
記住我


The Cancer Genome Atlas (TCGA) data suggest UHRF1 is significantly overexpressed in malignancies that frequently present RB pathway inactivation including sarcomas, breast invasive carcinomas, and lung adenocarcinomas, but not in cancers where RB1 loss is infrequent, like prostate adenocarcinomas (Supplementary Fig. 1A) [17]. In sarcomas, high UHRF1 expression is associated with poorer survival (Supplementary Fig. 1B). UHRF1 expression analysis using published RNA-Seq datasets from pretreatment biopsies from 88 osteosarcoma patients [18] associate high UHRF1 expression with poorer overall survival (Fig. 1A). UHRF1 mRNA in situ hybridization on an osteosarcoma tissue array confirmed a correlation between stage of malignancy and UHRF1 expression (Supplementary Fig. 1C, D).
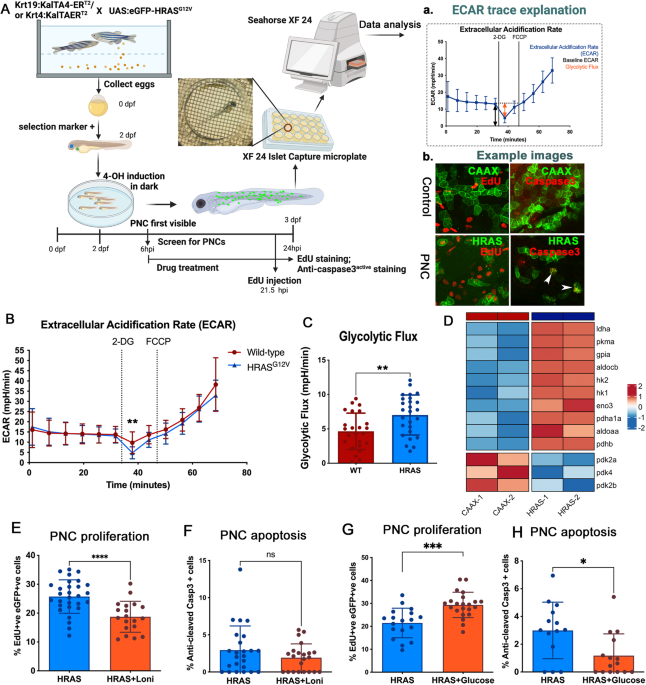
Fig. 1: UHRF1 expression directly correlates with malignancy and metastasis in osteosarcoma.
A Overall survival probability of osteosarcoma patients comparing tumors with high UHRF1 (blue, n = 38) versus low UHRF1 (red, n = 50) expression at the time of diagnosis. B, C Western blot analysis of UHRF1 in (B) human osteosarcoma cell lines compared to MSC as control and (C) PDXs tumors. High exposure was used for UHRF1 detection in MSCs. β-actin was used as a loading control.
The clinical data led to examine UHRF1 mRNA and protein levels in 4 human osteosarcoma cell lines: 143B, SJSA-1, SaOS-2 (RB1-null cell line), and U-2 OS, and 5 patient-derived orthotopic xenografts (PDX1-5). qPCR analysis showed significant upregulation of UHRF1 mRNA levels in all samples except PDX2 when compared to MSC, independent of RB1 expression (Supplementary Fig. 1E–H). At the protein level, UHRF1 was highly expressed across all samples compared to MSC (Fig. 1B, C).
UHRF1 is a direct target of the RB/E2F signaling pathway in the osteogenic lineageUHRF1 is reported as a direct E2F1 transcriptional target [19, 20]. Chromatin immunoprecipitation (ChIP) analysis using mesenchymal stem cells (MSCs) confirmed E2F1 enrichment at consensus binding motifs within the UHRF1 promoter (Supplementary Fig. 2A). However, knocking down E2F1 alone was insufficient to decrease UHRF1 expression in osteosarcoma cells (Supplementary Fig. 2B). We tested compensation by other activator E2Fs and found that knocking down E2F1 alongside E2F3, but not E2F2, reduced UHRF1 expression in osteosarcoma (Supplementary Fig. 2C, D). E2F3 knockdown alone was also insufficient to decrease UHRF1 expression (Supplementary Fig. 2E). Treatment with palbociclib, a CDK4/6 inhibitor, decreased UHRF1 mRNA and protein levels in all cell lines except SaOS-2, which is RB1-null and served as negative control (Supplementary Fig. 2F, G). Increased UHRF1 expression in RB1-wild-type cells correlated with upregulation of CDK4 and/or CDK6 transcripts and/or INK4A downregulation (Supplementary Fig. 2H, I). CDK4 amplification occurs in SJSA-1 and INK4A deletion in U2-OS [21, 22]. Thus, the RB/E2F pathway regulates UHRF1 through direct transcriptional activation by activator E2Fs, E2F1, and E2F3.
