
記住我
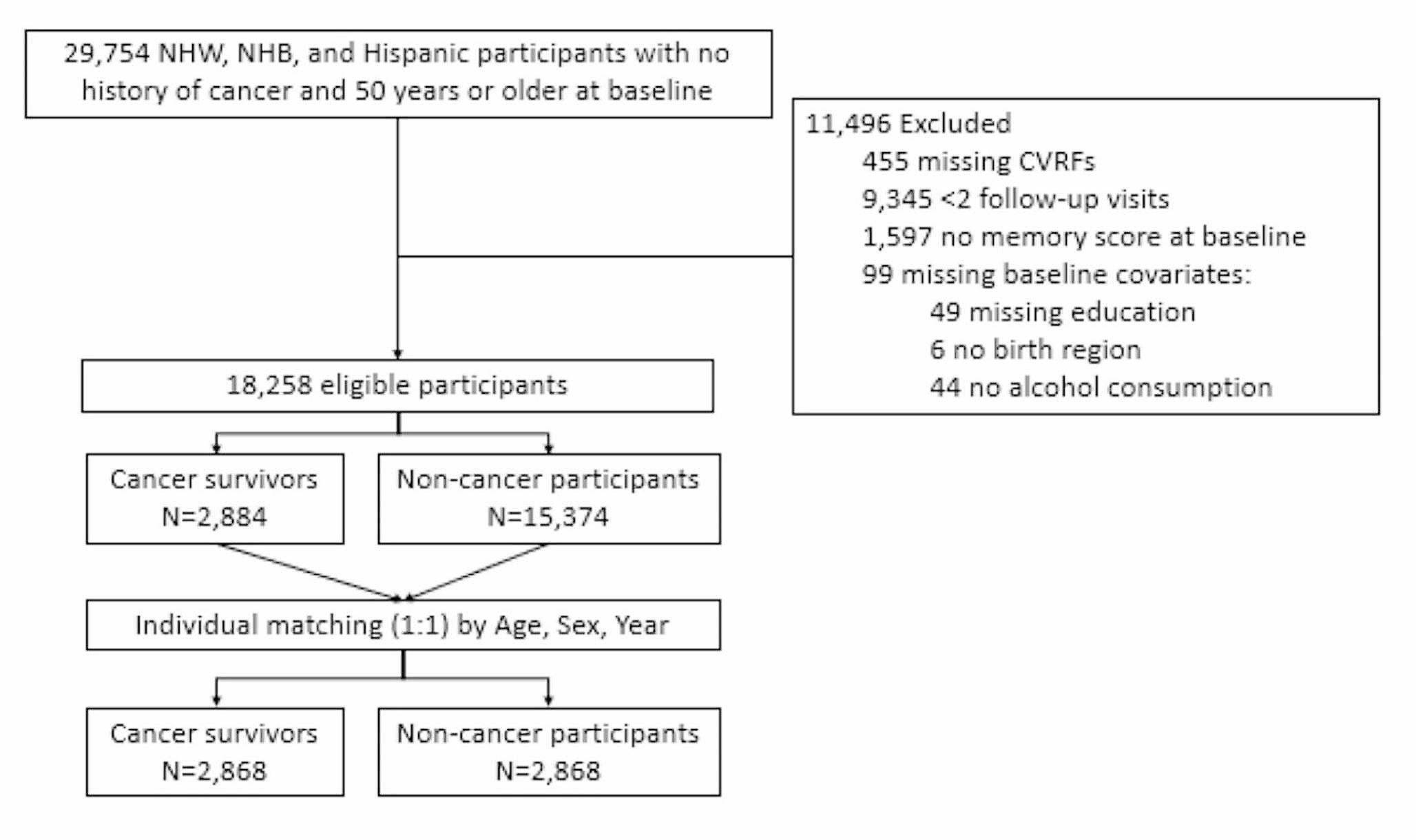


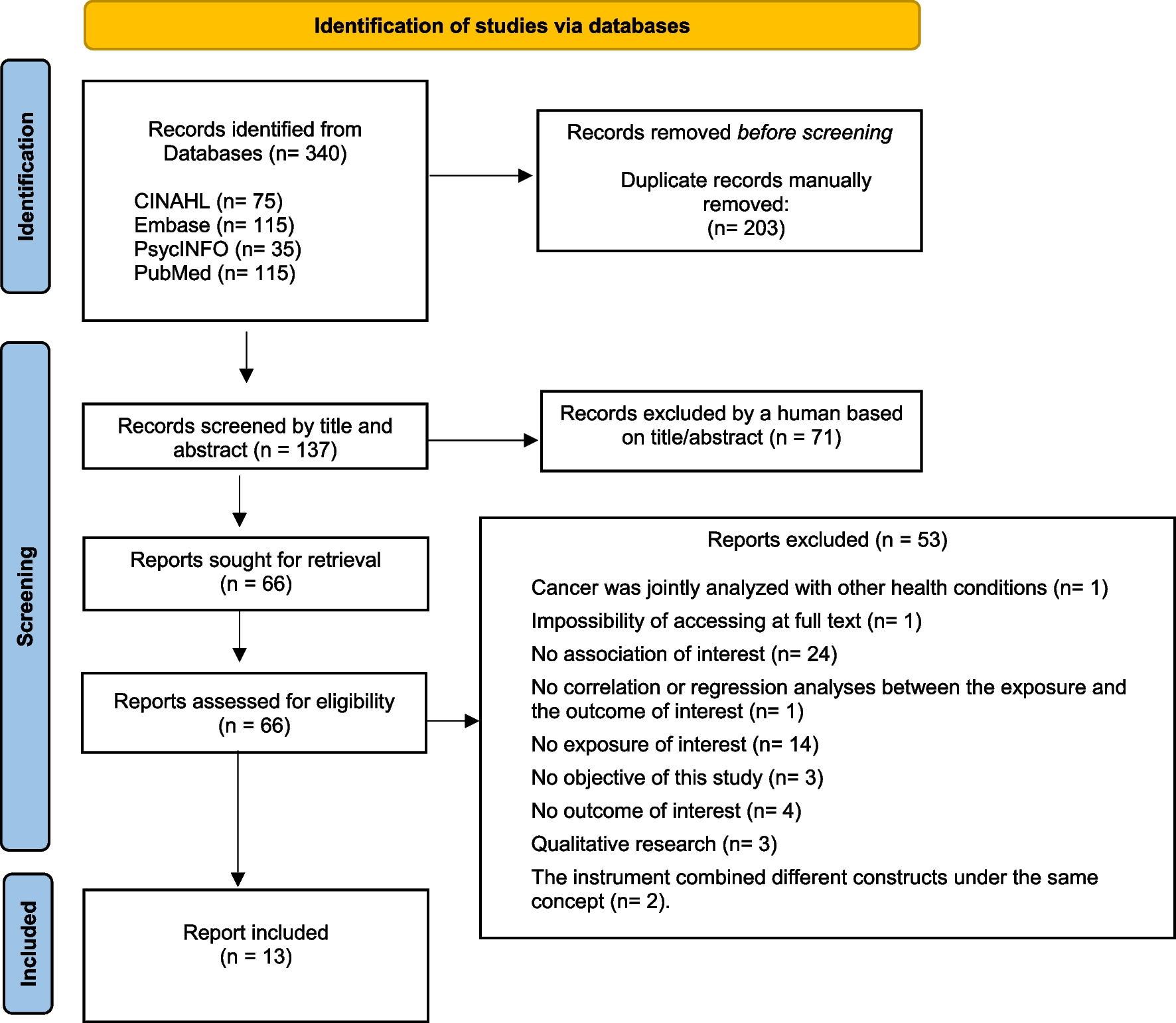
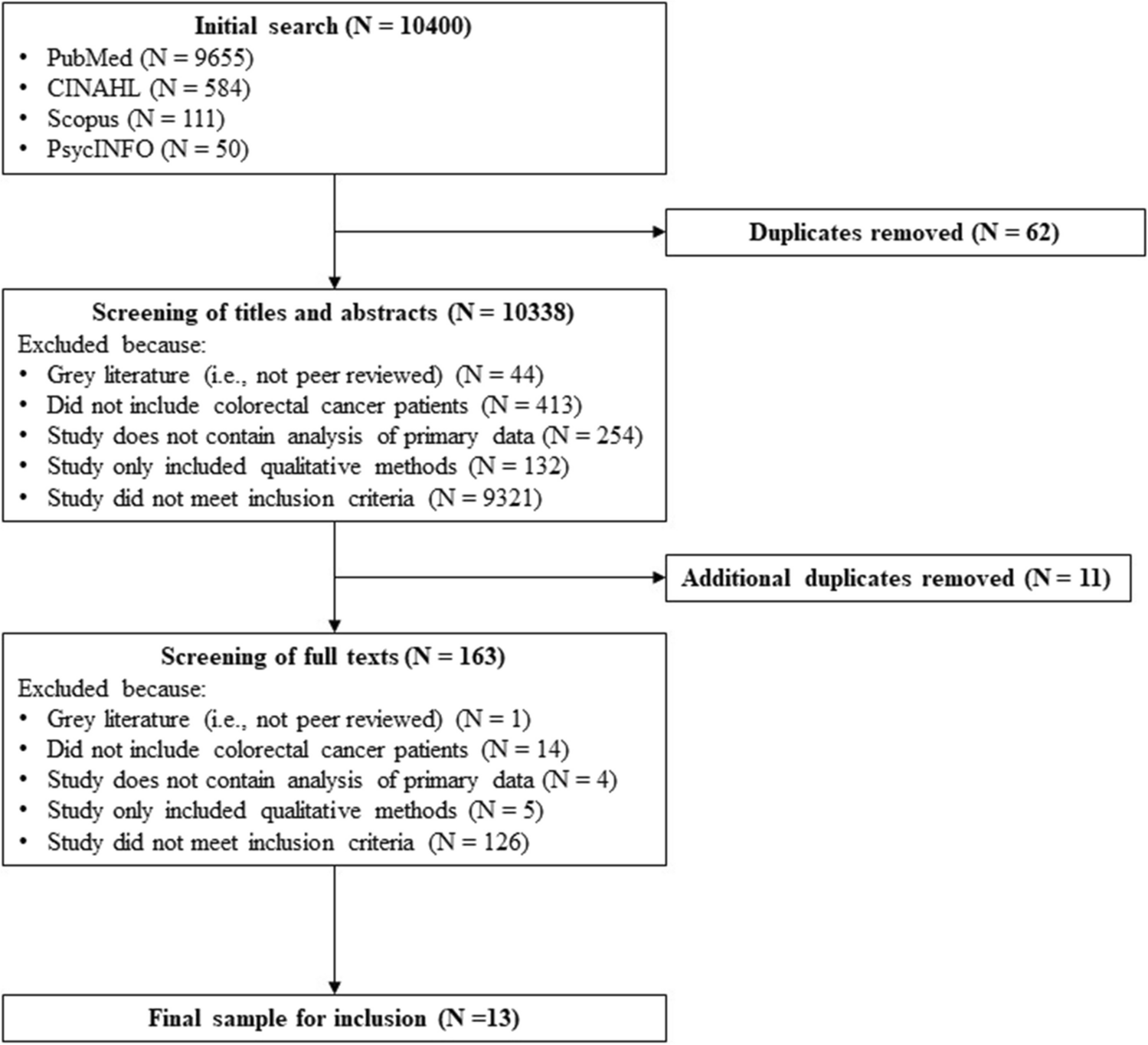
Database searches retrieved 7372 records and 4133 records remained after exclusion of duplicates. Following screening by title and abstract, inclusion and exclusion criteria were applied to 103 full text articles. Of these articles, ten articles [11, 26,27,28,29,30,31,32,33,34] fulfilled inclusion criteria, of which one was identified through back citation (see Fig. 3).
Fig. 3
PRISMA flow diagram showing records included through systematic search of the literature
There were five qualitative studies [11, 27, 30, 31, 33], four surveys [26, 28, 32, 34] and one letter to the editor [29] which identified views of CCRs from patients (n = 3) [11, 29, 30, 33], their partners who were sometimes also carers of patients (n = 1) [27], and healthcare professionals(n = 5) [11, 26, 28, 29, 31,32,33], including primary care professionals (see Table 1). There was one study measuring the impact of CCRs performed via group consultations [34]. There were no studies identifying validated outcome measures to evaluate CCRs, the impact of CCRs on quality of life (patients or their carers or spouses) or patients’ symptoms.
