
記住我






Orbital cavernous venous malformation (OCVM), also known as cavernous hemangioma, is classified as a slow-flow venous malformation by the International Society for the Study of Vascular Anomalies (International Society for the Study of Vascular Anomalies issva.org/classification). Surgical excision is typically recommended for symptomatic lesions.1 Although several external surgical methods have been employed, removing the OCVM at the deep orbital apex remains challenging due to the intricacy of the neurovascular anatomy and its proximity to visually critical structures like the optic nerve or vessels.2 The limited visibility and maneuverability of the instruments are other challenges.3 Here, we present an endonasal endoscopy-assisted removal of the orbital apex OCVM compressing the optic nerve with the addition of an inferomedial conjunctival orbitotomy. This case report followed the ethical principles specified in the Declaration of Helsinki as amended in 2013.
CASE PRESENTATIONA 43-year-old Asian man presented with an orbital mass incidentally found on orbital computed tomography for a 6-month gradual decrease in vision oculus dexter (OD). His visual acuity was 20/50 OD and 20/20 OS, and he denied any relevant medical or ocular history. Examination of the right eye revealed a visual field defect with a 22% visual field index and 2 mm of relative exophthalmos OD. A trace right afferent pupillary defect was observed. Orbital magnetic resonance imaging demonstrated a 2.0 × 1.5 × 1.7-cm T2 high, T1 low-signal intensity enhancing mass without diffusion restriction at the orbital apex. The lesion adjacent to the deep posterior aspects of the medial wall and the greater pterygopalatine canal displaced the optic nerve superiorly, rendering the surrounding structures indistinguishable. Based on the size and location of the lesion, the patient was considered a good candidate for endonasal endoscopic removal of the mass. Standard endonasal endoscopic ethmoidectomy was performed using a 4.0-mm, 30-degree endoscope (Olympus, Tokyo, Japan). The lamina papyracea was dissected to the orbital apex as far as necessary and removed from the periorbita using Seeker and ethmoidal forceps at the level of the OCVM border adjacent to the medial wall. A longitudinal periorbital incision parallel to the medial rectus muscle was made at the orbital apex, and careful dissection was performed in the medial intraconal region lateral to the medial rectus. Since the OCVM was firmly attached to the surrounding structures, we made a second inferomedial conjunctival incision. Orbitotomy