The WHO proposed ‘rapid ART initiation’ in 2017 and recommended that patients with no contraindication to rapid ART initiation should be offered ART initiation within 7 days of HIV diagnosis [1]. However, the timeframe of rapid ART initiation was not especially emphasized in some low-income and middle-income countries (LMIC), especially LMIC with a low HIV burden [2,3]. As rapid ART initiation is resource-intensive [4], and it is not easy or practical to implement this strategy in realistic resource-limited public settings. Therefore, the major concern now focuses on how rapidly to initiate ART to obtain maximum benefits in realistic, resource-limited public settings.
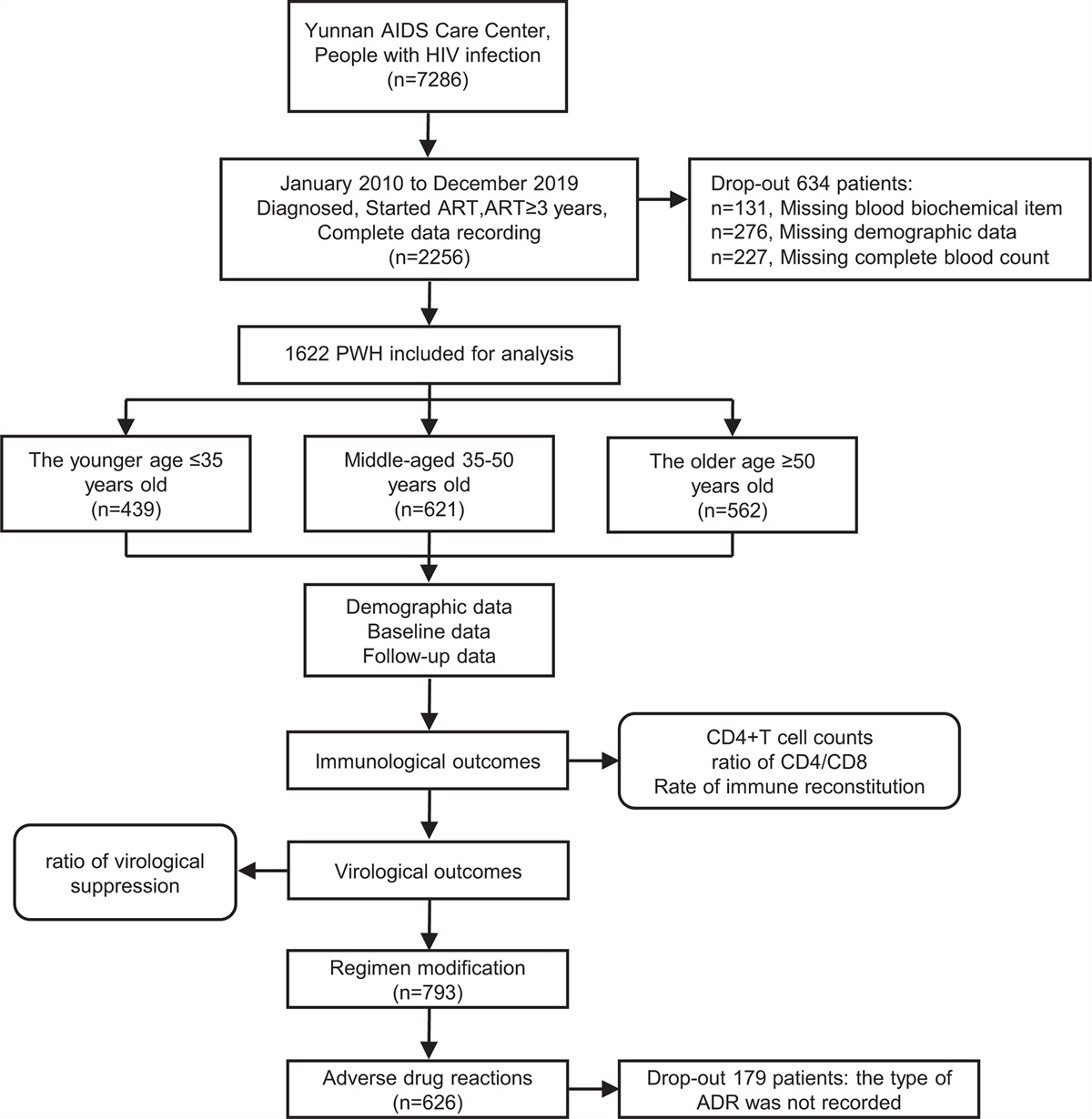
A retrospective observational cohort was conducted among people with HIV (PWH) who received a confirmed diagnosis of HIV infection in Shenyang city, a moderately HIV-prevalent province in China (PWH >10 000) [5], between 1 January 2016 and 31 December 2019. All patients who initiated ART were categorized into three groups according to the time of ART initiation, including the 7 days or less group (rapid ART initiation), the 8–30 days group, and the greater than 30 days group (deferred ART initiation). The baseline demographic, epidemiological data, and plasma samples were collected at the time of diagnosis, and clinical data were also collected until 31 December 2020.
