Study SampleHCPs
Interviews with HCPs were conducted between June 26 and August 18, 2020. Of the 18 HCPs invited to participate, 7 HCPs were recruited, including 5 neurologists, 1 nurse, and 1 nurse practitioner. The providers reflected geographic diversity across Canada, with two HCPs practicing in Quebec, two in Ontario, two in British Columbia, and one in Alberta. Experience in treating patients with MS ranged from 5 to 30 years (Table 1).
Table 1 Consulting HCP demographicsPatients
Interviews with 12 patients with RRMS were conducted between August 17 and December 1, 2020. Interviews were conducted in French (n = 4) and English (n = 8). The mean age of patients was 42 years, with nine identifying as female. The entire patient sample identified as Caucasian/white. All patients were recruited from three provinces: Quebec, Ontario, and British Columbia (Table 2).
Table 2 Patient demographic and clinical characteristicsMost patients reported their MS severity as “mild disability” per the Patient Determined Disease Steps (PDDS) instrument [30]. The time since diagnosis ranged from 33 to 264 months with the average time being 129 months (11 years). Most patients were taking DMF (n = 8), with two patients on teriflunomide and fingolimod, respectively. All patients had been taking their oral DMT for a year or longer; none had discontinued their oral DMT (Table 2).
HCP and Patient Perspectives on Oral DMT Treatment for RRMSHCP Perspectives
Health care providers perceived oral DMTs as a “major advance” in the treatment of MS, reporting that these therapies encourage patients to consider treatment earlier than they may have otherwise. Providers also observed that oral DMTs increased adherence, noting that patients valued being able to travel without needing to make special accommodations for their medication regimen. According to the HCPs, both factors contributed to patients’ willingness to try these therapies and to adhere to the DMTs once initiated. HCPs reported that both they and their patients found oral DMTs to be efficacious, and this was central to their appreciation for the treatment and their willingness to tolerate side effects to continue taking the medication.
HCPs explained that each of the oral DMTs available in Canada has positive and negative attributes to consider when determining the best treatment option for an individual patient. Five HCPs described taking patients’ GI-related comorbidities into account when prescribing DMF, noting that they would not choose this treatment for patients who had a predisposition to gastrointestinal problems. Fingolimod and teriflunomide were generally viewed as better tolerated overall, although some HCPs stated that treatment failure (more relapses) was more likely with teriflunomide than other available DMTs. HCPs reported that both they and their patients appreciated that DMF could be discontinued quickly without negative consequences such as rebound effects or the need for washout periods.
When asked what they and their patients specifically disliked about DMF, providers reported that the main patient complaints centered around GI-related symptoms, including diarrhea, nausea, vomiting, abdominal pain, and cramping. HCPs stated that diarrhea was consistently reported as the most common symptom from patients, and potentially the most noticeable and bothersome due to its impact on day-to-day functioning.
There was no HCP consensus on whether patients experienced these symptoms singly (e.g., only diarrhea) or in clusters of symptoms (e.g., nausea and abdominal cramping). Nor was there a consensus on which GI-related symptom or group of symptoms was most likely to cause patients to discontinue oral DMTs; even so, diarrhea, nausea, vomiting, and abdominal pain were all cited as likely causes. Providers stated that patient education, support, and expectation management are key to helping patients adhere to an oral DMT regimen when facing symptomatic AEs such as GI issues during dose titration.