through the conjunctiva was performed towards the intraconal OCVM using a thin malleable brain retractor, neuropathies, and a Gorney suction elevator to better visualize and minimize bleeding. A red-to-purple elastic-soft mass, tightly adhering to the surrounding tissue, was revealed and dissected carefully towards the medial wall in an atraumatic manner. Finally, we removed the lesion using ethmoidal forceps through the endonasal space (Fig. 1). The medial wall was not reconstructed, and only biodegradable packing was applied in the ethmoidal cavity to cover and support the entire medial aspect of the orbital wall. Histopathological evaluation was compatible with cavernous hemangioma. There was an instant improvement in the visual acuity of 20/20 visual field index to 94% after surgery. There was no relative afferent pupillary defect, diplopia, or extraocular movement limitation. At the 12-month follow-up, he had no sequelae but 1 mm of enophthalmos (Fig. 2).
 FIGURE 1:
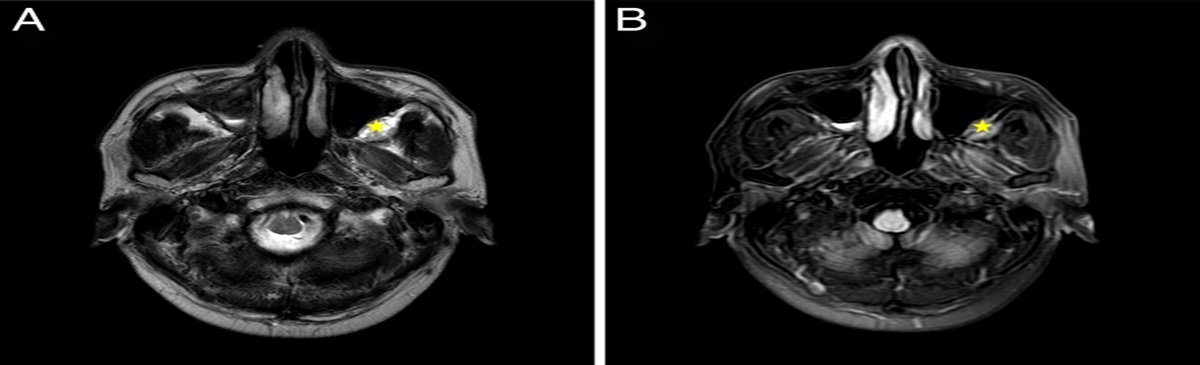
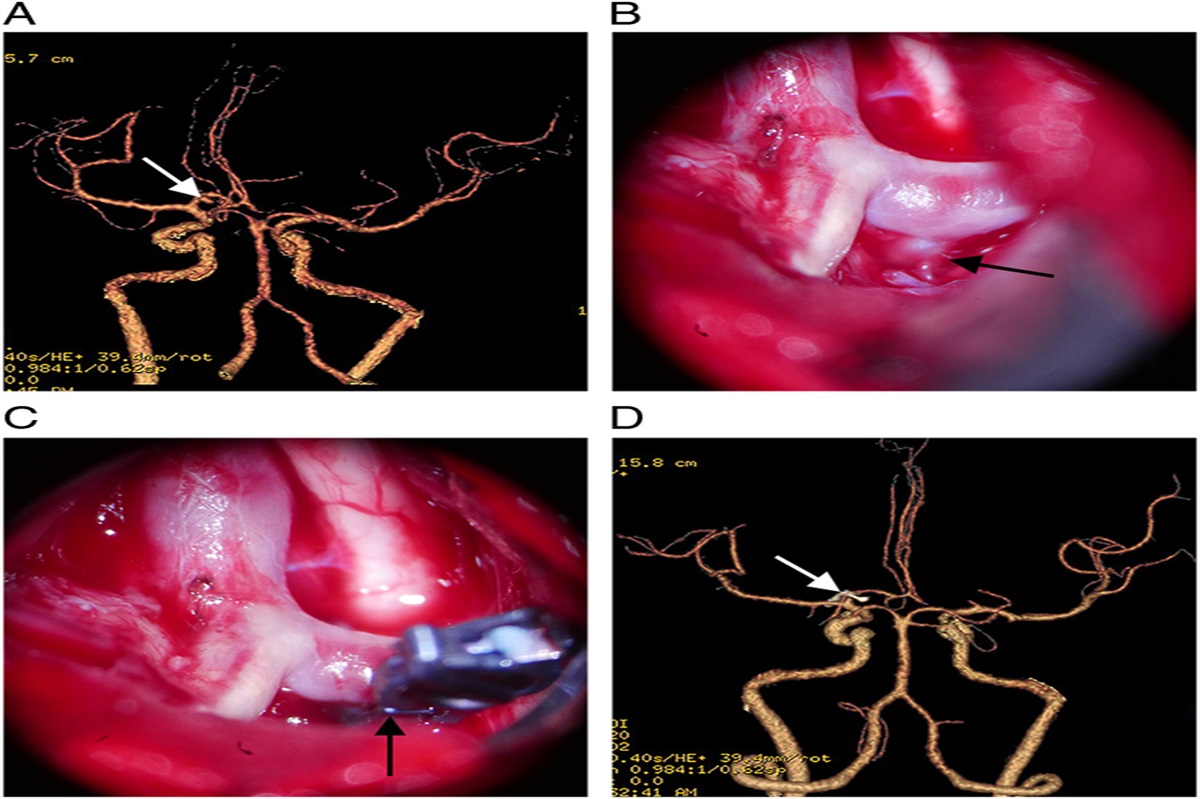
FIGURE 1: Axial (A) and coronal (B) magnetic resonance imaging of T1 weighted hypointense orbital cavernous vascular malformation. The optic nerve is displaced superiorly by the lesion (yellow asterisk). Sagittal (C) computed tomography scan demonstrating that the apical lesion adheres to the palatine bone and the greater palatine canal (red arrow). Magnetic resonance imaging showed a 2.0 × 1.5 × 1.7-mm-sized heterogeneous hyperintense signal on T2 and low-signal intensity on T1 (not shown in this picture) without diffusion-restricted orbital mass at the orbital apex (D–F). The diffusion-weighted apparent diffusion coefficient was 1.24±0.13 (mean±SD). G, Orbital tumor visualized endoscopically after mobilizing it inferiorly and medially via orbital approach. H, After complete dissection, the tumor was removed transnasally using forceps. I, The histopathological finding was compatible to cavernous venous malformation and its horizontal size was ~21 mm.
 FIGURE 2:
FIGURE 2: Axial (A) and coronal (B) magnetic resonance imaging after surgery showed complete removal of orbital cavernous venous malformation of the orbital apex with mild postoperative inflammation. Packing material is filled in the ethmoidal cavity and the contour of the medial wall is well preserved. Axial (C) and coronal (D) computed tomography scans 12 months after surgery showed no recurrence of orbital cavernous venous malformation. E and F, Postoperatively, no complications were observed, only mild enophthalmos OD. OD indicates oculus dexter.