UHRF1 overexpression promotes osteosarcoma cell proliferation in vitro and in vivoEmerging reports link UHRF1 overexpression in cancer with proliferation, migration/invasion, or both [10, 23,24,25,26,27,28,29]. To study the role of UHRF1 in osteosarcoma, we generated syngeneic UHRF1 CRISPR knockout clones (KO) and non-targeting vector controls (VC). Successful UHRF1 KO was achieved in all four osteosarcoma cell lines tested (Fig. 2A). Proliferation and EdU-incorporation analyses indicated UHRF1 KO cells have longer doubling times and lower proliferation rates compared to VC (Supplementary Fig. 3). This decrease in proliferation was confirmed by clonogenic assays showing significant reductions in both the number and the size of colonies in UHRF1 KO compared to VC cells (Fig. 2B, C).
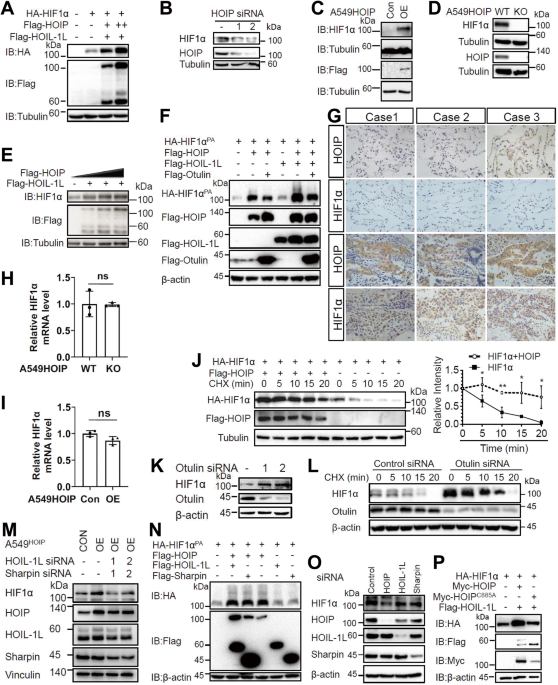
Fig. 2: UHRF1 promotes osteosarcoma tumor growth in vitro and in vivo.
A Western blot analysis of UHRF1 in CRISPR/Cas9-mediated UHRF1 knockout of osteosarcoma cell lines (KO) in comparison to non-targeting vector control (VC). β-actin was used as a loading control. B Representative images from clonogenic assay plates with 143B VC and UHRF1 KO. C Histogram of colony counts from clonogenic assay. *P < 0.05, **P < 0.01 by unpaired two-tailed t test. D Cartoon representation for doxycycline-inducible in vivo knockout for flank-injected osteosarcoma cell lines carrying a non-targeting sgRNA (iCRISPR VC) or UHRF1 sgRNA (iCRISPR KO). E Quantification of the tumor volume for each of the replicates. *P < 0.05 by paired two-tailed t test. F Images from tumors collected from subcutaneous injection of iCRISPR VC (iVC, n = 5) and iCRISPR KO (iKO, n = 5) SJSA-1. G Western blot verification of UHRF1 knockout in iKO compared to iVC for tumors shown in (F). β-actin was used as a loading control. H Representative images from tumors collected from intrafemoral injection of SJSA-1 VC and UHRF1 KO. I Quantification of the tumor volume for each of the replicates, 5 weeks after intrafemoral injection. A solid linerepresents median from n = 4 for VC and n = 5 for KO. *P < 0.05 by paired two-tailed t test. J Kaplan–Meier curves showing the survival of mice with orthotopic SJSA-1 VC (black, n = 5) and UHRF1 KO (red, n = 5) xenografts.