In this study, we assessed the impact of ART initiation time on individual and community benefits in resource-limited settings. Viral suppression (<50 copies/ml [6]) rate within 180 or 360 days post-ART initiation (DPA) and CD4+ T-cell count increase within 180–360 or after 360 DPA were detected to assess individual clinical benefits. On the basis of the baseline HIV pol sequence (HXB2: 2253–3300 base pairs), the lower risk of HIV transmission can be assessed as public health benefits by inferring molecular networks using HIV-TRACE [7]. The number of links between individuals in the network has been considered the most direct indicator to assess the risk of HIV transmission [8]. The other indicator is based on the contribution of individuals to recent HIV infection (RHI) in the network, which was determined by HIV-1 Limiting Antigen Avidity tests [9]. For example, a newly diagnosed RHI in 2017 can only be infected by those individuals who were infected with HIV before 2017 (inclusive). Finally, we can compare the proportion of individuals with a high risk of transmitting HIV in each group.
(The individuals with link ≥4 or the individuals that contributed to RHI in each group / All the individuals in each group involved in building the molecular network)
A total of 2842 patients were included in this study; 93.1% were men. The median age was 32 years [interquartile range (IQR) = 26–45]. Further, 81.9% were self-reported to be MSM, and 33.1% cases were RHI. 87.8% initiated ART and the number of individuals in the 7 days or less group, the 8–30 days group, and the greater than 30 days group were 817, 1009; and 668, respectively. 12.2% PWH did not initiate ART or lost follow-up. The median time of ART initiation was 5 days (IQR: 1–6), 16 days (IQR: 12–22), and 61 days (IQR: 40–165). 71.3% PWH who initiated ART applied the standard first-line ART regimen (Tenofovir/zidovudine + Lamivudine + Efavirenz) in China [3] (Supplementary Table 1, https://links.lww.com/QAD/C580).
Cox proportional hazards regression was used to evaluate determinants of viral suppression rate. Two thousand one hundred and two (95%) PWH with viral suppression were recorded, for an overall viral suppression rate of 11.3 per 100 person-months. ART initiation within 7 days of HIV diagnosis was the most important factor (adjusted hazard ratio = 1.268, P < 0.0001), and ART initiation within 8–30 days of HIV diagnosis was a modest important factor (adjusted hazard ratio = 1.132, P = 0.017) relative to ART initiation after 30 days of HIV diagnosis (Supplementary Table 2, https://links.lww.com/QAD/C581). There was no significant difference in viral suppression rate between the 7 days or less group and the 8–30 days group, regardless of within 180 or 360 DPA, and both were significantly higher than that of the more than 30 days group (Table 1).