DISCUSSIONSeveral techniques have been tried.4 Despite advancements in surgical procedures, the management of OCVMs near the orbital apex remains challenging because of the increased risk of collateral injury.5 Techniques for orbital apex lesions include transcranial and transcaruncular approaches, often combined with medial rectus muscle detachment, lateral orbitotomy, or infracture of the ethmoidal sinuses to provide additional room for surgical manipulation.6 Alternative therapeutic methods have also been documented, such as multisession gamma knife radiosurgery.7
The use of an endoscopic approach to the orbital apex has grown in popularity in recent years, since 1999 when Lot et al8 first described an endonasal endoscopic approach to remove an orbital hemangioma. Lenzi et al9 reported the purely endoscopic endonasal management of orbital intraconal hemangiomas. However, a significant drawback is the lack of binocular vision, which is important for orbital apex tumor removal. Wu et al,5 conversely, presented an endoscopic transethmoidal method with an additional transcaruncular approach. They found that significant adherence at the apex was a critical issue and that larger hemangiomas with apical extension that had been present for an extended period may be firmly adherent at the apex, necessitating additional manipulation, such as a transcaruncular approach, to dissect the lesion while avoiding collateral damage. In our case, the OCVM was located lateral to the medial rectus and firmly adhered to the palatine bone and surrounding structures. It was not possible to fully visualize or safely dissect from the apex using only the endoscopic approach; however, we were able to dissect the OCVM with additional inferomedial conjunctival orbitotomy. A previous decompression effect using an endoscopic approach permitted a safer approach to the lesion, even near the optic canal. We gently mobilized the tumor into the nasal cavity using diluted epinephrine (<100,000)-soaked neuropathies and a suction elevator while minimizing bleeding. Bleeding and visibility are other issues when managing OCVMs, especially in the orbital apex.10 We discovered that bleeding could be controlled from the posterior feeders to the OCVM in epinephrine-soaked neuropathies. However, when using epinephrine at the apex, it is essential to use care and inform patients about the risk of ischemic complications.
Decompression of the apex through the endoscopic approach before the external approach may reduce the pressure on the orbital apex, including the optic nerve, and may make it possible to manipulate to facilitate dissection of the OCVM safely and effectively in our patient, who had optic neuropathy. Instead of pulling out the OCVM with incomplete dissection of the posterior region, it was technically simpler to mobilize the OCVM inferiorly and medially using neuropathies and a suction elevator. This results in complete dissection with minimal damage to other critical structures. After thorough removal of the OCVM through the nasal cavity, we filled the ethmoidal cavity with an 8-mm-sized biodegradable packing material, which allowed the recovery of the medial wall contour.
To summarize, we recognized that using an endonasal endoscopic approach alone to remove a relatively large OCVM from the orbital apex may be somewhat insufficient; however, combining an endonasal endoscopic approach with a transconjunctival and caruncular orbitotomy appears to be a promising technique for removing OCVM from the intraconal apex. The proper use of surgical equipment and cautious maneuvering will enable adequate removal of the compressive lesion.
REFERENCES 1. Rootman DB, Heran MK, Rootman J, et al. Cavernous venous malformations of the orbit (so-called cavernous haemangioma): a comprehensive evaluation of their clinical, imaging and histologic nature. Br J Ophthlmol 2014;98:880–888 2. Cheung SSL, Lam SC, Yuen HKL. Transnasal endoscopic sclerotherapy for orbital apex lymphatic malformation. Ophthalmic Plast Reconstr Surg 2021;37(3S):S154–S156 3. Miyake MM, Bleier BS Chiu AG, Palmer JN, Adappa ND. Chapter 20—endoscopic approach and removal of orbital tumors. Atlas of Endoscopic Sinus and Skull Base Surgery (Second Edition). Philadelphia, PA: Elsevier; 2019:165–170.e161 4. Harris GJ. Cavernous hemangioma of the orbital apex: pathogenetic considerations in surgical management. Am J Ophthalmol 2010;150:764–773 5. Wu W, Selva D, Jiang F, et al. Endoscopic transethmoidal approach with or without medial rectus detachment for orbital apical cavernous hemangiomas. Am J Ophthalmol 2013;156:593–599 6. Cho KJ, Paik J-S, Yang S-W. Surgical outcomes of transconjunctival anterior orbitotomy for intraconal orbital cavernous hemangioma. Korean J Ophthalmol 2010;24:274–278 7. Young SM, Kim KH, Kim Y-D, et al. Orbital apex venous cavernous malformation with optic neuropathy: treatment with multisession gamma knife radiosurgery. Br J Ophthlmol 2019;103:1453–1459 8. Lot G, Portier F, Herman P, et al. Transnasal endoscopic removal of an orbital cavernoma. Ann Otol Rhinol Laryngol 1999;108:147–150 9. Lenzi R, Bleier BS, Felisati G, et al. Purely endoscopic trans-nasal management of orbital intraconal cavernous haemangiomas: a systematic review of the literature. Eur Arch Otorhinolaryngol 2016;273:2319–2322 10. Cohen LM, Grob SR, Krantz KB, et al. Combined endonasal and orbital approach for resection of orbital apical tumors. Ophthalmic Plast Reconstr Surg 2022;38:393–400
留言 (0)