To assess proliferative capacity in vivo, SJSA-1 UHRF1 KO and VC cells were injected subcutaneously at opposite flank regions. UHRF1 KO cells gave rise to significantly smaller tumors (average size 0.49 ± 0.37 cm3) when compared to VC (average volume 1.23 ± 0.75 cm3; P = 0.02; n = 10). The therapeutic potential of targeting UHRF1 in established tumors was tested using a doxycycline-inducible system to drive the expression of CRISPR/Cas9 gRNA against UHRF1. Inducible UHRF1 KO (iKO) and inducible VC (iVC) osteosarcoma cells were subcutaneously injected, and tumors allowed to establish for one week before inducing Cas9 expression via oral doxycycline delivery (Fig. 2D). Tumor growth was significantly reduced in UHRF1 iKO tumors (average tumor volume 0.356 ± 0.201 cm3; n = 5) compared to iVC tumors (1.455 ± 0.865 cm3; P = 0.02; n = 5) (Fig. 2E, F). Western blot analyses confirmed reduced UHRF1 protein at varying levels in UHRF1 iKO tumors (Fig. 2G). Thus, it is possible that residual tumors may be formed from cells not exposed to doxycycline or with incomplete UHRF1 KO. UHRF1 iKO tumors presented phenotypic features of less aggressive tumors, with lessened vasculature and ulceration compared to iVC tumors (Fig. 2F). Induction of a different UHRF1 gRNA in SJSA-1 resulted in similar tumor size reduction, as well as with other osteosarcoma cell lines (Supplementary Fig. 4A–D).
An orthotopic model using intrafemorally injected SJSA-1 confirmed UHRF1 KO tumors grow slower and have significantly higher survival than VC (Fig. 2H–J and Supplementary Fig. 4E). Together, our data suggest UHRF1 is critical for osteosarcoma growth.
UHRF1 promotes osteosarcoma metastasisThe high metastatic potential of osteosarcoma is the main cause of mortality in patients. UHRF1 was reported to promote cell invasion following exogenous UHRF1 overexpression in osteosarcoma [29]. Here, we evaluated whether the endogenously high UHRF1 protein levels present in osteosarcoma promote cell migration, invasion, angiogenesis, and metastasis. Scratch-wound assays were used to assess migration (Fig. 3A). UHRF1 KO resulted in a significant decrease in cell migration, with an average 56.8 ± 2.3% reduction in migration across three cell lines (Fig. 3B). Invasion assays also revealed a significant reduction in the number of UHRF1 KO cells capable of mobilizing across Matrigel-coated inserts (Fig. 3C, D).
Fig. 3: UHRF1 promotes osteosarcoma cell migration and invasion in vitro and in vivo.
A Representative image from scratch-wound assay comparing wound closure of non-targeting vector control (VC) and UHRF1 KO (KO) cells over 8 h in SJSA-1 cells. White dashed lines represent the wound edge. Scale bar, 1000 μm. B Quantification of distance (pixels) migrated in scratch-wound assays for each of the osteosarcoma cell lines. Each data point is mean ± s.d. of ten measurements in triplicate samples. C Representative images from Transwell assays with cells stained with crystal violet (purple) comparing levels of invasion between VC and UHRF1 KO in SJSA-1 cells. D Quantification of the number of cells invaded across the Transwell membrane for each of the osteosarcoma cell lines. Each data point is mean ± s.d. of triplicate samples. E Representative histological images of H&E-stained lung section from intrafemoral-injected mice with VC and UHRF1 KO SJSA-1 cells, 5 weeks after injection. Scale bar, 200 μm. Quantification of the burden of lung metastases was quantified as (F) the number of mice with or without lung metastases and (G) the number of metastatic lung nodules per mouse. A solid line represents median from n = 4 for VC and n = 5 for KO. *P = 0.03 by unpaired t test. H Representative histological images of CD31 expression in intrafemoral tumors derived from VC and UHRF1 KO SJSA-1 cells, 5 weeks after injection and (I) quantification of the average number of vessels per mm2 and (J) quantification of the mean vessel diameter. Solid line represents median from n = 4. ns not significant; ***P = 0.002 by unpaired t test. Scale bars, 100 μm. K Representative brightfield (top) and fluorescent (bottom) images of late phase sprouting angiogenesis assay (day 6) using human lung fibroblasts as assay control and 143B VC and KO conditioned media in the fibrin gel bead assay. This is quantified as (L) the number of sprouts per bead. n = 30. M 5-year metastasis-free survival probability of osteosarcoma patients comparing tumors with high UHRF1 (blue, n = 37) versus low UHRF1 (red, n = 16) expression at the time of diagnosis. For all graphs: *P < 0.05, **P < 0.01, ****P < 0.0001 by unpaired two-tailed t test.
