
記住我
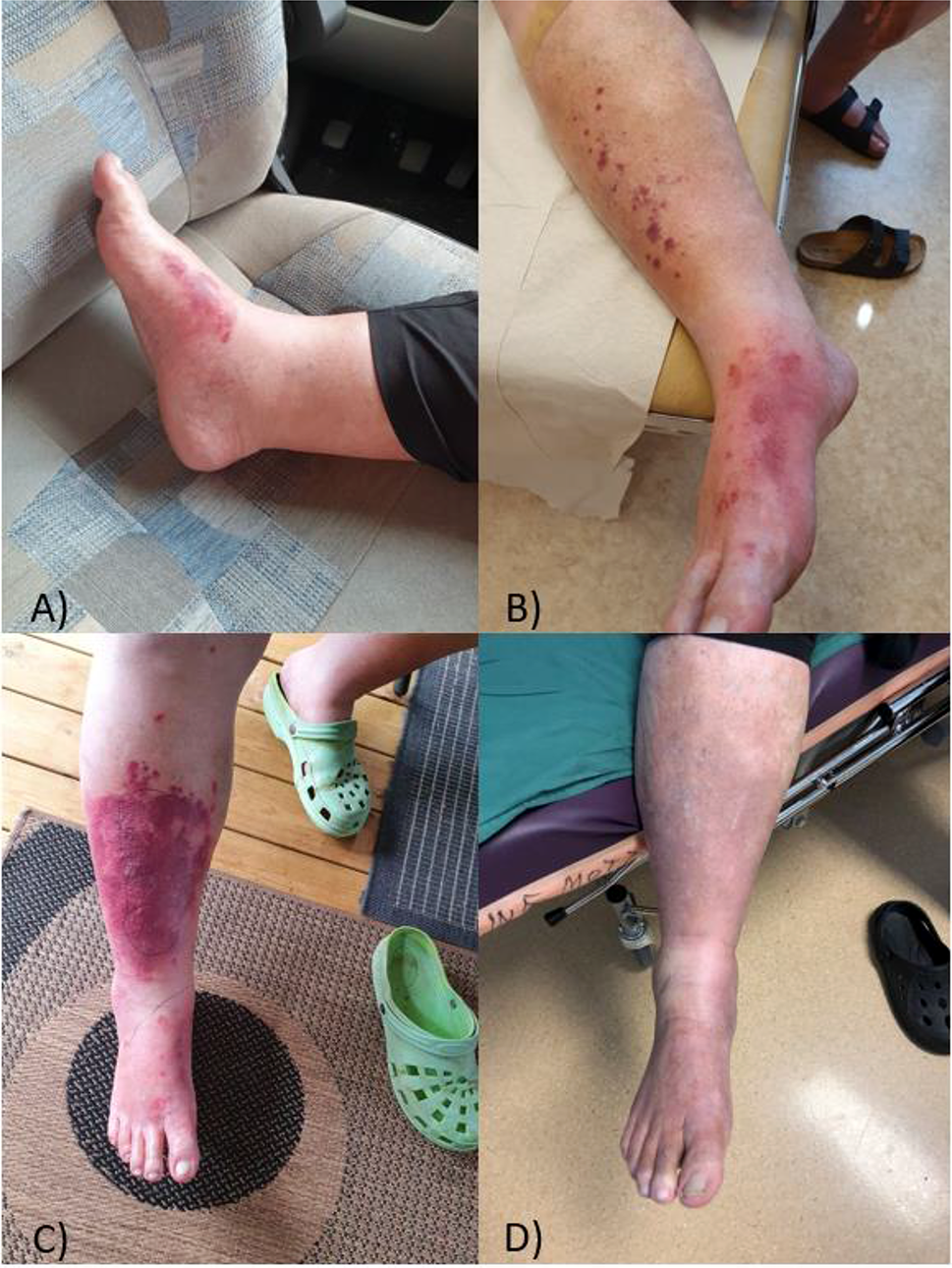
A 43-year-old female professional technician from Nanbu County, Sichuan Province, was admitted to our hospital on 1 September 2020 with complaints of “repeated fever with superficial lymphadenopathy and systemic rash for 5 months.” The patient had no obvious cause of fever for 5 months before admission, with a maximum temperature of 41 °C. Multiple subcutaneous nodules with a diameter of approximately 1 cm could be palpated in the neck, armpit, and groin and were accompanied by multiple rashes on the face and body (Fig. 1). There was no pain, itching, or burning sensation while walking; no hypoesthesia of the eyes, hands, or feet; no movement disorder of the limbs; no chills or shivering; no headache or dizziness; no chest tightness or shortness of breath; and no abdominal distension or pain. After treatment with ibuprofen in the local clinic, her body temperature temporarily normalised but repeatedly rose again. A left inguinal lymph node biopsy was performed at a local hospital. Histopathological examination revealed lymphoid tissue hyperplasia, granulomatous structures with necrosis, and immunohistochemical staining for histiocytic necrotising lymphadenitis. The patient was diagnosed with histiocytic necrotising lymphadenitis and pleomorphic erythema. Therapy including levofloxacin and prednisone acetate (30 mg/day) was administered. Subsequently, the patient's temperature and systemic erythema decreased; thus, levofloxacin was stopped, prednisone acetate was reduced to 20 mg/day, treatment was maintained, and the patient was discharged from the hospital. At 1 month before admission, the patient again had a fever, and her temperature did not significantly decrease after treatment in the local clinic. As a result, the patient visited our hospital. Physical examination on admission indicated the following: body temperature 36.9 °C, pulse 93 beats/min, respiration 20 breaths/min, and blood pressure 106/78 mmHg. Visible and palpable enlarged lymph nodes under the chin, bilateral armpits, and groin were approximately 1 cm in diameter, hard, tender, and fixed. Pleomorphic erythema was present on the face and over the body. The lesions were approximately 2–7 cm in size, with some protruding from the skin but not accompanied by ulceration or secretion. Physical examination of the heart, lung, abdomen, perineum, spine, limbs, and nervous system revealed no abnormalities.