Table 1 Summary table of included studies in scoping review on cancer care reviews (CCRs). These included online surveys, interviews and focus groups. n/a, not applicable. None of the papers reported disability. GPs, general practitionersIn surveys[26, 28] involving healthcare staff, 25–38% respondents were female whilst gender was not reported in an interview study[31], a focus group study[11], or a trial [34] involving healthcare professionals. Fifty percent of patients interviewed for one study were female[11] and another study only included participants who had endometrial cancer[30]. An interview study[27] involving partners of patients had 68% female participants. No studies reported data on disability and some studies[11, 26, 28, 31,32,33,34] did not report ethnicity. In those that did report this[27, 30], 5–6% of patients or partners were from ethnic minority groups.
Patient views on cancer care reviewsThis data was sourced from interviews with patients in GP practices with various cancer types within 6 years of diagnosis (n = 38) [11] and within 3 months of diagnosis (n = 16) [33], interviews with patients (n = 17) from gynaecology outpatient clinics diagnosed with stage I endometrial cancer within the last year [30], and a letter from a GP who had been diagnosed with cancer [29]. Adams and colleagues[11] conducted interviews with patients within three years of their cancer diagnosis, where just 5% (n = 2) recalled a CCR and more than half (n = 20) could not recall any detailed discussion with their primary care team. This was echoed in the study by Kendall et al. [33] where few patients could not remember either having a specific proactive cancer related appointment or a CCR. A more recent qualitative interview study [30] conducted with patients with stage I endometrial cancer indicated that some were unsure of what a CCR involved, and the difference compared to a routine GP appointment. Only those who reported the existence of a good relationship with a GP were positive about CCRs with some not keen to discuss their cancer diagnosis with unfamiliar practitioners in a supplementary appointment dedicated to CCRs: “Well the thing is, I don’t feel comfortable with my GP because the one I had is retired. And every time I go to phone up now, I get somebody different. And I've built no relationship up with them. They don’t know me, they don’t really know my condition.” (ID 11, page 6) [30].
A letter [29] written by a GP who had a cancer diagnosis suggested that CCRs and their associated funding is important to provide an access route to primary care: “QOF cancer care reviews can provide a valuable doorway allowing patients to access this support. As a patient, I vote that they should remain.”
Those patients that had CCRs (n = 2) [11] did not find them particularly helpful as primary care staff seemed unaware of the patient’s history and ongoing cancer treatment, which may be in part not reading clinical notes, and a general lack of awareness of novel cancer treatments:
“They invited us to go and see them as a follow-up, but she was not aware of the operation I’d actually had, and she was not aware what they had in fact done, and she, sitting discussing with her ‘they really do that now do they?’” (P20, 68-year-old male, pages e176-7) [11].
“He hadn’t looked at the notes, it was almost like I kind of went through ‘this is what I’ve got, these are the drugs I’m having’, which was … Trying to remember all those, so it wasn’t really, there was no value to me at all at that point frankly, it was a bit of a waste of time quite honestly.” (P16, 36-year-old male, page e177) [11].
Patients were unsure about the right time for a CCR with some preferring a review with primary care soon after diagnosis and others preferring contact at the end of treatment or several reviews during cancer treatment. A proactive approach to cancer care via a CCR would legitimise concerns to seek help in primary care and patients mentioned several things that should be included in primary care cancer-specific reviews, but which are not formally part of CCRs. These included the following: illness acknowledgement, an explanation of cancer in lay terms, support for children, emotional and psychological support for themselves and, information about the symptoms of recurrence, travel insurance, and local support groups.
Patients recognised that barriers to providing cancer care, which may include CCRs, in GP practices may arise from lack of coordination between primary care and secondary care, with some secondary care professionals denigrating the value of GPs in cancer care: “I fear that there’s no consistency between specialists and GPs, because I like to feel as though I trust my GP, but when they start bickering about ‘oh your GP doesn’t know anything’, you can be easily swayed, and you say, ‘should I be talking to my GP about this?’.” (37-year-old male, page e178) [11].
