
記住我

Infliximab (IFX) is a monoclonal IgG1 anti-tumor necrosis factor (TNF) antibody discovered in 1989 (1) whose use since the early 2000s has profoundly improved the management of inflammatory diseases and in particular Crohn's disease (CD). IFX and other more recent antibodies targeting TNF have proven to be effective in active CD for both induction and maintenance treatment (2–4). More than 60% of anti-TNF-naive CD patients respond to IFX at 1 year. However, a significant number of patients secondarily withdraw their treatment for various reasons. The first is linked to a progressive loss of response (LOR) requiring optimization of IFX treatment with an increase in the dose and/or the frequency of infusions (5). This often effective strategy may prove to be useless, particularly in the case of the appearance of anti-drug antibodies neutralizing IFX. This immunization against IFX does not in itself explain all the secondary LORs; however, it can be limited by the concomitant use of an immunosuppressant at least at the beginning of IFX treatment (6,7). Another common reason for stopping IFX during maintenance therapy is the occurrence of a side effect, including an infusion reaction, the pathophysiological mechanisms of which are varied but mostly simple intolerance (8). In this case, the strategy is to slow down the infusion or to propose premedication or even a tolerance induction protocol (9). Secondary LOR and intolerance are responsible for discontinuation of IFX. Although the therapeutic arsenal of CD has increased considerably in 5 years with the availability of monoclonal antibodies targeting IL12/23 (ustekinumab) (10) or leukocyte trafficking (vedolizumab) (11), the response rates of these new drugs are not higher than those obtained with IFX, especially because the effectiveness of the biologics decreases with the number of treatment lines previously used (12,13). We therefore observe in clinical practice some patients who, despite the increased number of available drugs, have not responded or have become refractory to all molecules. In the literature, the data regarding the possibility of restarting IFX in this situation come only from retrospective studies (14,15). The aim of the REGAIN study was to prospectively assess the efficacy, safety, and tolerability of retreatment with IFX after stopping for intolerance or LOR.
METHODS Study designREGAIN was a prospective observational cohort study conducted in 16 French academic centers from the Groupe d'Etudes Thérapeutiques des Affections Inflammatoires Digestives (GETAID). Investigators from the GETAID designed the study and collected and analyzed the data. The study was approved by the local institutional review board of each participating center and by the French Health Authority and was registered under EudraCT number 2012-001061-33. Written informed consent was obtained from all participants.
To be included, patients had to be of the age of at least 18 years and meet the following inclusion criteria: (i) a diagnosis of luminal CD based on clinical, biological, endoscopic, and histological signs of the disease, according to the Lennard-Jones criteria; (ii) an active disease confirmed by a CD Activity Index (CDAI) of > 150 with at least 1 objective sign of active inflammation (C-reactive protein (CRP) >5 mg/L and/or fecal calprotectin >250 μg/g and/or radiological and/or endoscopic signs of activity); and (iii) a need to reintroduce IFX therapy after at least 6 months of discontinuation. The reasons for the initial discontinuation of IFX was loss of efficacy after an initial response in a patient treated for at least 6 months (secondary LOR) or intolerance to IFX, regardless of the previous duration of treatment. Patients who had previously experienced life-threatening IFX intolerance were excluded. Patients with stoma and exclusive perianal lesions and pregnant women were also ineligible. Digestive infections were ruled out with fecal culture and an enzyme-linked immunosorbent assay (ELISA) for Clostridium difficile toxins. Medical history, disease characteristics, and current medications were recorded at study inclusion.
ProceduresIFX was reintroduced at a dose of 5 mg/kg of body weight and was infused over a 2-hour period at weeks 0, 4, and 8 (induction regimen) and then every 8 weeks (maintenance regimen). During the maintenance regimen, IFX was administrated over 1 hour, with a subsequent clinical monitoring of 1 hour. Dose intensification (up to 10 mg/kg every 4 weeks) of IFX was decided in the case of insufficient response or LOR. Premedication with an infusion of dexchlorpheniramine and hydrocortisone was performed in all patients before each IFX infusion. The concomitant use of immunosuppressants (azathioprine, 6-mercaptopurine, and methotrexate) was left to the discretion of each investigator.
