
記住我



Our primary aim is to evaluate if a group intervention based on CBT-I is feasible in a regular psychiatric outpatient clinic for patients with depression, bipolar disorder, anxiety disorder and PTSD. Our second aim is to investigate if symptoms of insomnia, depression and anxiety improve after treatment.
DesignThis is an uncontrolled treatment feasibility study with 17 participants. Feasibility measures were collected throughout the recruitment and treatment process. Symptoms of insomnia, depression and anxiety were assessed pre – and post treatment. Insomnia severity was also assessed at three-month follow-up.
Participants and recruitmentThe study included 17 adult patients at a psychiatric out-patient clinic in Stockholm, Sweden, serving patients with affective and anxiety disorders and/or PTSD. In addition to these diagnoses, a notable minority of patients at the clinic have comorbid conditions like ADHD, autism, substance use disorder or personality disorder.
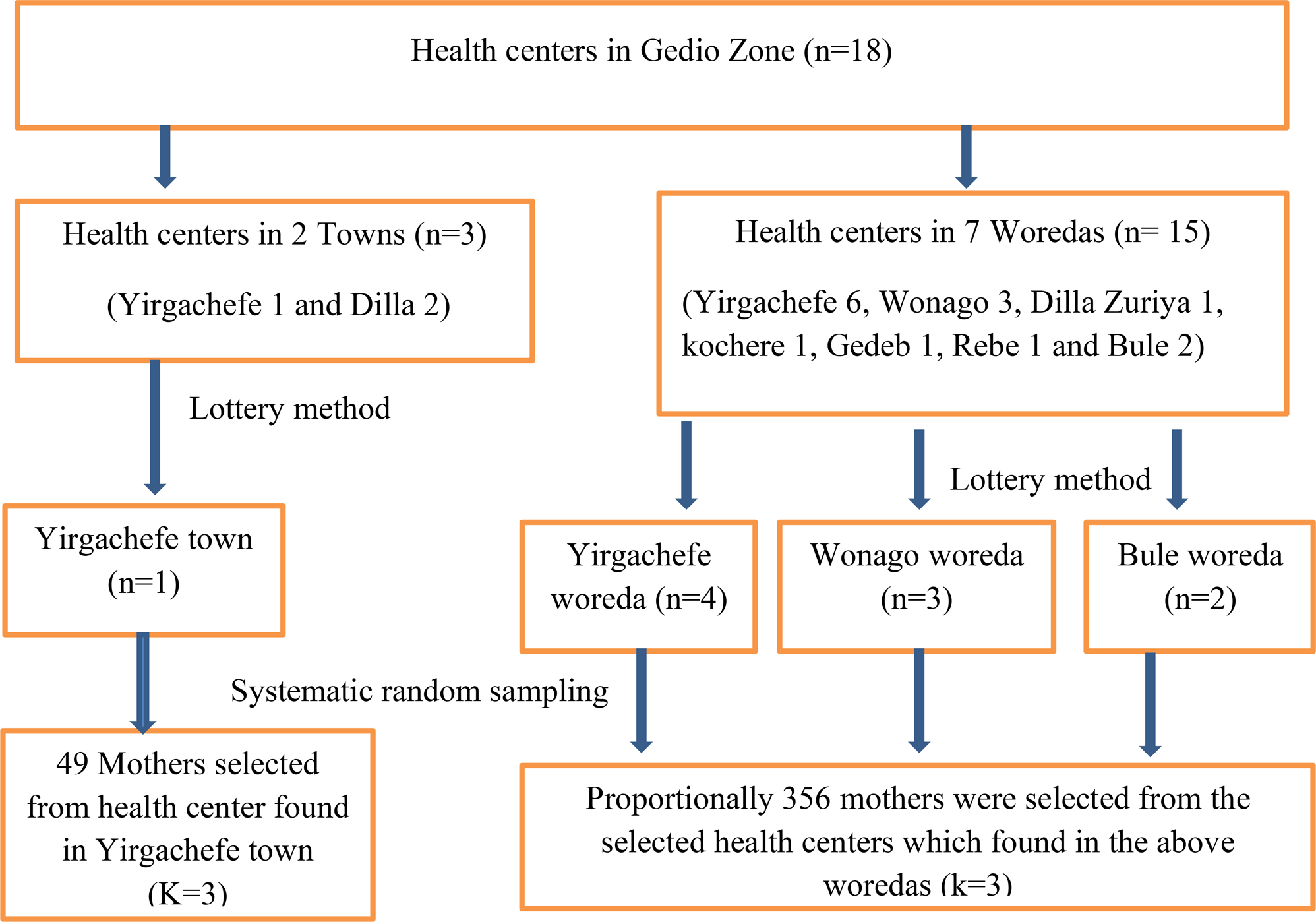
Inclusion criteria for the study were self-reported difficulties initiating or maintaining sleep, Insomnia Severity Index (ISI) score > 10, indicating clinical insomnia [25], sufficient knowledge in Swedish and no practical barriers to participate in the group treatment. Exclusion criteria was night shift work and ongoing alcohol or drug abuse that require treatment at a specialised unit. Information about the study was posted in the waiting room and in psychoeducational group meetings, along with registration forms. Patients could also be referred by their doctor, psychologist, or nurse. Patients interested in participating received written information about the treatment and were contacted by telephone for a short interview to assess inclusion- and exclusion criteria. All patients who were interested in the treatment and fulfilled inclusion criteria received treatment. Those not consenting to participate in the study but wanting to participate in the treatment still received the treatment within regular care and some feasibility measures could still be used for those patients, but self-report data is not available. For participant flow, please see Fig. 1.
Fig. 1
Participant flow through study
Patient feasibility measures were collected throughout recruitment, treatment, and follow-up. Therapist feasibility measures were collected post treatment.
TreatmentThe treatment consisted of six group sessions (four to eight participants; first two sessions 120 minutes, the following 90 minutes) led by two therapists. It was based on well-established CBT techniques for insomnia, including sleep-restriction, stimulus control, sleep hygiene, cognitive techniques and relaxation [26]. The content was adapted to the psychiatric patient group in several ways. First, scheduled sleep with the option of sleep compression was introduced as an alternative to sleep restriction. Although