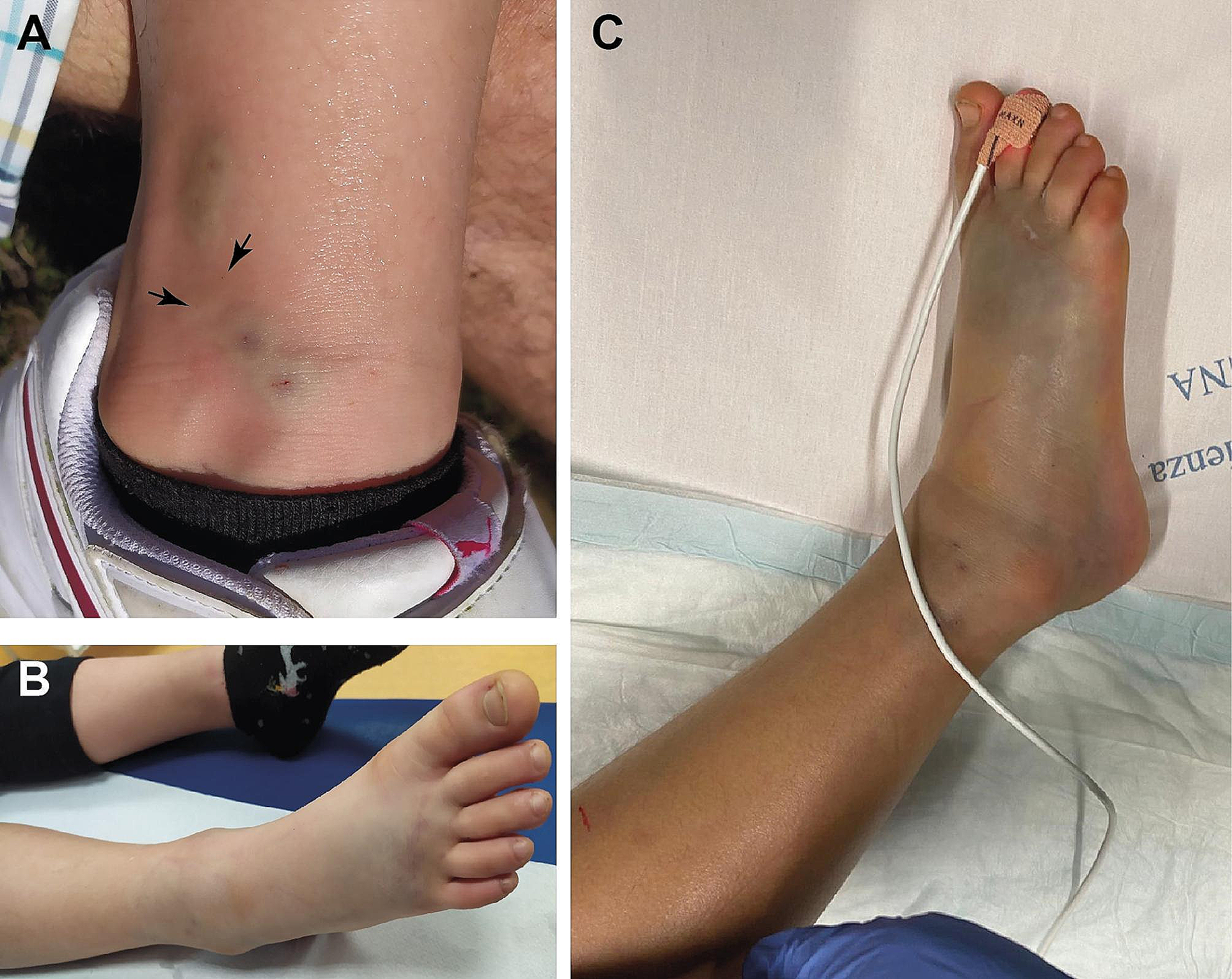
Acyl-coenzyme A (CoA) dehydrogenases (ACDHs) are a family of mitochondrial flavoproteins actively involved in mitochondrial fatty acid β-oxidation (FAO), branched chain amino acid (BCAA) catabolism and amino acid catabolism [8]. These enzymes require oxidised flavin adenine dinucleotide (FAD) as cofactor. FAD continuous re-oxidation is provided by the concerted action of ETFs and ETFDH [9]. Mutations in the genes codifying for these flavoproteins give rise to a variety of different inborn errors of metabolism, so-called MADD, characterized by the impairment of the FAO and BCAA catabolic pathways responsible for downstream effects that explain the typical phenotype and the peculiar laboratory findings observed in our patient [2, 5, 6, 9, 10]. FAO is deeply involved in ATP production pathway in the heart, kidney and skeletal muscle, together with glycolysis. In MADD, its defective activity causes a compensatory hyper activation of glycolysis and glycogenolysis to ensure the right ATP provision necessary for the correct functioning of cellular processes [11]. The dysfuction of Glutaryl CoA Dehydrogenases due to mutation in ETFs or ETFDH leads to increased accumulation of glutaric acids, which is responsible for metabolic acidosis that doesn’t benefit from aggressive treatment with bicarbonate boluses [12]. The defective mitochondrial fatty acid beta-oxidation processes negatively influence acetyl-COA production, with accumulation of large amounts of fatty acyl-COA species and of the corresponding acylglycine and -carnitine coniugates, increased lipid accumulation in the liver and muscles, high blood methionine and phenylalanine levels, and decreased ketone body and blood glucose levels [11]. Lipid accumulation is observed in the tissues including the liver, heart and renal tubular epithelium, which use fatty acids as a primary source of energy. Colevas et al. speculated that the malformations might be the consequence of an accumulation of toxic metabolites that is not corrected by placental transfer [13]. Formal clinical diagnostic criteria for MADD have not been established. The diagnosis is suspected on the basis of the combination of clinical and supportive specific and non-specific laboratory findings and requires confirmation by identification of biallelic pathogenic variants in ETFA, ETFB, or ETFDH genes. Our patient had growth retardation, with reduced OFC, ogival palate, low-set ears, bilateral syndattilia of the 2th and 4th toes and empty scrotum as well as loss of cortico-medullary differentiation of the kidney. This is coherent with the description of congenital alterations occurring in type I MADD including dysmorphic facial features (high anterior hairline, wide nasal bridge, short nose with anteverted nares and long philtrum, tented upper lip, midface retrusion), single palmar creases, rocker-bottom feet, hypospadias with or without chordee in males. Renal malformation with large cystic kidneys and antenatal oligohydramnios, cardiomyopathy and hepatomegaly may also be seen. Non-specific laboratory findings include nonketotic or hypoketotic hypoglycemia, with blood glucose often less than 45 mg/dL, hyperammonemia, elevated liver transaminases (AST, ALT). The absence of ketones at urinalysis in the setting of hypoglicemia is an important laboratory marker that may contribute to clinically differentiate MADD-related hyperlactatemia from other conditions linked to primitive metabolic defects of the Krebs’ cycle before NBS results have become available. The condition of hyperglycemia recorded in our patient instead of hypoglycemia may be