
記住我







This study draws on data from publicly available nationally representative 2017/2018 Bangladesh Demographic and Health Survey (BDHS). It is a cross-sectional survey administered by the National Institute of Population Research and Training (NIPORT). Technical assistance to conduct this survey was provided by the ICF International of Calverton, Maryland, USA. The survey was based on a two-stage stratified sampling of households. At the first stage, 675 enumeration areas (clusters) were drawn from a list of 296,718, which was prepared for the national population and housing census conducted in 2011 by the Bangladesh Bureau of Statistics [25]. Of the 675 enumerations areas, 672 were finally selected and the remaining three were excluded because of a flood. At the second stage, 30 households from each enumeration area were selected by systematic random sampling, and all married women aged 15–49 years in the selected households were included. More information regarding the survey sampling procedure and collected data have been published in the BDHS survey report [26].
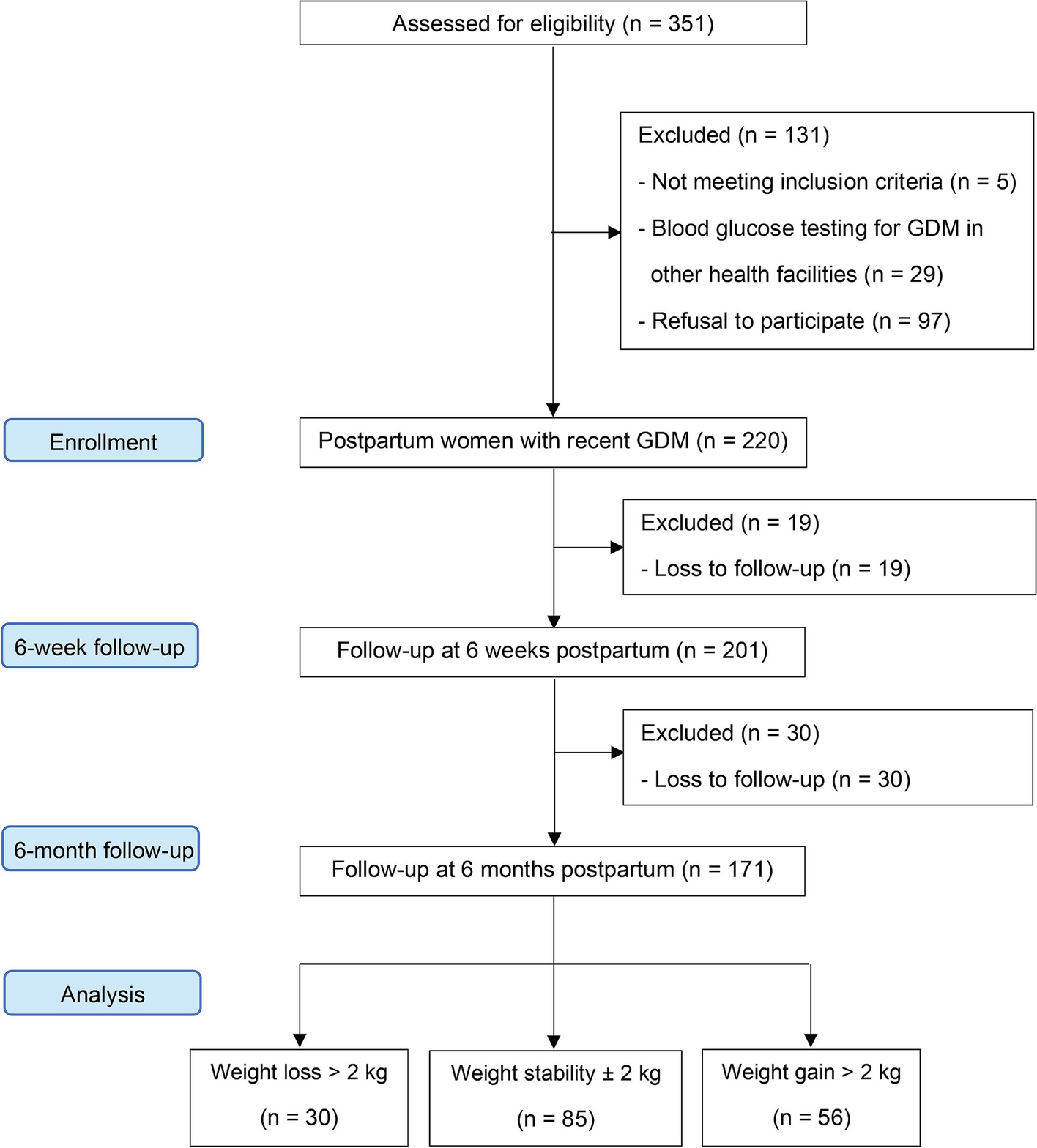
SampleOf the 20,127 reproductive-aged married women interviewed in the 2017/2018 BDHS, data of 4126 women were included in the analysis (Fig. 1). The inclusion criteria were (i) fecund women (by birth) who were not pregnant at the time of the survey, (ii) had at least one birth in the 3 years preceding the survey (from whom the pregnancy intention data were collected), (iii) not in the infertile period due to absence of ovulation and (iv) who had at least one episode of sexual intercourse in the month preceding the survey. Women’s responses to the following three questions were used to determine the ovulation status and the month in which women became fertile again: (i) have you had menstrual bleeding?; (ii) are you giving regular supplementary foods or fruits or fluids to your baby in addition to breastfeeding?; and (iii) is your infant older than 6 months of age? [27] Women who answered negatively to each of these three questions were identified as infertile due to the absence of ovulation during the survey and excluded from the analysis [27].