the evidence base for sleep compression is far behind that of sleep restriction, in later years it has been suggested as a more gentle method, with fewer adverse events, that can be considered when treatment has to be modified according to patient needs [27]. To enhance treatment adherence, patients were allowed to choose freely between sleep restriction, and scheduled sleep with the option of sleep compression. Patients with bipolar disorder were instructed to choose scheduled sleep in order to avoid sleep deprivation that might trigger hypomania or mania [28]. For patients who chose sleep restriction, a sleep window was set to average total sleep time based on 1 week of sleep diary data. Patients who chose scheduled sleep were instructed to set their sleep window based on estimated sleep need. If they did not know, they were advised to choose a sleep window of 7–7,5 hours since this is suggested to be optimal sleep duration for adults [29]. Time of awakening was set individually based on the patient’s daily schedule or, if possible, patient preference. Sleep schedule was changed weekly based on sleep diary data, adding 15 min by going to bed earlier if sleep efficiency (SE) was > 85; held constant if 80 < SE > 85; and shortened by 15 min by going to bed later if SE < 80. Patients with a mean total sleep time of less than 5 h were instructed to choose sleep compression and use it together with stimulus control if unable to sleep. Second, instructions for stimulus control were slightly adjusted. Instead of giving the instruction of going to bed only when sleepy, patients were instructed to follow their sleep window. If not being able to fall asleep or if they woke up during the night, they were instructed to leave the bed for 15–20 minutes and then go back and try to fall asleep again. This was to minimize the risk of patients engaging in arousing activities that could interfere with sleep and because some patients have a high level of arousal that makes it difficult for them to notice sleepiness. Third, interventions aiming to stabilize circadian rhythm were added, including systematic use of light and darkness, i.e. light exposure in the morning (e.g. draw the blinds and turn on the lights when waking up, take a morning walk, and dim lights at night for evening chronotypes and the opposite for morning chronotypes), as well as regular meals and wake-up and wind-down routines [30, 31]. Fourth, psychoeducation included information on sleep and psychiatric disorders. Detailed information of treatment content can be found in Table 1.
Table 1 Treatment contentTo facilitate therapist treatment adherence, all sessions had a power-point presentation with a manuscript for each slide. At the end of each session, patients received a booklet with a summary of session content and all worksheets for the session. The booklet was also sent home to patients who did not attend the session.