To determine if UHRF1 overexpression is sufficient to induce cell migration, we performed gain-of-function studies in MSCs. Using a doxycycline-inducible system to drive UHRF1 overexpression (pCW57-UHRF1; Supplementary Fig. 6A, B), we observed a significant increase in MSC migration and invasion in cells induced to overexpress UHRF1 compared to controls (Supplementary Fig. 5C–F). We also utilized our pCW57-UHRF1 vector to rescue UHRF1 expression in UHRF1 KO cells. Doxycycline treatment for 24 h was able to restore UHRF1 protein expression back to levels comparable to wild-type and significantly increase migration in all osteosarcoma cell lines (Supplementary Fig. 5G, H).
The reduction in migration and invasion observed in vitro translated into a lessened metastatic potential in vivo. We assessed the rate of spontaneous lung metastasis in the NSG mice bearing intrafemoral SJSA-1 UHRF1 KO and VC tumors (Fig. 2H, I). At 5 weeks after injection, 100% of VC mice (4/4 mice) had metastatic lung nodules compared to only 60% of UHRF1 KO mice (3/5 mice) and the number of metastatic lung nodules was significantly lower in UHRF1 KO compared to VC (Fig. 3E–G). To test if UHRF1 contributes to tumor intravasation or extravasation, SJSA-1 UHRF1 KO and VC cells were injected into the tail vein of NSG mice to assess the rate of lung colonization. At 3-weeks post injection, UHRF1 KO mice had fewer lung metastatic nodules, but only the nodule size was significantly smaller than VC (Supplementary Fig. 6A–F).
Following the observation that UHRF1 loss appears to reduce tumor vascularization (Fig. 2F, H), we probed UHRF1 VC and KO orthotopic xenografts for the vasculature marker CD31. UHRF1 KO tumors exhibited reduced number of tumor vessels without reducing the overall tumor vessel caliber compared to VC (Fig. 3H–J). Thus, we evaluated a novel role of UHRF1 in cancer cell induction of endothelial cell migration (sprouting) using a fibrin gel bead assay (Fig. 3K). UHRF1 KO osteosarcoma cells displayed a significant lower ability to induce endothelial cell sprouting compared to VC (Fig. 3L). These data suggest a novel role of UHRF1 in osteosarcoma cell’s ability to affect early stages of angiogenesis.
UHRF1 expression analysis using pretreatment biopsies from 53 osteosarcoma patients [18] associate low UHRF1 expression with increased rates of 5-year metastasis-free survival (Fig. 3M). Together, these results support the role of UHRF1 in the early stages of osteosarcoma metastasis, including tumor migration, invasion, and angiogenesis, and promotes tumor growth at secondary sites.