Patient PerspectivesGI Symptomatic Adverse Events Associated with DMT Treatment
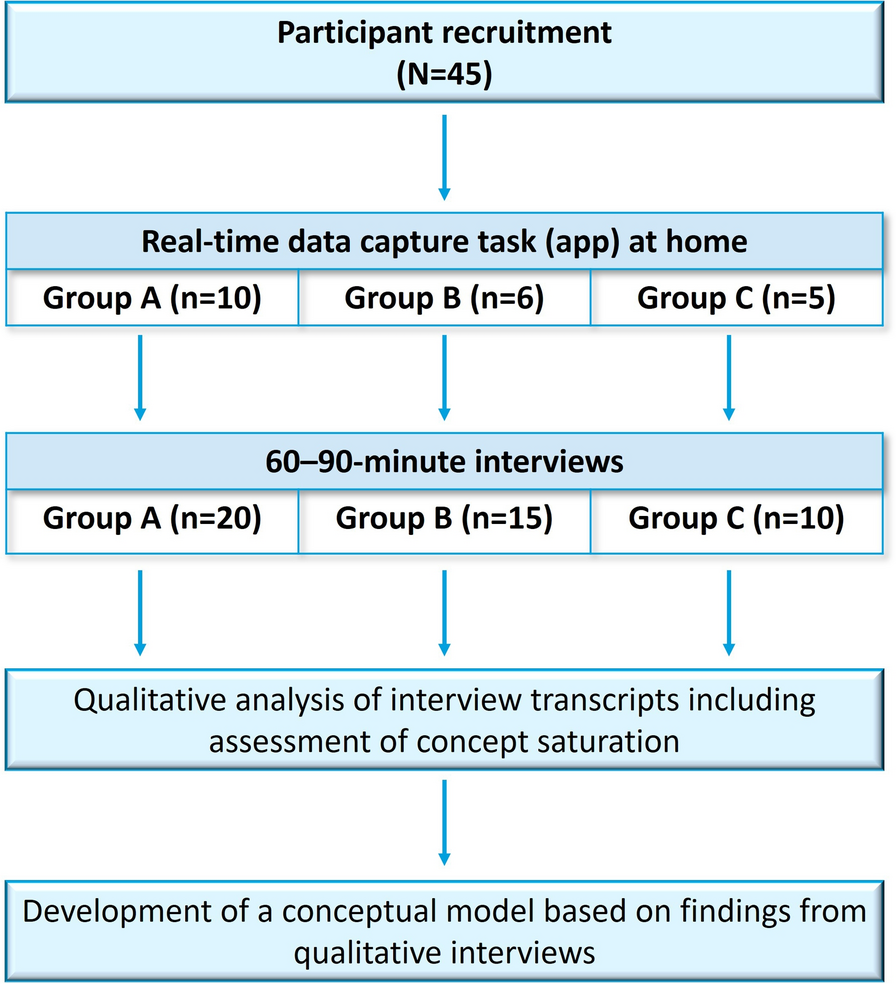
Participants reported 16 unique GI symptom-related codes, with most symptom concepts (12/16 or 75%) reported by more than one patient. The most commonly reported symptoms were diarrhea, indigestion, and nausea; all three of these symptoms were reported by nine patients. Gas was not spontaneously reported by any patients; however, once probed, nine patients endorsed this symptom. Table 3 summarizes the emergence of symptom concepts across the 12 patient interviews conducted, illustrating the achievement of conceptual saturation. All GI-related concepts reported in HCP interviews were also reported in this patient sample; no additional GI-related concepts emerged from patient interviews.
Table 3 Saturation analysis—Number of newly emerged concepts by interview groupThe GI-related symptoms reported were similar across all three oral DMTs. There were no clear differences in types of symptoms reported between patients in different provinces, though this is descriptive data only and these findings should be interpreted cautiously given the small sample size (See Supplemental Materials).
Positive Considerations of Oral DMTs
While patients acknowledged the negative impact of GI-related adverse events, most characterized the overall oral DMT experience as positive, focusing on the perceived efficacy of the treatment in terms of lack of MS relapse, slowed progression of disease, and improvement in MS symptoms. Participants also described aspects of oral administration that they liked, including the simplicity, a feeling of more control and a less restrictive medication schedule, and appreciation for the patient support programs run by sponsors. The most prevalent response was an expressed preference for oral medications over the alternative, injections.
Drawbacks of Oral DMTs
Drawbacks patients noted around oral DMTs reflected concerns around taking medication for MS in general. One participant expressed negative feelings about needing to be on a drug for the rest of her life, and another regarded their twice-daily DMT regimen as a constant reminder that they had MS.
Patients also described the impact that their GI-related symptoms had on their day-to-day life, including impact on functioning, activities of daily living (ADLs), and instrumental activities of daily living (IADLs), such as work, exercise and leisure, and emotions. Coping strategies for dealing with GI-related symptoms included adapting schedules based on expected symptom onset, dietary changes, taking over-the-counter medications to address specific symptoms, resting, and adapting clothing choices.
Six patients discussed the impact of GI-related symptoms on their work life. Experiences were variable, with several explaining that impact was relatively short lived during dose titration, some experiencing a low-level, ongoing impact on their work-life, and others stating that they stopped working in part due to GI symptoms related to their oral DMT regimen. Diarrhea and abdominal pain/discomfort were reported to have the most impact on patients’ work experience; nausea was also reported to interfere with work.
Several patients highlighted the impact that GI-related symptoms had on their exercise and leisure activities. For these patients, impact related specifically to the need to be near a toilet when experiencing nausea or diarrhea, which curtailed outdoor activities, and lack of motivation and desire to exercise or socialize when experiencing GI symptoms.
