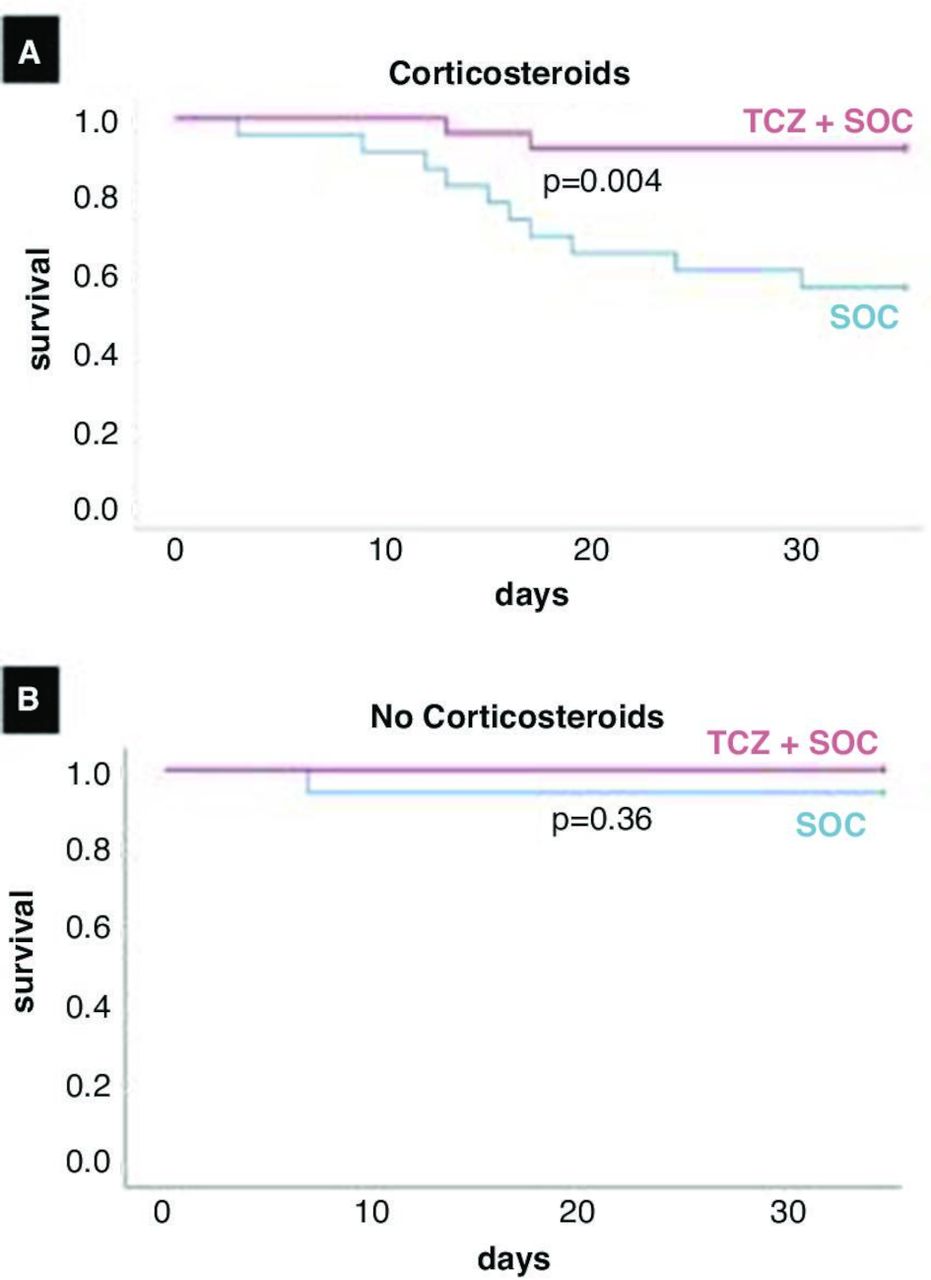 Figure 1
Figure 1 Survival in patients treated with tocilizumab stratified according to corticosteroid use. Patients receiving tocilizumab (TCZ) on top of standard of care (SOC) were significantly less likely to die than patients treated with SOC only matched for sex, age and severity of illness in the stratum on corticosteroids (A), log-rank Mantel-Cox χ2 8.445, p=0.004), and not in patients who did not receive corticosteroids (B).
It is however worth pointing out that corticosteroids were administered at higher dosage in the CHIC study4 as compared with the RECOVERY3 trial and our case–control study,2 and a high-dose corticosteroid administration may exert different clinical effects in patients with COVID-19, including an immunosuppressive rather than anti-inflammatory only activity. Furthermore, in contrast with our study, tocilizumab was administered intravenously at higher dosage in the CHIC study,4 with a different pharmacokinetic and pharmacodynamic profile and possibly different clinical response. Whether the difference in the route of administration and dosage of tocilizumab is clinically relevant is still unclear, and randomised controlled trials exploring both therapeutic regimens are ongoing.
Notwithstanding the many limitations of our study including the small sample size, the non-random allocation of comparisons, the heterogeneous dose and timing of concomitant corticosteroid treatment, our data, consistently with other reports,4–6 suggest that subcutaneous tocilizumab may be considered a safe and beneficial therapeutic option for selected subgroup of patients with COVID-19 pneumonia and hyperinflammation in combination with corticosteroids.
Ethics statementsPatient consent for publicationAcknowledgmentsWe thank Giulia Rizzo, Matteo La Vella and Leonardo Pieramati for their appreciable help in data collection. We thank all patients who agreed to participate to the study and our first-line colleagues who incessantly worked to contain the COVID-19 pandemic.
留言 (0)