High PLAU/uPA expression is associated with enhanced osteosarcoma cell migration and invasionGiven UHRF1 role in heterochromatin maintenance, we analyzed the effect of UHRF1 loss on DNA methylation, chromatin structure, and transcription to determine how UHRF1 serves as an oncogene in osteosarcoma. Decreased genomic DNA methylation was detected in UHRF1 KO compared to VC in most osteosarcoma cells examined (Supplementary Fig. 6A). Reduced representation bisulfite sequencing (RRBS) analysis of differentially methylated regions across the genome of VC and UHRF1 KO cells confirmed a reduction in DNA methylation, with most changes occurring at non-coding regions of the genome (Supplementary Fig. 8B). We also assessed chromatin landscape changes upon UHRF1 loss by performing ATAC-seq on UHRF1 KO compared to VC (Supplementary Fig. 8C). Despite the role of UHRF1 in heterochromatin maintenance and decreased genomic DNA methylation levels, we identified only 16 chromatin regions with significant changes in chromatin accessibility across three biological replicates (Supplementary Table 1). Within these changes, the majority were consistent with the role of UHRF1 in chromatin repression, with ~69% (11/16) resulting in the opening of chromatin upon UHRF1 loss.
In line with modest changes in DNA methylation and chromatin accessibility, transcriptome analysis using RNA-seq revealed that the gene expression profile from UHRF1 KO cell lines present minor variability from VC cells (Supplementary Fig. 8D). We identified 272 differentially expressed genes (DEGs; 191 upregulated and 81 downregulated) in UHRF1 KO compared to VC cells. Gene ontology (GO) analysis for biological processes of the DEGs revealed an enrichment of genes involved in the regulation of cell adhesion and migration (Fig. 4A). GO analysis of cellular components of the DEGs from the RNA-seq data also exposed an enrichment of genes involved in extracellular vesicle formation and cell adhesion (Fig. 4B). We confirmed the changes in gene expression observed among top the 13 genes involved in the regulation of cell migration (Fig. 4C) through qPCR (Supplementary Fig. 6E).
Fig. 4: UHRF1 controls the expression of genes involved in exosomes and urokinase plasminogen activator production to drive osteosarcoma migration.
A, B Gene ontology (GO) analysis for (A) biological processes and (B) cellular components of the downregulated differentially expressed genes (DEGs) identified through RNA-seq. C Heatmap of top 13 genes involved in the regulation of cell migration, decreased (blue) or increased (red) in expression level upon UHRF1 loss. D, F Quantification of relative distance migrated in scratch-wound assays for (D) osteosarcoma VC cells assayed with fresh media (FM) or conditioned media (24 h) from VC cells or UHRF1 KO cells, normalized to FM; E osteosarcoma UHRF1 KO cells assayed with FM or conditioned media from VC cells or UHRF1 KO cells, normalized to FM; F each of the osteosarcoma cell lines treated with DMSO, 10 µM GW4869 or 20 µM CPZ, normalized to DMSO control. Each data point is mean ± s.d. of ten measurements in triplicate samples. G qPCR analysis of PLAU mRNA levels in flank-implanted tumors from control (VC) and UHRF1 KO (KO) SJSA-1 cell lines. *P < 0.05 by paired two-tailed t test. H Quantification of relative distance migrated in scratch-wound assays for each of the osteosarcoma cell lines treated with DMSO, 150 µM amiloride, or 16.4 µM BC11 hydrobromide, normalized to DMSO control. Each data point is mean ± s.d. of ten measurements in triplicate samples. I Representative images from Transwell assays with cells stained with crystal violet comparing levels of invasion between cells treated with DMSO or 150 µM amiloride in SJSA-1. J Quantification of the number of cells invaded in Transwell invasion assay for each of the osteosarcoma cell lines treated with DMSO or 150 µM amiloride. Each data point is mean ± s.d. of triplicate samples. For all graphs: ns not significant, **P < 0.01, ***P < 0.001, ****P < 0.0001 by unpaired two-tailed t test.