Laboratory tests (C-reactive protein, blood counts, and fecal calprotectin) were performed systematically at baseline and during the follow-up if necessary. Trough level of IFX (TLI) and antibody to IFX (ATI) concentrations were all measured just before IFX infusion at weeks 0 and 4 using 2 assays: the Lisa-Tracker Premium IFX ELISA kit (Theradiag, Marne La Vallée, France), which is a drug-sensitive technique, and drug-tolerant ELISA, which was previously described by Ben-Horin et al. (16), using antihuman lambda chain for the detection of anti-drug antibodies. ATIs were considered positive if ≥ 10 ng/mL with the Lisa-Tracker kit and ≥ 2.5 μg/mL Eq with the drug-tolerant assay.
Outcomes measuresThe primary end point was the efficacy of IFX retreatment at week 26 defined by a CDAI of <150 in the absence of IFX discontinuation or use of corticosteroid therapy, surgery, or other biologics. Prespecified secondary end points were (i) tolerance of IFX retreatment over a 12-month period, (ii) predictive factors of efficacy and tolerance at week 26, and (iii) association of TLI and ATI with efficacy and tolerance of IFX retreatment.
Safety assessment occurred during induction and maintenance phases up to at least 52 weeks after IFX reintroduction as recommended by the French health authorities. Safety end points were adverse events (AEs), serious AEs and AEs related to study treatment, AEs leading to discontinuation, and deaths.
Statistical analysisUnder the hypothesis of an IFX retreatment success rate between 30% and 70%, we calculated that approximately 100 patients would provide a power of 80% to detect a factor associated with success with an odds ratio (OR) of > 4.
Quantitative variables are described by median and interquartile range and compared between groups using the Wilcoxon test. Qualitative variables are described by count and percentage and compared between groups with the χ2 test or Fisher exact test when necessary.
Clinical or biological factors associated with retreatment success or failure at W26 were searched for by comparing the 2 groups in univariate and multivariate analyses, and the strength of the association was expressed using ORs with 95% confidence interval calculated by fitting logistic regression models. A similar analysis was made on the subpopulation who received the total IFX induction treatment (landmark analysis).
Specific analyses were performed for the pharmacokinetics of IFX (TLI and ATI). Their predictive value was assessed by comparing positive rates between success and failure groups, at baseline, and in 2 landmark analyses in the subgroup of patients still receiving IFX at week 4. The evolution of positive ATIs was assessed by comparing the proportion of ATI-positive patients at baseline and week 4 using the McNemar χ2 test.
A P value of < 0.05 was considered significant, and all statistical tests were 2‐sided. All analyses were performed using R software R 3.4.2 (http://www.R-project.org).
RESULTS Patients and study treatmentFrom June 2015 to June 2018, 110 patients from 16 GETAID French centers were screened. Thirteen patients were not included (inclusion criteria not met, withdrawal of consent, etc) and 97 patients were included. Ultimately, 69 patients were analyzed after excluding patients whose initial reason for stopping IFX was pregnancy (n = 10) or personal considerations (n = 18) (Figure 1). The demographic and clinical characteristics of the 69 analyzed CD patients are summarized in Table 1. Almost two-thirds of the patients were women (61%) with a median age of 34 years (27–43) at inclusion. The median duration of disease was 10.1 years (7.6–16.1), and a history of previous intestinal resection was observed in 27 cases (39%). Twenty-seven (40%) and 19 (28%) patients had stricturing and penetrating phenotypes, respectively, and 37 patients (54%) had a history of perianal lesions. All patients had active CD at the time of inclusion with a median CDAI of 259 (197–363), a median CRP of 13.1 mg/L (6.2–31.6), and a median fecal calprotectin of 1,084 μg/g (439–1,800).