Table 1 -
The virological and CD4+ T-cell response and HIV transmission risk of the people with HIV in antiretroviral therapy groups
7 days vs. greater than 30 days
8–30 days vs. greater than 30 days
Characteristics
Total (n = 2494)
%
7 days or less group (n = 817)
8–30 days group (n = 1009)
>30 days group (n = 668)
P value
P value
Viral suppression rate (<50 copies/ml)
2102
84.3
n = 687
n = 863
n = 552
within 180 DPA
1237
49.6
431 (62.7)
510 (59.1)
296 (53.6)
0.0012
0.0427
within 360 DPA
1721
69.0
581 (84.6)
709 (82.2)
431 (78.1)
0.0035
0.059
CD4+ T-cell count increase (cells/μl)
Total
1304
52.3
n = 444
n = 532
n = 328
Within 180–360 DPA
158 ± 156
141 ± 186
105 ± 181
<0.0001
0.004
Total
1259
50.5
n = 393
n = 517
n = 349
After 360 DPA
224 ± 191
201 ± 196
169 ± 259
0.001
0.04
HIV transmission risk
Total
2312
92.7
n = 756
n = 941
n = 615
Link at least 4
146
5.9
37 (4.9)
54 (5.7)
55 (8.9)
0.0033
0.0163
Linking to RHI
385
15.4
110 (14.6)
151 (16.0)
124 (20.2)
0.0062
0.0378
ART, antiretroviral therapy; DPA, days post-ART initiation; PWH, people with HIV; RHI, recent HIV infection.
However, there were still no significant differences on CD4+T-cell count increase between the 7 days or less and 8–30 days groups, regardless of within 180–360 or after 360 DPA, and both were also significantly higher than those in the more than 30 days group (Table 1).
The molecular networks of the three major subtypes [CRF01_AE; CRF07_BC; and B (92.9%)] was inferred [10]. The third quartile of the number of links for all individuals with links greater than 1 in the network was 4; therefore, link at least 4 was identified as the standard for high risk of transmitting HIV. The proportion of individuals with link at least 4 in the 7 days or less group and 8–30 days group were similar and significantly lower than that in the more than 30 days group. The fraction of individuals linked to RHI in the 7 days or less and 8–30 days groups were also similar and significantly lower than those in the more than 30 days group (Table 1).
Previous studies only focused on the benefits of rapid ART initiation [11–14] or ART initiation within 30 days after HIV diagnosis [15,16]. Our study was the first to compare the benefits of ART initiation within 7 and 8–30 days after HIV diagnosis at the individual clinical and public health levels. We found that ART initiation within 30 days of HIV diagnosis could achieve benefits similar to those of ART initiation within 7 days of HIV diagnosis in resource-limited settings. In addition, we also found that the individuals in the more than 30 days were most likely to be less than 30 years old and have better immune status (higher baseline CD4+ T-cell count), which suggested that relatively good physical condition could be obstacle to immediate ART initiation (Supplementary Table 1, https://links.lww.com/QAD/C580). This study is also another good example of applying molecular network technology to evaluate public health benefits of ART initiation time by assessing the risk of HIV transmission [8]. More importantly, our study is a real-world, whole population observation study, rather than a cohort study with specific research purposes, and therefore, likely reflects the real effect of different ART initiation times.
Our study has some limitations. First, inferred linkage in molecular network does not prove transmission. Second, we were unable to determine, which regimens better contributed to positive outcomes because of the different ART regimens of PWH in each ART group. Third, we did not analyze the impact of the time of ART initiation time on the virtual reservoir, the viral setpoint, immune damage and so on.
Overall, ART initiation within 7 days and 8–30 days of HIV diagnosis had similar benefits in terms of ART efficacy and control of HIV transmission, both of which were superior to deferred ART initiation. This study provides important evidence to guide rapid ART initiation in real-world, resource-limited public settings.
Acknowledgements
Authors’ contributions: H.S. and X.X.H. conceived the study; W.S., X.D., X.L., L.U.W., J.M.L. Z.X.C. and H.B.D. collected samples and epidemiology data; B.Z., Y.Q. and L.I.N.W. conducted the experiments and collected the data, B.Z., H.B.D. and M.M.K. analyzed the results and B.Z. drafted the manuscript. X.X.H. and H.B.D. reviewed and edited the manuscript. All authors read and approved the final manuscript.
Sources of funding: this work was supported by Mega-Projects of National Science Research for the 13th Five-Year Plan (2018ZX10721102); The National Natural Science Foundation (81871637); CAMS Innovation Fund for Medical Sciences (2019-I2M-5-027), Scientific Research Funding Project of Liaoning Province Education Department (QN2019005); Shenyang Science and Technology Project (19-112-4-004). Data in this manuscript were collected by the Shenyang Center for Disease Control and Prevention.