The potential role of UHRF1 in migration and invasion through the control of exosome-mediated pathways was examined by testing the effect of conditioned media collected from VC and UHRF1 KO cell cultures on osteosarcoma cell migration. Conditioned media from osteosarcoma VC cells significantly increased autologous osteosarcoma cell migration compared to fresh media (Fig. 4D, blue bars). While conditioned media derived from osteosarcoma UHRF1 KO cells also increased cell migration compared to fresh media, VC cell migration was lower when exposed to UHRF1 KO conditioned media than autologous VC conditioned media (Fig. 4D, red bars). Interestingly, UHRF1 KO cells also displayed a robust increase in cell migration when exposed to VC conditioned media, but not when exposed to autologous UHRF1 KO conditioned media (Fig. 4E). Thus, UHRF1 loss decreases the secretion of pro-migratory factors to the extracellular matrix that can serve as an autologous signal to stimulate osteosarcoma cell migration but does not affect the ability of the cells to respond to these extracellular factors. Inhibition of exosome biogenesis/release using GW4869 and inhibition of endocytosis using chlorpromazine (CPZ) significantly reduced the cell migration induced by osteosarcoma conditioned media (Fig. 4F). Together, this indicates that UHRF1 overexpression alters the production and/or secretion of exosomes and/or its cargo which contribute, at least in part, to increased osteosarcoma cell migration.
Plasminogen activator, urokinase (PLAU) was one of the DEGs identified through transcriptome analysis as potentially involved in UHRF1-mediated cell migration. Encoded by PLAU, uPA is associated with cell migration and is a known cargo protein in osteosarcoma-secreted exosomes [30]. PLAU transcript levels were significantly decreased in UHRF1 KO osteosarcoma cells (Supplementary Fig. 6E) and subcutaneous xenografts, with an average 2.2-fold decrease compared to VC cell-derived tumors (P = 0.038, Fig. 4G). Thus, we tested whether uPA inhibition could decrease migratory potential and invasiveness of osteosarcoma cells. Amiloride treatment resulted in significantly reduced migration, with an average 40.3 ± 11.9% decrease across all osteosarcoma cells examined (Fig. 4H). BC11 hydrobromide treatment, a selective uPA inhibitor, resulted in a 23.2 ± 10.2% decrease in migration across all lines (Fig. 4H). Reduced invasiveness was also observed upon uPA inhibition (Fig. 4I, J). Further, amiloride treatment also inhibited cell migration in MSCs with induced UHRF1 expression (Supplementary Fig. 7). Thus, uPA is an important contributor of UHRF1-induced migration in osteosarcoma.
UHRF1 repression of AMPK activation and SEMA3E expression induces angiogenesisAnother DEG identified in our RNA-seq analysis was SEMA3E (Fig. 4C). Sema3E acts as a repulsive factor for plexin-D1-expressing endothelial cells, leading to decreased neoangiogenesis and reduced tumor growth [31]. We confirmed that the increased SEMA3E transcript expression correlated with increased SEMA3E protein levels in the KO cells compared to VC (Fig. 5A). A recent study identified that UHRF1 suppresses AMPK activity [32], and AMPK activation was shown to induce SEMA3E expression [33]. Thus, we tested whether increased SEMA3E expression is correlated with increased phosphorylated AMPK (pAMPK) levels in UHRF1 KO cells. We found that while the total AMPK is unaltered by UHRF1 loss, pAMPK is elevated in UHRF1 KO cells, confirming a direct correlation between AMPK activity and SEMA3E expression (Fig. 5B). To determine if elevated SEMA3E is, at least in part, associated with the lower ability of UHRF1 KO cells to induce angiogenesis (Fig. 3N), we next tested whether knocking out SEMA3E could reverse the decreased angiogenesis observed in UHRF1 KO cells. Inducing SEMA3E KO resulted in a significant increase in the number of endothelial cells sprouting on the surface of fibrin gel beads both in UHRF1 VC and KO cells (Fig. 5C). Interestingly, upon SEMA3E KO, the extent of angiogenesis induced by UHRF1 VC and KO cells is similar (Fig. 5C). This suggests decreased SEMA3E secretion is associated with increased angiogenesis upon UHRF1 overexpression.
Fig. 5: UHRF1 decreases SEMA3E expression through suppression of AMPK activation to induce angiogenesis.