GI-related symptoms also had emotional impacts on this group of patients. Study participants described feelings of depression, irritability, isolation, lethargy, and worry associated with the side effects of oral DMTs.
Two different aspects of symptom duration were described by patients. Some patients described duration in terms of the length of a single episode (e.g., 3- to 4-h instances of diarrhea or stomach pain), while others referenced the persistence of the symptom over time (e.g., constipation “coming and going” over several weeks). For the patients in this sample who had been taking oral DMTs between 1 to 10 years, the experience of GI-related symptoms was not confined to the dose titration stage but instead was ongoing and persistent. Some patients described intermittent symptoms that had only an occasional impact on daily life activities. For others, GI-related symptoms and their impact on work, family life, social and leisure activities, and emotions were described as more pervasive and limiting.
Tolerability
Tolerability discussions with HCPs and patients highlighted the key role that ongoing patient education support can play in helping patients stay on these treatments. HCPs advocated for proactive patient education so that patients were prepared for potential GI-related AEs, were aware of how the treatment should be taken (i.e., with food), and knew what their options were for managing AEs when they happen. Patients and HCPs cited support during the dose titration process as a key success factor, citing regular calls with clinic staff and using support phone lines as methods helpful in navigating dose titration.
The most prevalent response was an expressed preference for oral medications over the alternative, injections. Patients described weighing these positive aspects of treatment against the impacts they experienced, particularly during dose titration, their fear that these symptoms would not resolve, the ongoing impacts of living with long-term GI-related symptoms, and their fear of long-term effects. The tolerability concepts and concerns generated in patient interviews were reflected in the interviews with HCPs, who outlined the same general picture of oral DMT tolerability considerations. Key considerations in patient experiences with oral DMTs are summarized in Table 4 below.
Table 4 Patient experiences with oral DMTsIGISIS and GGISIS Content ValidityHCP Feedback on PROs
Overall, HCP feedback on the IGISIS and GGISIS questionnaires used to assess patient-reported GI AEs in DRF trials broadly supports the content validity of both instruments. HCPs thought IGISIS was a valuable instrument and easy to complete. They indicated that the five symptoms assessed by the IGISIS instrument—nausea, vomiting, upper and lower abdominal pain, and diarrhea—are among the most clinically relevant and impactful GI-related symptomatic adverse events experienced by patients. No consensus arose when HCPs were asked which symptom was the most important from the patient perspective, suggesting that all symptoms assessed by the IGIGIS are important to assess. This finding aligns with the results of the symptom concept elicitation described above, where nausea, vomiting, diarrhea, and abdominal pain/cramping were reported as the most prevalent and impactful symptoms.
All HCPs stated that the GGISIS items assessing overall symptom intensity, bothersomeness, and interference with everyday activities and work are relevant. Across the questions included in GGSIS, there were few reported issues relating to interpretation or clarity. One HCP noted that the word “bothersome” is subjective. Regarding the work questions, one HCP suggested this could be confusing for seasonal workers, and another noted that the question implies that if people are not paid, they are not employed, i.e., people doing voluntary work are excluded.
Feedback regarding both instruments as administered together was positive overall, with six HCPs specifically reporting that they complement one another and cover aspects that are important to patients. Three HCPs noted some overlap between the two scales or stated that they believe that patients would find them similar. They also noted that completing both instruments would not be burdensome to patients if the trial period is not too long.
Patient Feedback on PROs
Content validity is generally defined as the extent to which a questionnaire measures what is intended [31]. Patient debriefing of these PROs broadly supports the content validity of both the IGISIS and GGISIS questionnaires. Patients understood and endorsed the five IGISIS symptoms as relevant and comprehensive and stated that the GGISIS assessment of overall intensity, bothersomeness, daily activity interference, and work productivity is important. Patients encountered little difficulty in responding to intensity and interference questions using the response options provided. These findings align with HCP perspectives on the relevance, comprehensiveness, and acceptability of the instruments.
For each item in the scales, participants were asked what change of score on both the intensity and interference scales would constitute a meaningful change in their status. This was framed by asking the participant to explain what change in their current score (if higher than “did not have” or “not at all”) would be meaningful. Participants were also specifically asked to explore the movement from 2 to 1 or 2 to 0 on the 11-point intensity scale for both IGISIS and GGISIS. For some patients, a 1-point change was considered intrinsically meaningful. For others, a 1-point change was considered less meaningful, particularly on the lower end of the scale where some participants perceived the difference between a score of 1 or a score of 2 to be negligible. Change from 2 to 0 was universally considered meaningful by patients who were asked this question across all items and symptoms.



留言 (0)