
記住我


In general, clinicians confirmed the findings from the literature review in terms of the signs, symptoms, and immediate impacts of cholestatic pruritus. For example, clinicians consistently emphasized the importance of pruritus and noted that it is most troublesome when a child goes to bed, can be exacerbated by warm weather, and that itching of the ears can be particularly troublesome. Clinicians also suggested that cholestatic pruritus varies in severity and age of onset depending upon the underlying CLD. They indicated that cholestatic pruritus is a more severe symptom and emerges earlier in life in PFIC and Alagille syndrome than in other CLDs such as biliary atresia or primary sclerosing cholangitis.
Suggestions from clinicians included the addition of “bone loss/brittle bones” to the initial listing of signs from the literature review. Clinicians emphasized that interference with sleep and difficulty focusing while in school are two key impacts of CLD and indicated that “impaired cognitive development” is too broad to be measured through this type of instrument. In place of this concept, they suggested assessing difficulty focusing while in school and forming social bonds. They also noted that general impacts, such as depression or fatigue, are not easily attributable to cholestatic pruritus alone and may not be useful in instrument development. All clinicians agreed that existing instruments for assessing pruritus at the time that the interviews were conducted did not adequately measure the features and impacts of pediatric cholestatic pruritus. Examples of available instruments (and the patient populations in which they were initially described) that were reviewed with clinicians included the Pruritus Grading System (in patients with dermatologic or uremic conditions) [24], the Patient Benefit Index (in patients with pruritus of various origins) [25], the Eppendorf Itch Questionnaire (in patients with eczema) [26], the ItchyQoL (in adults with dermatologic conditions) [27], the 5-D itch scale (in adults with liver disease, kidney disease, dermatologic conditions, human immunodeficiency virus, or burn injuries) [28], the Children’s Dermatology Life Quality Index (in children with dermatologic conditions) [29], the Itch Severity Scale (in patients