A, B Western blot analysis of (A) SEMA3E in SJSA-1 and SaOS-2 VC and KO osteosarcoma cell lines quantification of KO normalized to VC; and (B) activated AMPK (pAMPK) and total AMPK with the quantification of the ratio. UHRF1 used to confirm VC and KO status. β-actin was used as a loading control. C Early phase sprouting angiogenesis (day 3) using human lung fibroblasts as assay control and SJSA-1 VC and KO cells with inducible sgRNA to knockout SEMA3E upon doxycycline addition in the fibrin gel bead assay. Quantified as the number of sprouts per bead. n = 30. ns not significant, *P < 0.05, ****P < 0.0001, by unpaired t test. D Model of UHRF1 oncogenic function in osteosarcoma. UHRF1 overexpression stimulates proliferation, exosome and uPA production that stimulates migration, invasion, and metastasis. UHRF1 also suppresses AMPK activation to inhibit SEMA3E and induce angiogenesis. Downstream of UHRF1, inhibitors of exosome secretion (e.g., GW4869), exosome endocytosis (CPZ), or uPA inhibitors (e.g., amiloride, BC11 hydrobromide) are attractive therapeutic options to decrease migration and metastasis. The development of UHRF1-targeted therapeutics might result in a beneficial decrease in both tumor growth and pulmonary metastases.
UHRF1 overexpression is a critical driver of metastasis and the poor survival observed in Rb1-null osteosarcomaFinally, we evaluated UHRF1’s pro-oncogenic function in osteosarcoma tumorigenesis using developmental mouse models. Loss of Tp53 in conditional knockout mice driven by osterix-cre recombinase (Tp53 cKO; Osx-cre Tp53lox/lox), a transgene expressed in preosteoblasts, results in osteosarcoma formation with complete penetrance [34, 35]. This model is potentiated by Rb1 loss (Tp53/Rb1 DKO; Osx-cre Tp53lox/loxRb1lox/lox), mimicking the poor clinical outcome of RB1 loss in human osteosarcoma [34, 35]. Analysis of osteosarcoma tumors arising from Tp53 cKO and Tp53/Rb1 DKO mice revealed that UHRF1 is highly expressed at the mRNA (Fig. 6A) and protein level (Supplementary Fig. 8B) in these mouse models.
Fig. 6: UHRF1 is a critical driver of the increased malignancy observed in RB-null osteosarcoma.
A Representative fluorescent images of in situ hybridizations using RNAscope on wild-type femurs or tumors from genetically engineered osteosarcoma mice using a probe against Uhrf1 (red). Nuclei were counterstained with DAPI (blue). Uhrf1 expression is detected in Tp53 cKO and Tp53/Rb1 DKO mouse tumors but is low or not detected in wt, Tp53/Uhrf1 DKO, and Tp53/Rb1/Uhrf1 TKO tumors. B Kaplan–Meier curves showing the survival of osteosarcoma mouse models. Mice bearing Rb1 mutations Tp53/Rb1 DKO: Osx-Cre; p53lox/lox; Rb1lox/lox (red; n = 53) have significantly shorter lifespan compared to Tp53 cKO: Osx-Cre; p53lox/lox; Rb1lox/lox (black; n = 39). This survival time was significantly increased in Tp53/Rb1/Uhrf1 TKO: Osx-Cre; p53lox/lox; Rb1lox/lox; Uhrf1lox/lox (blue; n = 37) mice. †Three surviving mice were removed from the study to confirm tumor absence. Tp53/Uhrf1 DKO: Osx-Cre; p53lox/lox; Uhrf1lox/lox (green; n = 39) showed an overall survival comparable to Tp53 cKO (black; n = 39). Mantel–Cox test were used for curve comparisons. ns not significant, *P < 0.05, ****P < 0.0001. C Summary table for each osteosarcoma mouse model. ††Age of mice (weeks) at earliest tumor detection via microCT and PET scans comparison: P < 0.05 by unpaired two-tailed t test; Tp53/Rb1 DKO (n = 4) and Tp53/Rb1/Uhrf1 TKO (n = 3).