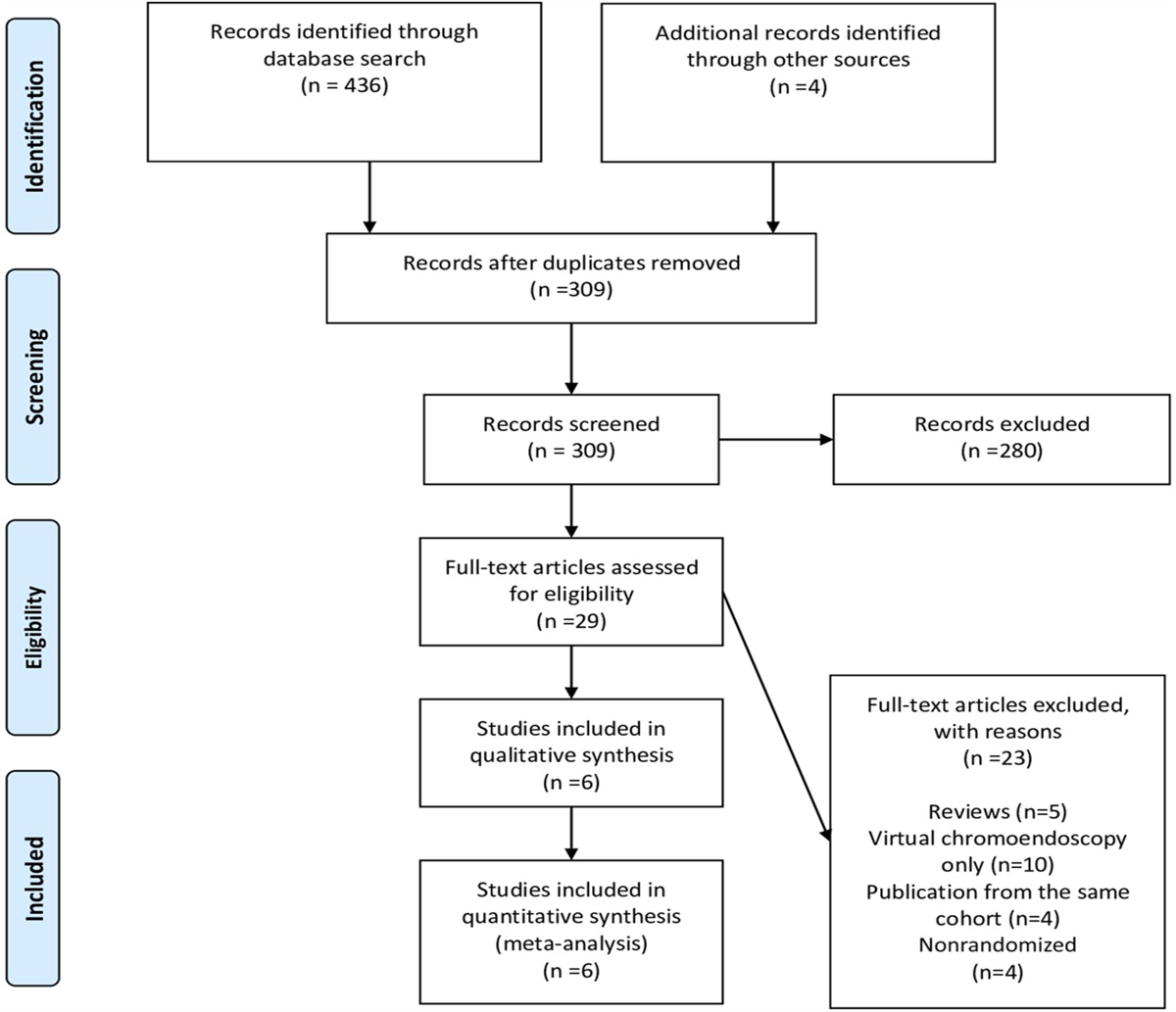
 Figure 1.:
Figure 1.: Flow chart of the study. IFX, infliximab.
 Table 1.:
Table 1.: Baseline characteristics of patients
Median duration between initial IFX discontinuation and inclusion was 43.4 months (21.0–76.2). Reasons for the initial discontinuation of IFX were secondary LOR in 48 patients (70%) and intolerance in 21 patients (30%). During the IFX-free interval, patients were treated with a variety of other agents including investigational drugs and surgery.
Patients with prior LOR and intolerance were comparable for baseline clinical and biological characteristics, except for a median disease duration (median duration 14.1 years in the “intolerance” group vs 8.7 years in the “LOR” group; P = 0.005). A longer duration between IFX discontinuation and inclusion in the “intolerance” group compared with that observed in the “LOR” group (median duration 76.2 months [33.1–101.4] vs 34.5 months [17.2–62.0], respectively; P = 0.007) was also highlighted (see Supplementary Table 1, https://links.lww.com/AJG/C537).
Within the year after inclusion, patients received a median of 6 IFX infusions [2–9]. During the induction regimen (first 3 infusions), only 5 patients required an increase of their IFX posology. However, among patients who received at least 2 infusions during the maintenance regimen (40 patients), 11 patients (28%) required an increased dose of IFX (up to 10 mg/kg body weight) and 20 patients (50%) benefited from an optimization of IFX infusions frequency up to 4 weeks.