Others recognised lack of time as a potential barrier to providing a CCR within a 10-min consultation which stopped patients raising concerns with GPs or practice nurses about their cancer:
“Some sort of follow-up thing would be nice because there are things you’d like to ask because when you do come back here for your check-up they’re so pushed for time, you haven’t, they obviously haven’t really got a lot of time.” (P52, 74-year-old male, page e178) [11].
Partner views on cancer care reviewsInterviews with partners of patients (n = 22) who had been diagnosed with various types of cancer within the last 3 years were the only data source. Most partners of patients [27] (n = 17, 77%) who had various types of cancer were in favour of having their own cancer care review, designated review time, to discuss symptoms of recurrence for the patient: “I’d like maybe to talk about the likelihood of it coming back, or him developing a different kind of cancer, touch wood, that would put my mind at rest…” (P155, wife, separate interview, page 2791) [27].
Other partners thought that having a personal CCR appointment for themselves would allow them to stay up-to-date with their fellow partner who was undergoing cancer treatment: “Yes, that would be a good idea, yes, yes, it’s best to know what’s going on, I mean if you have it first hand you know the governor is not giving you a load of cobblers to keep you quiet, don’t you, no, I think that would be a very good idea” (P1214, husband, separate interview, page 2791) [27].
A dedicated appointment for a partner would provide an opportunity to discuss their own concerns relating to their own health but specifically being a carer: “We’re coping OK, but given all the things I’ve read about carers, getting stressed and all that kind of thing, it does surprise me that now this has been happening for 18 months, nobody has ever suggested that I should just have a check up, or talking to me to see if I’m caring [sic] …” (P174, wife, separate interview, page 2791) [27].
Partners of patients with cancer found that primary care tended to be for patients rather than for carers. This acted as a perceived barrier to seeking help about their own health or caring needs. Others found that the confidentiality of the doctor-patient relationship limited disclosure of information relevant to their caring responsibility, such as when discussing patient care at a dedicated appointment for the partner. Furthermore, partners thought that primary care professionals lacked knowledge of family roles, such as knowing the partner or main carer.
Primary care professional views on cancer care reviewsProfessional views were derived from a variety of sources: a 2010 survey of 100 oncologists and 200 primary healthcare professionals with an audit of oncology discharge letters [26], a 2015 survey of 500 GPs [28], a 2020 survey of 123 GP practice nurses [32], a 2011 focus group of 6 GP multidisciplinary teams [11], a 2013 interview study of 29 primary healthcare professionals [33], and a 2020 interview study with 19 primary and secondary care clinical and managerial staff[31].
Understanding of CCRsOnly one survey checked understanding of the concept of CCRs and found that of those practice nurses who were clear in supporting patients with cancer, 43% (n = 32) did not correctly understand or were unsure about the purpose of CCRs [32].
How CCRs are carried outSurvey data of GP practices and primary care staff identified that most CCRs were performed by GPs. In a survey of 200 GPs [26], 98% performed CCRs themselves but some practices reported delegating this to practice nurses (14%), district nurses (19%), palliative care nurses and community matrons (6%). In the same survey, just over half the GPs (51%) conducted CCRs opportunistically during a consultation with a similar proportion (45%) reported by Walter and colleagues [28] in a survey of 500 GPs. This was similarly reflected in focus groups with primary care teams where CCRs were completed opportunistically in person or on the telephone [11]. There was no consensus on the optimum timing of CCRs and very few performed CCRs at a set time point. Only 17% were performing CCRs at a set time whilst 5% were performing regular reviews in the study by Watson [26]. In the same study, 39% aspired for CCRs at different times of the patient journey such as at diagnosis (62%), end of outpatient follow-up (53%) and six-monthly (60%).
Between 40 and 64% of GPs used a CCR template or structure [26, 28] with practice or local CCG templates being the most popular [28]. However, participants in focus groups [11] and interviews [33] had mixed views on the value of templates in CCRs with some GPs finding them a useful structure and others thinking CCRs were a “tick-box exercise”—thereby fundamentally changing the consultation structure:
“I don’t think it’s of any value personally, I don’t think it’s to the patient benefit at all, I think it’s just another hoop you have to jump through if you want to get paid.” (practice 5, GP partner, page e179) [11].