Conflicts of interest
There are no conflicts of interest.
References
1. World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Geneva: WHO; 2017.
2. Perez F, Gomez B, Ravasi G, Ghidinelli M. Progress and challenges in implementing HIV care and treatment policies in Latin America following the treatment 2.0 initiative. BMC Public Health 2015; 15:1260.
3. AIDS and Hepatitis C Professional Group, Society of Infectious Diseases, Chinese Medical Association; Chinese Center for Disease Control and Prevention. Chinese guidelines for diagnosis and treatment of HIV/AIDS (2018). Zhonghua nei ke za zhi 2018; 57:867–884.
4. Wu Z, Zhao Y, Ge X, Mao Y, Tang Z, Shi CX, et al. Simplified HIV testing and treatment in China: analysis of mortality rates before and after a structural intervention. PLoS Med 2015; 12:e1001874.
5. Wu Z, Chen J, Scott SR, McGoogan JM. History of the HIV epidemic in China. Curr HIV/AIDS Rep 2019; 16:458–466.
6. Joya C, Won SH, Schofield C, Lalani T, Maves RC, Kronmann K, et al. Persistent low-level viremia while on antiretroviral therapy is an independent risk factor for virologic failure. Clin Infect Dis 2019; 69:2145–2152.
7. Kosakovsky Pond SL, Weaver S, Leigh Brown AJ, Wertheim JO. HIV-TRACE (TRAnsmission Cluster Engine): a tool for large scale molecular epidemiology of HIV-1 and other rapidly evolving pathogens. Mol Biol Evol 2018; 35:1812–1819.
8. Little SJ, Kosakovsky Pond SL, Anderson CM, Young JA, Wertheim JO, Mehta SR, et al. Using HIV networks to inform real time prevention interventions. PLoS One 2014; 9:e98443.
9. He X, Xing H, Ruan Y, Hong K, Cheng C, Hu Y, et al. Group for HIV Molecular Epidemiologic Survey. A comprehensive mapping of HIV-1 genotypes in various risk groups and regions across China based on a nationwide molecular epidemiologic survey. PLoS One 2012; 7:e47289.
10. Zhao B, Song W, Kang M, Dong X, Li X, Wang L, et al. Molecular network analysis reveals transmission of HIV-1 drug-resistant strains among newly diagnosed HIV-1 infections in a moderately HIV endemic city in China. Front Microbiol 2021; 12:797771.
11. Rosen S, Maskew M, Fox MP, Nyoni C, Mongwenyana C, Malete G, et al. Initiating antiretroviral therapy for HIV at a patient's first clinic visit: the RapIT Randomized Controlled Trial. PLoS Med 2016; 13:e1002015.
12. Koenig SP, Dorvil N, Devieux JG, Hedt-Gauthier BL, Riviere C, Faustin M, et al. Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: a randomized unblinded trial. PLoS Med 2017; 14:e1002357.
13. Coffey S, Bacchetti P, Sachdev D, Bacon O, Jones D, Ospina-Norvell C, et al. RAPID antiretroviral therapy: high virologic suppression rates with immediate antiretroviral therapy initiation in a vulnerable urban clinic population. AIDS 2019; 33:825–832.
14. Pathela P, Jamison K, Braunstein SL, Borges CM, Lazar R, Mikati T, et al. Initiating antiretroviral treatment for newly diagnosed HIV patients in sexual health clinics greatly improves timeliness of viral suppression. AIDS 2021; 35:1805–1812.
15. Zhao Y, Wu Z, McGoogan JM, Shi CX, Li A, Dou Z, et al. Immediate antiretroviral therapy decreases mortality among patients with high CD4 counts in China: a nationwide, retrospective cohort study. Clin Infect Dis 2018; 66:727–734.
16. Zhao Y, Wu Z, McGoogan JM, Sha Y, Zhao D, Ma Y, et al. Nationwide cohort study of antiretroviral therapy timing: treatment dropout and virological failure in China, 2011–2015. Clin Infect Dis 2019; 68:43–50.




留言 (0)