
記住我

Video
Tao, Zhang MD1; Wang, Haixia MD1; Du, Zhonghan MD1; Zhang, Yan MD1
Author Information1Department of Gastroenterology, Nanchong Central Hospital, The Second Clinical Medical College, North Sichuan Medical College, Nanchong, China.
Correspondence: Zhang Tao, MD. E-mail: [email protected].
SUPPLEMENTARY MATERIAL accompanies this paper at https://links.lww.com/AJG/C498
This is an open access article distributed under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
The American Journal of Gastroenterology: doi: 10.14309/ajg.0000000000001772 Metrics
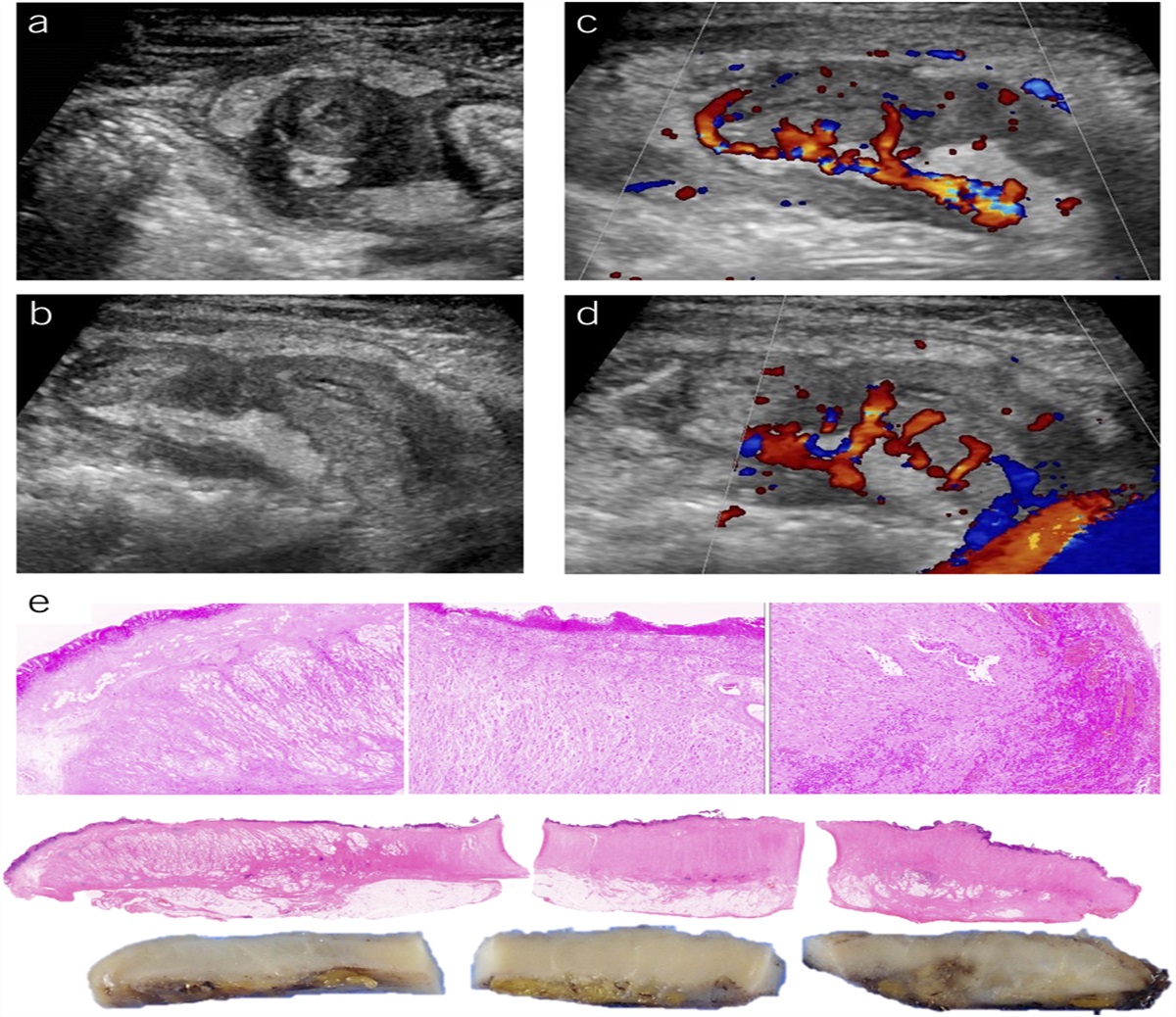
A 75-year-old man presented to our department with a complaint of rectal bleeding for 2 weeks of hematochezia occurring 2–3 times per day. He had normal vital signs, a 10-year history of cirrhosis, a Child–Pugh grade of B, moderate ascites, and esophageal varices. Blood analysis revealed low white blood cell (2.77 × 109/L) and platelet (49 × 109/L) counts, low hemoglobin (8.3 g/dL) and albumin (3.8 g/dL), and normal prothrombin time. We observed anorectal varices with many traffic branches, and crevasses of hemorrhoids were observed under colonoscope (a,b). The apparent return of blood in the transparent needle verified needle puncturing into the venous plexus (c). Polidocanol with methylene blue was injected into the anorectal varices, and the traffic branches of the anorectal varices were filled with flowing bubbles and blue polidocanol (d). Twenty minutes later, anorectal varices with traffic branches had disappeared at the rectum (e). The patient did not report rectal bleeding after sclerotherapy. A few bleached scars were observed at the smooth rectum 1 week later (f). For patients with bleeding varices, besides sclerotherapy, ligation and transjugular intrahepatic portosystemic shunt are the alternative treatment options. Sclerotherapy, not ligation, should be preferred for varices with multiple traffic branches because polidocanol can be dispersed into the whole variceal plexus. However, variceal ligation was challenging due to difficulty in fully ligating traffic branches of varices. In addition, transjugular intrahepatic portosystemic shunt may also be a good choice for variceal bleeding with many traffic branches. Watch the video at https://links.lww.com/AJG/C498. (Informed consent was obtained from the patient to publish these images.)
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology
留言 (0)