Uhrf1 KO mice result in embryonic lethality [36]; thus, we generated Uhrf1 cKO mice (Osx-cre Uhrf1lox/lox), Tp53/Uhrf1 DKO (Osx-cre Tp53lox/loxUhrf1lox/lox) and Tp53/Rb1/Uhrf1 triple knockout (Tp53/Rb1/Uhrf1 TKO; Osx-cre Tp53lox/loxRb1lox/loxUhrf1lox/lox) to study the role of UHRF1 in osteosarcoma development. Uhrf1 cKO mice display normal bone development (Supplementary Fig. 8C, D). For Tp53/Uhrf1 DKO and Tp53/Rb1/Uhrf1 TKO mice, we tracked overall survival and tumor formation compared to the corresponding littermate controls (Tp53 cKO and Tp53/Rb1 DKO, respectively). In situ hybridization confirmed reduced Uhrf1 expression in Tp53/Uhrf1 DKO and Tp53/Rb1/Uhrf1 TKO osteosarcoma tumors (Fig. 6A). All strains presented osteosarcoma with 100% penetrance but with distinct survival rates and disease presentation (Fig. 6B, C). Consistent with previous reports, Rb1 loss in Tp53/Rb1 DKO mice resulted in shorter median survival compared to Tp53 cKO mice (Fig. 6B). Strikingly, Uhrf1 genetic ablation in Tp53/Rb1/Uhrf1 TKO mice resulted in significantly increased survival compared to Tp53/Rb1 DKO mice. Further, the median survival of Tp53/Rb1/Uhrf1 TKO was comparable to Tp53 cKO (P = 0.0577, Gehan–Breslow–Wilcoxon test), suggesting that Uhrf1 overexpression is critical for the poor prognosis associated with Rb1 loss (Fig. 1B). However, the overall survival of Tp53/Rb1/Uhrf1 TKO and Tp53 cKO mice is distinct (P = 0.0126, Mantel–Cox test), suggesting that early UHRF1 overexpression is not the only factor contributing to Rb1 loss-associated outcomes. Three Tp53/Rb1/Uhrf1 TKO mice did not acquire tumors well beyond the average of the rest of their study group (>69 weeks; Fig. 6B†). FDG-PET/microCT scans in these three mice revealed no detectable tumors (Supplementary Fig. 8E), which was confirmed upon autopsy.
Since UHRF1 is also overexpressed in Tp53 cKO tumors (Fig. 6A and Supplementary Fig. 8B), we examined the effect of Uhrf1 loss in Tp53/Uhrf1 DKO compared to Tp53 cKO mice. We observed a significant increase in median survival of Tp53/Uhrf1 DKO mice, compared to Tp53 cKO (P = 0.0007, Gehan–Breslow–Wilcoxon test), but not in overall survival (P = 0.1189, Mantel–Cox test; Fig. 6B). Interestingly, we found that all Tp53 cKO mice with early morbidity (<50 weeks) presented tumors with increased Uhrf1 mRNA levels, suggesting spontaneous RB pathway inactivation (Supplementary Fig. 8F). High Uhrf1 mRNA expression correlated with increased Cdk4 expression (Supplementary Fig. 8G). No correlation was found with the expression of other RB regulators, including p16 and Cdk6 (Supplementary Fig. 8H, I). No significant changes on Rb1 expression were observed between these groups (Supplementary Fig. 8J). Histopathology analysis of tumors from the four mouse models analyzed linked Uhrf1 loss with lower mitotic index and decreased anaplasia (Supplementary Fig. 9 and Supplementary Table 2).
Most remarkably, in line with our in vitro observations, Uhrf1 loss resulted in a significant reduction of pulmonary metastases, with only 22.6% of Tp53/Rb1/Uhrf1 TKO mice presenting lung metastases compared to 52.4% of Tp53/Rb1 DKO mice. A smaller number of metastatic nodules was also observed in the Tp53/Rb1/Uhrf1 TKO mice that developed lung metastases (Fig. 6C).
To determine whether Uhrf1 contributes to tumor promotion or tumor progression, we performed periodic FDG-PET/microCT scans on Tp53/Rb1 DKO and Tp53/Rb1/Uhrf1 TKO mice to determine the age at which tumors are detectable (Supplementary Fig. 8A). In Tp53/Rb1/Uhrf1 TKO mice, tumors were detected significantly later than in Tp53/Rb1 DKO mice (P = 0.0362; Fig. 6C). All test subjects reached humane end-of-study within 3 weeks of tumor detection. These data suggest that Uhrf1 plays a pivotal role in the early developmental process of osteosarcoma promotion following the loss of Rb1.
留言 (0)