“I do have slight anxieties about making everything so structured, I mean the ethos has always been “we’re accessible, we’re here if you want us, if you do come in we don’t have to follow a template, we can go by your agenda, and what you’re worried about”, and I have concerns about templates.” (practice 2, GP partner, page e179) [11].
Some GPs and practice nurses found that filling the CCR documentation with the patient was mutually beneficial and improved clinical practice and documentation [33].
One GP [29] who had experience of having cancer treatment identified a potential driver for cancer care review as ticking of the financial incentive, Quality and Outcomes Framework (QOF) box. This was corroborated by two participants of a study by Williamson [31] including healthcare professionals, managers and commissioners interviewed, who suggested that financial incentives may support related initiatives such as holistic needs assessments which inform CCRs.
Walter and colleagues [28] found that 53% of GPs found CCRs useful whilst 10% did not specify in which regard. GPs who performed CCRs with a template and those who made specific appointments were more likely (48% and 327%, respectively) to find CCRs useful compared to those who did not use templates, or performed CCRs opportunistically. GPs with specific appointments for CCRs found CCRs three times more useful even after adjusting for template use compared to those that performed CCRs opportunistically. Watson [26] reported 40% of primary care staff found CCRs useful to staff and 60% found them useful to patients.
A 2010 [26] and 2015 [28] survey showed that most GPs (> 50%) discussed psychological symptoms and support during CCRs. However, Watson[26] in 2010, found that in addition most GPs reviewed treatment, patient follow-up and discussed family needs. Walter’s [28] more recent survey found that most GPs discussed treatment-related side effects and lifestyle. However, Watson [26] in 2010 found 68% of GPs discussed social support, such as work and finances, compared to 36% of GPs in 2015 [28]. In addition, 19% fewer GPs discussed lifestyle or healthy behaviours in 2010 [26] compared to 2015 [28]. The content of CCRs in Walter’s study [28] such as lifestyle advice or social support was significantly related to GP confidence in discussing these topics. Only a minority of GPs provided information on symptoms of recurrence, familial or genetic risks of cancer, and screening requirements in Watson’s study [26]. These topics were not included in the survey by Walter and colleagues [28]. A 2020 survey of practice nurses [32] found practice nurses were more confident in discussing hormone treatment and surgery but less confident in discussing immunotherapy. Furthermore, practice nurses were more confident in discussing physical and mental health problems as well as lifestyle advice such as smoking cessation. However, they were less confident at discussing long term effects such as sexual dysfunction or the effect on fertility alongside signs of recurrence and the need for follow-up testing.
Barriers to the implementation of CCRsImplementation of CCRs, as part of the Recovery Package, by clinicians and policymakers was noted to be difficult at a time of ‘decreasing resources’[31]: “We’re already having talks with our commissioners which are being led by our local cancer network to look at how we can jiggle the funds around really and commission the Recovery Package activity, but that would be on the proviso obviously that we reduce the follow-up ‘cos there won’t be more money and we’ve got a lot more patients coming in …’” (ID 11 Lead Cancer Nurse, page 4) [31].
This allusion to a lack of time to conduct CCRs was reflected in Adams and colleagues’ paper [11]: “One of the things really struck me was the patients really wanted a lot of information, and to some extent I think the sort of cancer care review process is probably not the place for that, I mean I think a few good websites and information sheets or a few helplines for the patients, they could actually be more useful, I think you could do a lot of that outside of a GP setting, if there was more sort of an information infrastructure that would be helpful.” (practice 3, GP partner, page e180) [11].
Other barriers to implementation of CCRs by the primary care team included lack of knowledge in long-term cancer care [11]: “I also feel you know, I probably don’t know enough about the subject to give advice, but I think from an emotional point of view, yeah, you just sometimes you just have to listen, don’t you.” (practice 5, practice nurse, page e180) [11].
This was more evident on a survey [28] including a measure of
留言 (0)