Fig. 1
Skin lesions on the patient’s face (A and B) and right lower leg (C)
Blood examination after admission showed that the total number of leukocytes was 7.94 × 109/L, the percentage of neutrophils was 85.6%, and the absolute value of neutrophils was 6.80 × 109/L. There was no obvious abnormality in the absolute value and proportion of other blood cells. Among inflammation indicators, C-reactive protein (CRP) was 243.00 mg/L, and procalcitonin (PCT) was normal. Pathogenic microorganism examinations, including virus (including EB, cytomegalovirus (CMV), rubella, and herpes simplex viruses), toxoplasma, fungus, tuberculosis, and blood cultures, were all normal. Immunoglobulin IgG, IgA, IgM, and IgE were normal, complement C3, C4, rheumatoid factor, antineutrophil cytoplasmic antibody ANCA, antinuclear antibody Ana, anti-double-stranded DNA antibody, anti-SM antibody, anti-SSA, SSB antibody, anti-Ro52 antibody, anti-ScL-70 antibody, and anti-Jo-1 antibody were also normal. Lupus anticoagulant screening time (La 145.30 s), diagnosis time (La 232.30 s) and La1/La2 (at 1.40) were normal. immunoglobulin G4 subtype (IgG4) was normal, and there was no abnormality in urination and stool tests. The results of colour Doppler and transesophageal echocardiography were also normal, eliminating infective endocarditis. Chest computed tomography (CT) revealed minor inflammation in the right lower lung. Based on the above clinical manifestations, systematic examination results, and consultation among the Dermatology and Rheumatology Immunology Departments, the potential aetiology of recurrent fever and pleomorphic skin lesions was not identified.
To further determine the cause of these irregular phenomena in this patient, after obtaining the patient’s consent, left inguinal lymph node resection and biopsy were performed. The pathological diagnosis was lymphoid tissue hyperplasia with necrosis and neutrophil infiltration. Immunohistochemistry (IHC) found positivity for some markers, including CD20 (+, part), CD79a (+, minority), CD3 (+, part), CD5 (+, part), CD30 (+, minority), necrotic MPO (+, part), CD123 (+, part), and Ki-67 (+, 20–30%). Intriguingly, some positive bacilli were observed by acid-fast, silver hexamine, and periodic acid-Schiff (PAS) staining. However, DNA fragments of Mycobacterium tuberculosis (MTB) were not identified by qPCR. Flow cytometry showed no abnormally expressed populations of T, B, and NK lymphocytes. Combined with the results of pathological morphology, immunohistochemistry, and special staining, mycobacterial infection was considered, though it was difficult to determine which species.
Considering the advantage of second-generation gene sequencing in distinguishing rare infectious diseases, a skin biopsy of the right leg flexor erythema was performed, the pathological examination and second-generation gene sequencing of fresh biopsy tissue were performed simultaneously. The pathological diagnosis showed a large number of lymphocytes, plasma cells, neutrophils, and histiocytes in the dermis and subcutaneous fat and around blood vessels. IHC also revealed positivity for some proteins, including CD3 (partial +), CD7 (partial +), CD8 (partial +), CD4 (partial +), and CD20 (partial +). Acid-fast staining showed that a large number of positive bacilli distributed in the dermis and subcutaneous fat (Fig. 2). However, the PCR did not detect any DNA fragments of Mycobacterium tuberculosis. In conclusion, our results were consistent with those of Mycobacterium infection; however, the species could not be confirmed by PCR or special antibody tests in our institute. The results of second-generation gene sequencing suggested the presence of Mycobacterium leprae (Table 1) but no other types of mycobacteria; thus, the patient was finally diagnosed as leprosy with erythema nodosum leprosum (ENL) [11, 12], characterized by erythema multiforme-like skin lesions, lymphadenopathy, fever, elevated CRP concentration, and histological perivascular infiltrate of neutrophils.
Fig. 2
Pathological HE staining (A) and acid-fast staining (Ziehl–Neelsen) (B) of skin biopsy of the right leg. Scale bar: 20 μm
Table 1. High throughput gene detection results of pathogenic microorganismsSince the pathogens of leprosy tend to affect the nerve system and loss of sensation in skin lesions is a cardinal sign in diagnosing leprosy, a careful nervous system physical examination was performed again, such as Shallow sensation of limbs, body and all skin lesions, which was evaluated in pain, touch and temperature. shallow reflex including corneal reflex, pharyngeal reflex and abdominal wall reflex; deep reflex including biceps brachii reflex, triceps brachii reflex, radial membrane reflex, knee reflex and heel reflex; pathological reflex including Hoffman sign, BABINSKY sign and Kirschner’s sign. Finally, the vision was also assessed. However, no abnormality was found.
The administration of prednisone acetate was stopped for this patient once the leprosy diagnosis was made. Due to a lack of leprosy treatment drugs in our hospital, this patient was referred to the Institute of Dermatology and Venereal Diseases. A therapy consisting of dapsone, rifampicin, and clofazimine was administered. The patient’s fever was controlled at 3 days after treatment, and her systemic erythema and superficial lymph node swelling were reduced at 3 months after treatment. At 1 year after treatment, the patient was followed up by telephone. Her temperature was normal, a few erythemas were present on the face, and her axillary lymph nodes were slightly larger, with no other uncomfortable symptoms.
留言 (0)