the consequence of the parenteral nutrition in the first days of life. Strongly suggestive for MADD is the typical plasma acylcarnitine profile evidenced on blood dried spot by the tandem mass spectrometry analysis, with elevations of C4, C5, C5DC, C6, C8, C10, C12, C14:1, C16, and C18:1 acylcarnitine [5, 6, 10, 14] The urine organic acid analysis reveals a combination of increased excretion of glutaric-, ethylmalonic-, adipic-, suberic-, sebacic-, dodecanedioic-, 2-hydroxyglutaric-, 3 -, and 5- hydroxyhexanoic acid, in conjunction with C4 and C5 glycine conjugates i.e. isobutyrylglycin, isovalerylglycine, hexanoylglycine, suberylglycine. The urinary excretion of hydroxy isovaleric acid explains the unpleasant feet smell of the patient’s urine. However, the diagnosis may be challenging in late-onset cases since the biochemical abnormalities may be mild, atypical or only detectable during metabolic decompensations [15].MADD differential diagnoses include disorders of riboflavin metabolism with similar biochemical findings or overlapping phenotypic features, like the severe congenital anomalies associated neonatal-onset form of carnitine palmitoyl transferase II deficiency, and the neonatal transient MADD-like illness. The latter lacks birth defects and is caused by a maternal riboflavin deficiency sustained by a heterozygous pathogenic variant with secondary neonatal riboflavin deficiency, that dramatically improve after riboflavin supplementation [16]. Molecular genetic testing is mandatory to confirm the diagnosis. MADD is inherited in an autosomal recessive manner, caused by loss-of-function variants. A recent systematic review has identified 36, 19 and 280 pathogenic variants of ETFA, ETFB and ETFDH genes, respectively [11]. Homozygous or compound heterozygous null pathogenic variants or pathogenic variants that severely affect mRNA expression or stability result in a complete loss of protein expression or function and cause the most severe form of MAD. Instead, pathogenic variants involving the active site and/or pathogenic splice site variants give rise to very low residual enzyme activity, leading to neonatal onset without congenital malformations. Missense mutations not affecting the active site, mRNA expression, or stability have relatively high residual activity, and subsequently cause milder, late-onset disease (type III) [3]. Next-generation sequencing genetic analysis revealed a homozygous indel variant c.606 + 1 _606 + 2insT in the ETFDH gene, localized in a canonical splite site. This indistinct variant, segregated from the two heterozygous parents, is not present in the general population frequency database and has never been reported in the literature. In silico analyses predict that this variant is probably damaging to protein structure and it can be assigned to class IV according to standard guidelines of the American College of Medical Genetics and Genomics [17]. In this case, the diagnosis of MADD by expanded neonatal screening arrived the day the newborn died, simultaneously to the results of typical plasma acylcarnitine profile and urine organic acid analysis, which were consistent with the diagnosis. This case underlines the importance of expanded newborn screening in the diagnosis of congenital metabolic diseases which may present complex clinical pictures at birth. For that reason, the collecting of blood sample in the first days of life is essential and should be always performed. Moreover, the recognition of new mutations in the ETFDH gene, such as in this case, may improve also the quality of genetic counseling for parents who desire a new pregnancy.




留言 (0)