with psoriasis) [30], the Visual Analogue, Numerical Rating, and Verbal Rating Scales (in patients with chronic pruritus of any origin) [31], and the McGill Pain Questionnaire adapted for use in uremic pruritus [32]. In addition, examples of pruritus rating scales used in natural history or interventional studies in children with CLDs were also presented (e.g,. as described in Kronsten et al. [33] and Hasegawa et al. 2014 [34], which used the scale described by Whitington [35] that is sometimes referred to as the Clinician Scratch Scale, or CSS [36]).
Based on the information gathered during the literature review and clinician interviews, initial versions of the PRO and ObsRO instruments for pediatric CLD (i.e., PRUCISION instruments) were drafted. These measures were to be completed twice daily (upon waking each morning and before going to bed) and covered concepts such as pruritus, pain, gastrointestinal problems, and sleep disturbance.
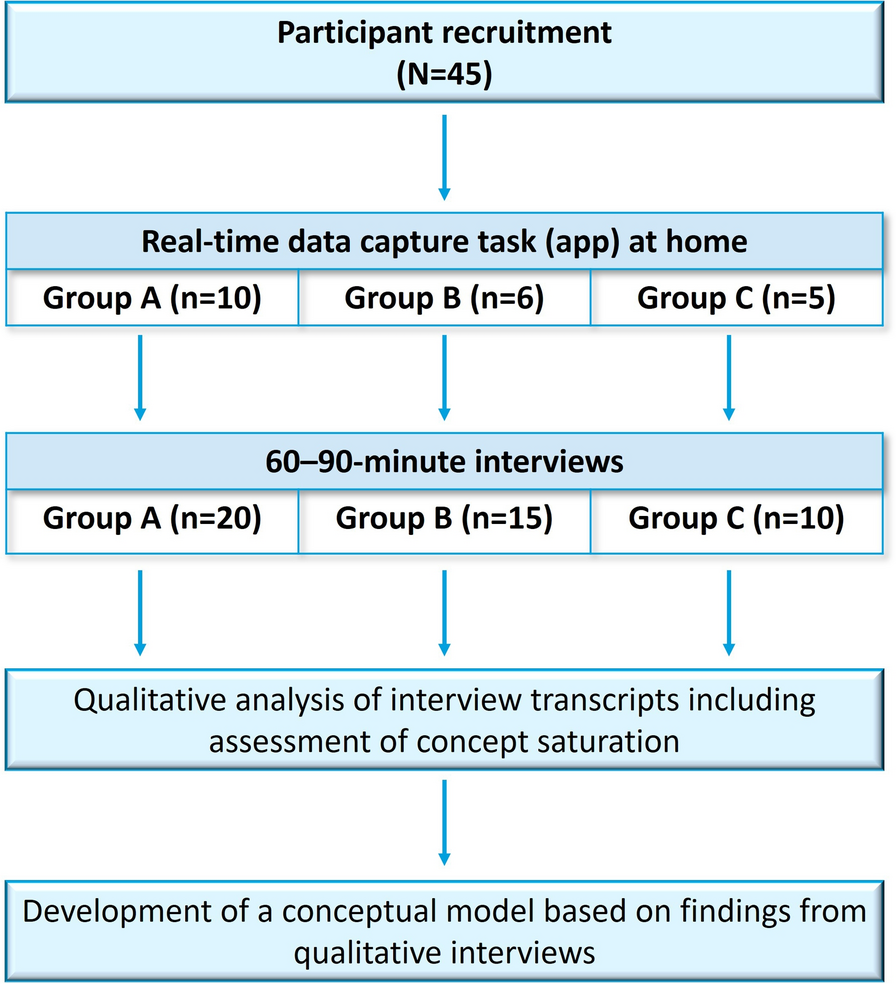
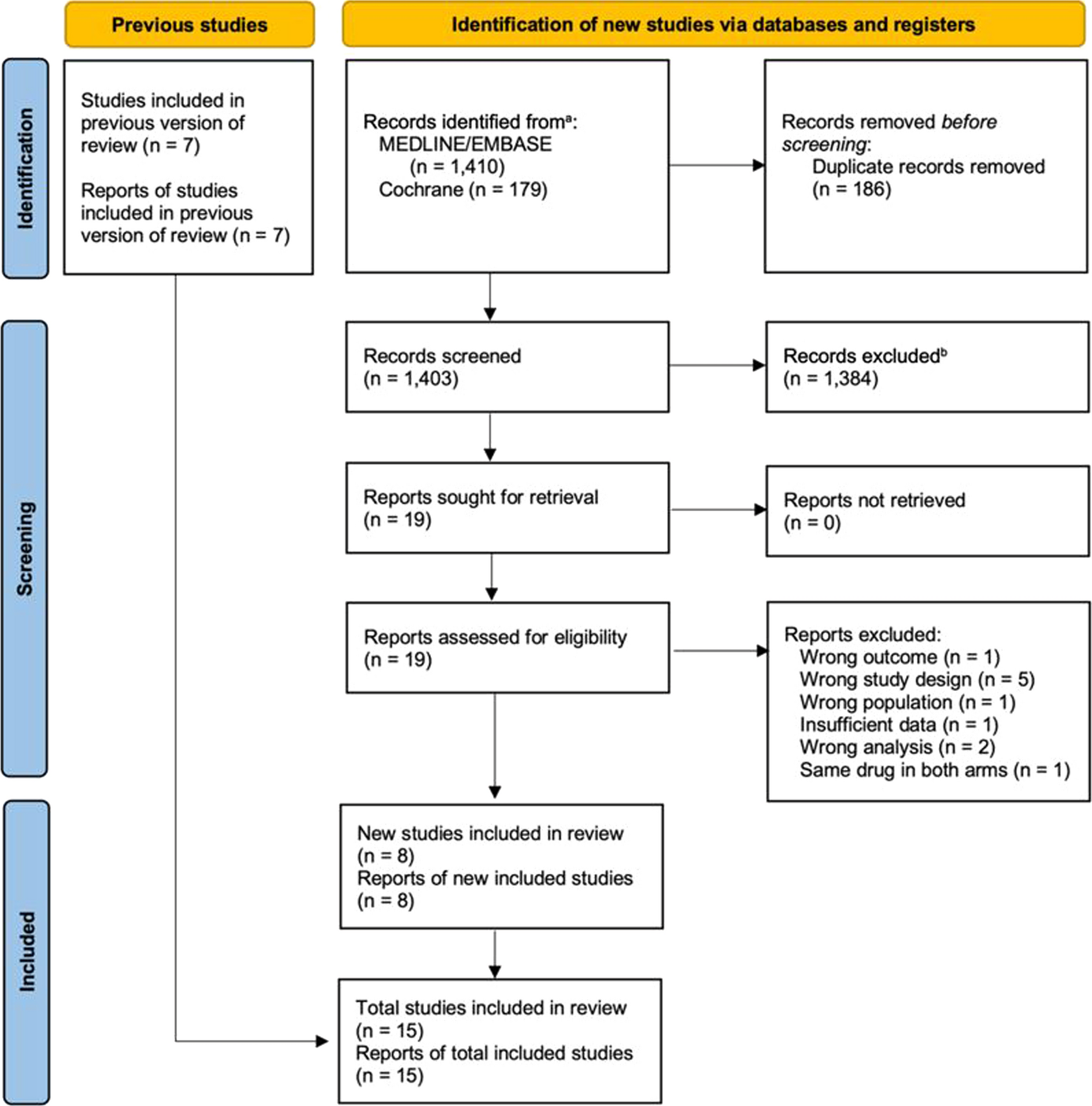
Patient and Caregiver InterviewsStudy ParticipantsA total of 36 interviews were conducted with 28 patients and caregivers across the two stages; eight patients and caregivers were interviewed in both stages I and II. While the study was designed to include 21 patients and/or their caregivers in stage I interviews, only 15 were recruited, met eligibility criteria, and participated in stage I interviews, which were completed in four sequential series (n = 5, n = 5, n = 4, and n = 1, respectively), with modifications to the instruments made after each series. Twenty-one patients and/or their caregivers met eligibility criteria and were interviewed in stage II in three series (n = 15, n = 1, and n = 5, respectively). Series in stage I and II interviews that only included one interview each were due to receipt of regulatory feedback and subsequent revision of the instruments. A summary of patient characteristics among interviewees, including CLD type and age group, is shown in Table 2.