TherapistsA total of four therapists from the regular staff acted as group leaders. Two of them were licensed psychologists, one a psychologist in training and one a psychiatrist, all with at least 18 months of training in CBT and with additional training in CBT-I. The therapists had access to supervision on demand by last author SJ.
Outcome measuresTreatment feasibilityFeasibility was measured in several ways related to uptake, attendance, and acceptability. The feasibility criteria were formulated in collaboration with staff at the clinic and reflect their view on what criteria a treatment should meet to be considered feasible in the real-world clinical setting.
Patient related feasibility criteria, collected throughout recruitment and treatment process
Number of patients interested in the treatment after given information is sufficient to start at least one group per semester (i.e., around eight).
At least 50% of included patients attend the first session
Patients attend on average at least three out of six sessions
Treatment drop-out, defined as attending less than three sessions in total, is below 50%
All four patient-related feasibility measures were registered for all patients, also patients who did not participate in the study.
Therapist related feasibility measures, collected after all treatment groups included in the study had ended treatment.
Therapists find the treatment manual credible, assessed by semi-structured interviews
Therapists want to continue using manual after end of study, assessed by semi-structured interviews
Symptom of insomniaSymptoms of insomnia were measured using the Insomnia Severity Index (ISI) at pre-, post-, and three-month follow-up. The ISI is a 7-item self-report scale that assesses symptoms of insomnia. It has adequate psychometric properties and is sensitive to change [32]. Each item is scored on a 0–4 scale, total score ranging from 0 to 28, higher score representing a higher degree of symptoms. A cut-off score of 10 indicates probable insomnia in a community sample [25]. Levels of insomnia severity were defined as: 0–7 points: no clinically significant insomnia, 8–14 points: sub-threshold insomnia, 15–21 points moderate insomnia, 22–28 points: severe insomnia [25].
Symptoms of depressionPatient’s health questionnaire-9 (PHQ-9) was administered at pre – and post-treatment. The PHQ-9 is a 9-item self-report scale with good psychometric properties, which assesses each of the nine DSM-5 diagnostic criteria of depression on a 0–3 scale, total score ranging from 0 to 27. A higher score represents a higher level of depression symptoms. Depression severity was defined according to Kroenke as minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19) or severe depression (20–27) [33].
Symptoms of anxietyGeneralised anxiety disorder scale 7 (GAD-7) was administered at pre – and post-treatment. The GAD-7 is a reliable and valid 7-item self-report scale used as a tool for screening for GAD with 10 points recommended as cut-off score for likely generalized anxiety disorder [34]. In an outpatient setting for patients with anxiety and affective disorders, high scores mirror general distress and negative affect in patients [35]. Each item is scored on a 0–3 scale, total score ranging from 0 to 21. A higher score represents a higher level of symptoms. Levels of anxiety were defined as mild (5–9), moderate (10–14) and severe (15–21) [34].
Power considerationsBased on previous research on CBT-I for patients with psychiatric disorders, within-group effect size on the secondary outcome measure ISI, was estimated to Cohen’s d = 1.0 [36, 37]. To achieve a power of 80% with an alpha-level of 0.05, 16 participants were needed. Since attrition was expected, we aimed for 20 participants. This number of patients was also deemed to be enough to evaluate the primary outcomes related to feasibility.
Data handling and statistical analysisFeasibility data is reported descriptively.
Statistical analysis was made using Jamovi, version 1.6.23 [Computer Software]. Retrieved from https://www.jamovi.org.
Data was screened for normality using the Shapiro Wilks test, and no data violated the assumption of normality.
One participant was missing one individual item from one assessment point for the GAD-7. This item was imputed using the corrected item mean substitution [38].
Changes in continuous data from pre- to post-treatment was analysed with dependent t-test, in a per protocol analysis, including those patients who had completed at least three out of six sessions, since this dose could render an effect on insomnia severity. The within-group effect size was calculated on observed data and is reported as Cohen’s d with 95% confidence intervals [39]. Pooled SD was used as denominator: (SDpre+SDpost)/2. Sensitivity analyses were performed using dependent t-tests with last observation carried forward (LOCF) for participants with pre- but not post-data.
Differences in severity levels for insomnia, depression and anxiety were analysed with Wilcoxon signed ranks test on observed data at pre- and post-treatment.
Due to high attrition at three-month follow-up, no statistical tests were performed on follow-up data, but results are presented numerically and graphically.
留言 (0)