Fig. 1
Sampling strategy of the 2017/2018 BDHS and sample selection procedure for this study
Outcome variableThe pattern of women’s contraceptive switch from before to after pregnancy is our outcome variable. The variable was generated by comparing women’s contraceptive using patterns at two different times: (i) at the month of the most recent pregnancy that ended with live birth (will be expressed as before pregnancy hereafter) and (ii) at the month when women became fertile again following the live birth of the most recent pregnancy (will be expressed as after pregnancy hereafter). The BDHS recorded these data using the calendar approach, which is a validated approach and used worldwide. In this approach, women’s monthly reproductive history, including contraceptive methods, pregnancy and birth from the survey dates to the previous 5 years was recorded [28]. Women were asked to report the names of their monthly contraceptive methods from a list that included: no method use, oral contraceptive pill, injections, condoms, female sterilization, male sterilization, intrauterine device, implant/Norplant, periodic abstinence and withdrawal. A free-text response option was also given to record if method(s) of contraceptives used were not on the list. Where women reported multiple contraceptive methods, their most frequently used method was selected. Using this data, we first determined women’s contraceptive methods using patterns before and after the most recent pregnancy that ended with live birth. We then classified them as no contraceptive use (if no methods were used), traditional contraceptives use (used periodic abstinence and/or withdrawal) and modern contraceptives use (used oral pills, injections, condoms, male and female sterilization, intra-uterine devices and/or implants). Contraceptive switching patterns were then determined by comparing types of contraceptives used before and after pregnancy. The variable was categorised as follows: (i) no change (if women reported the same contraceptive method use before and after pregnancy), (ii) switched to higher effective contraceptives (if women switched from pre-pregnancy less effective contraceptive methods to post-pregnancy more effective contraceptive methods), and (iii) switched to less effective contraceptives (if women switched from pre-pregnancy more effective contraceptive methods to post-pregnancy less effective contraceptive methods). International guidelines were followed to determine the effectiveness of contraceptive methods for this comparison [29].
Exposure variablesThe main exposure variable was the intention of the most recent pregnancy. This information was collected from women who had at least one live birth within 3 years prior to the survey. Women were asked: (i) when you became pregnant with (name of the last child born within 3 years of the survey date), did you want to get pregnant at this time? If women responded affirmatively, responses were categorised as wanted pregnancy. If women responded negatively, their pregnancies were identified as unintended. They were then asked: did you want to have a baby later on, or did you not want any more children? Responses were recorded as “later” and “no more/none”. Responses were then categorised as mistimed pregnancy (if the answer was “later”) and unwanted pregnancy (if the answer was “no more/none”).
Potential confounding variables were identified by a comprehensive literature search on the determinant factors of contraception use [12,13,14,15,16,17]. Respondents’ level factors included were women’s age at birth of the last child (≤ 19, 20–34, ≥ 35), desire for more children (within 2 years, after 2 years, and no more children wanted), women’s educational status (no formal education, primary, secondary, and higher), and parity (one child, two children, three or more children). Husbands’ educational status (no formal education, primary, secondary, and higher), occupation (agricultural worker, services and non-agricultural labor, business, and others), and household wealth quintile (poorest, poorer, middle, richer, and richest) were also identified as potential covariates. Other factors were residential locations (urban, rural) and seven administrative divisions of residence (Barishal, Chattogram, Dhaka, Khulna, Mymensingh, Rajshahi, Sylhet).
Statistical analysisWe used descriptive statistics to characterise the demographic profile of women and two-sample proportion tests to assess the significance of the differences in contraceptive methods uses before and after the most recent pregnancy. In the BDHS, respondents included are nested in the households, and households are nested in the clusters. Therefore, responses from the same household and cluster are more likely to be similar and behave more alike than a different household and cluster. Multilevel regression is an appropriate approach for this type of hierarchical data [30]. Therefore, we used multinomial multilevel logistic regression to examine the association between the intention of the most recent pregnancy occurring within the 3 years prior to the survey and women’s contraceptive methods switching patterns from before to after pregnancy. The presence of multicollinearity was checked among variables using Variance Inflation Factors (VIF) at a cut-off point of 10. If VIF was more than 10, the relevant variable was deleted. Results were reported as adjusted odds ratios (aOR) with 95% confidence intervals (95% CI). All statistical analyses were conducted using Stata software version 15.1 (Stata Corp, College Station, Texas, USA).
留言 (0)