Table 2 Summary of patient characteristics among intervieweesStage I Interview FindingsSaturation, Symptoms, and ImpactsDuring the stage I concept elicitation interviews, saturation was attained after eight interviews had been conducted. Patients and their caregivers indicated that pruritus was the most frequent and highly disturbing symptom associated with CLDs, with an average disturbance rating of 7.7 (Fig. 2a). In the subgroup of patients with PFIC, the average disturbance rating associated with pruritus was similar but slightly higher than in patients with non-PFIC diagnoses (Fig. 2b).
Fig. 2
Patient/caregiver-reported symptoms and associated disturbance in pediatric cholestatic liver diseases in all patients (a) and by subgroups of patients with PFIC or other diagnoses (i.e., non-PFIC) (b). Based on sample of n = 13; disturbance ratings were not obtained during two patient interviews. PFIC progressive familial intrahepatic cholestasis
Overall, the impact that pruritus had on sleep was considered to be highly disruptive because it often interfered with the sleep of not only the patient but also the family. Sleep disturbance and fatigue were the most common impacts experienced by patients with CLDs and pruritus, with an average disturbance rating of 8.3 and 7.8, respectively (Fig. 3a). In the subgroup of patients with PFIC, the average disturbance ratings associated with sleep disturbance and fatigue were similar but slightly higher than in patients with non-PFIC diagnoses (Fig. 3b). Many caregivers reported that their children were highly irritable as a result of fatigue and constant pruritus. Several quotes from caregivers of patients with CLDs, presented in Table 3, illustrate patients’ experience with pruritus, which seems to be particularly bothersome at night.
Fig. 3
Patient/caregiver-reported impacts and associated disturbance in pediatrics with cholestatic liver diseases and pruritus in all patients (a) and by subgroups of patients with PFIC or other diagnoses (i.e., non-PFIC) (b). Based on sample of n = 13; disturbance ratings were not obtained during two patient interviews, and ratings for fatigue were only reported by eight interviewees. PFIC progressive familial intrahepatic cholestasis
Table 3 Select quotations from caregivers of patients with cholestatic liver disease on the patient experience of pruritus and associated impactsThe frequency and average disturbance ratings of other commonly reported symptoms and impacts in all patients and in patients with PFIC or other diagnoses are depicted in Figs. 2 and 3.
Insights from Stage I Cognitive Debriefing Interviews and Summary of Changes MadeAfter the stage I cognitive interviews, several refinements were made to the PRO and ObsRO instruments based on feedback from patients and caregivers. First, wording adjustments were made to certain phrases so they would be easier for children to understand. For example, several children questioned the meaning of the word “moderate,” so it was replaced with the word “medium.” In addition, the original instruction of “please rate” the itching was simplified to “how bad is” the itching. Wording changes in the PRO were carried over to the ObsRO for consistency. Second, several concepts were either removed or expanded based on the information gathered during the interviews. For example, concepts that were identified in the literature review or included following clinician interviews were not considered as relevant to patients and caregivers (e.g., gastrointestinal symptoms, pain) and were subsequently removed from the PRO and ObsRO instruments. Furthermore, caregivers considered sleeping with and soothing their children to be two separate concepts, so these were split into separate items when the instruments were revised. Finally, the PRO and ObsRO instruments were modified to use a five-point pictorial faces scale instead of a verbal response scale, and a training guide for caregivers was created.
Stage II Interview FindingsThe major adjustments made following the stage II interviews were the addition of details to the caregiver training guide and modifications to the ObsRO instrument instructions. Specifically, in the caregiver training, a few sentences were added to give caregivers examples of what could be considered scratching behavior. For example, observable pruritus-related behaviors in patients could include scratching with their hands, scratching by rubbing their body parts against objects, asking their parents to scratch them, restlessness, kicking of legs, and/or crying/irritability and complaints about itching. The instructions in the ObsRO were then revised to align with the caregiver training material, such that caregivers were asked to think about all of the different types of scratching behaviors when rating their child’s scratching.
Card-Sorting TaskA total of 13 patients completed the card-sorting task. All of these patients could correctly sort the cards in order from “feeling ok” to “feeling the worst,” and when comparing two cards, all patients correctly identified which card was “feeling worse.” Therefore, it was determined that children aged ≥ 6 years could differentiate between all five faces of the pictorial scale and understood their order, supporting the content validity of this rating scale.
Qualitative Assessment of Meaningful ChangePotential thresholds for meaningful within-patient change were explored in 19 stage II interviews. Interviewed patients and caregivers indicated that an approximately two-point decrease in itching or scratching on the five-point pictorial scale would constitute a meaningful change. However, this estimate should be considered preliminary, as patients did not experience actual changes in pruritus during the course of instrument development.
Quantitative measurement characteristics, including an empirically derived threshold for clinically meaningful change in pruritus score, were established based on an independent, blinded, psychometric analysis that is the subject of a companion article in this issue. In brief, the psychometric performance of the ObsRO PRUCISION instrument was evaluated using data from the phase 3, randomized, placebo-controlled study of odevixibat in patients with PFIC (NCT03566238) [37]. Scores on the PRUCISION scale in this patient population were compared with scores from other established rating scales (i.e., patient-, caregiver-, and clinician-reported Global Impression of Change and Global Impression of Symptoms scales; Pediatric Quality of Life Inventory and family impact module) to test the instrument’s reliability, construct validity, and sensitivity to change.
Age at AdministrationOver the course of the stage II interviews, the minimum age at which the PRO instrument could be administered was determined based on multiple factors, including a patient’s ability to pay attention over the course of the interview, read the items, answer the items, explain what the items meant to them, complete the card-sorting task, or answer the meaningful-change questions. In general, patients aged 6 to 8 years had difficulty responding to the PRO items appropriately, even with support from their caregiver. Therefore, it was decided that the ObsRO instrument was to be used for patients younger than 8 years of age, while the PRO instrument could be used in patients aged 8 years and older.
Final Developed InstrumentsThe PRO and ObsRO instruments were finalized following completion of the stage II interviews. The final developed PRUCISION instruments are depicted in Fig. 4a and b, respectively. For each PRUCISION instrument, intended to be administered once in the morning and once in the evening in an electronic diary format, it takes users approximately 1–2 minutes to complete each assessment.
Fig. 4

Final PRUCISION PRO (a) and ObsRO (b) instruments to assess pruritus and sleep characteristics in patients with pediatric cholestatic liver diseases. ObsRO observer-reported outcome, PRO patient-reported outcome
留言 (0)