Primary end point and factors associated with treatment successAt week 26, 24 patients (35% [95% confidence interval: 24%–48%]) reached the primary end point (CDAI < 150). We analyzed all the clinical and biological baseline characteristics of patients to find predictive factors of IFX retreatment success. We found no difference between rates of clinical remission in patients with initial secondary LOR and those with IFX intolerance (35% and 33%, P = 0.87, respectively) (Figure 2). Neither disease duration nor its phenotype or the clinical and biological activity (CRP and fecal calprotectin) of CD were predictors of IFX success. Only a shorter median duration between initial discontinuation and restart of IFX was significantly associated with the success of IFX reprocessing (31.6 vs 56.1 months, P = 0.024) (Table 2). There was also a tendency for a more severe disease with a higher median CDAI at inclusion in the failure group compared with the success group but without reaching significance (290 points [226–371] vs 243 points [176–296], P = 0.098) (Table 2).
 Figure 2.:
Figure 2.: Proportion of patients who reached the primary end point at week 26 in the overall cohort and according to the reasons of initial infliximab discontinuation (loss of response or intolerance).
 Table 2.:
Table 2.: Characteristics of patients according to success or failure of IFX treatment at week 26
We then performed a landmark analysis of the subpopulation of patients who received at least the IFX induction treatment (i.e., ≥ 3 infusions) to study the relationship between the use of immunosuppressants during the induction regimen and the success of IFX reprocessing. We found no statistically significant association because 42% of the patients in IFX failure at week 26 received combination therapy with immunosuppressants against 35% of the patients in IFX success (P = 0.77). The response to IFX at week 26 was not different depending on the specific use of thiopurines or methotrexate (P = 0.54 and P = 0.48, respectively).
IFX concentrations and antibodies to IFXRegarding pharmacokinetics, we determined TLIs and the presence of s using, as described in the methods section, drug-sensitive and drug-tolerant assays; we therefore compared the predictive value of these 2 techniques. TLIs measured with the Lisa-Tracker Premium IFX ELISA kit at week 4 were not predictive of a response to IFX at week 26 although the median TLI in the failure group is lower than that found in the success group (1.7 μg/mL [0.4–3.8] vs 3.5 μg/mL [0.7–8.0], respectively, P = 0.17) (Figure 3). At baseline, detection of ATIs was not associated with success or failure of IFX treatment at week 26 whatever the assay used. Thus, with the drug-sensitive technique, at baseline, 16 patients had positive ATIs, which represented 36% of the patients in remission at week 26 against 19% of the patients in treatment failure (P = 0.14). The results were comparable with the drug-tolerant assay with 14 patients with positive ATIs at inclusion representing 18% of the patients treated successfully at week 26 vs 24% of the patients who failed to respond to IFX (P = 0.75) (Figure 4a,b).
 Figure 3.:
Figure 3.: Infliximab trough level measured at week 4 according to subsequent infliximab retreatment success or failure at week 26.
 Figure 4.:
Figure 4.: Proportion of patients in remission at week 26 according to pharmacokinetics results. Proportion of patients in remission according to ATIs at baseline measured with (a) a drug-sensitive assay and (b) a drug-tolerant assay. Proportion of patients in remission according to ATIs at week 4 measured with (c) a drug-sensitive assay and (d) a drug-tolerant assay.
We performed a landmark analysis of the subpopulation of patients who received at least IFX treatment up to week 4. Using the drug-sensitive assay, 24 patients had positive ATIs with a statistically significant difference between the proportion of patients with positive ATIs in success vs failure of IFX treatment at week 26 (19% vs 56%, respectively, P = 0.012) (Figure 4c). At week 4, the use of the drug-tolerant technique made it possible to highlight that 50 patients had positive ATIs with statistically significant difference between the mean level of ATIs at week 4 in success vs failure group (2 μg/mL Eq (1.2–5.7) vs 5.55 μg/mL Eq (2.4–16.2), respectively, P = 0.009) and in the proportion of patients with positive ATIs in success vs failure of IFX treatment at week 26 (48% vs 75%, respectively, P = 0.048) (Figure 4d). Thus, the presence of ATIs at week 4 measured by the drug-sensitive method and the drug-tolerant method both was associated with a high risk of IFX reintroduction failure at week 26 (OR = 5.31 [1.49–19.0] and OR = 3.30 [1.05–10.3], respectively). After multivariate analysis, only positive ATIs at week 4 were significantly associated with IFX treatment failure at week 26 (P = 0.03 with the drug-sensitive assay and P = 0.04 with the drug-tolerant method). We did not detect ATI thresholds providing better precision in the prediction of nonresponse to IFX according to the receiver operating characteristic curves (data not shown).
The frequencies of positive ATIs measured with the 2 methods were not different in patients whose initial reason for stopping IFX was either intolerance or LOR, both at baseline (19% vs 28%, P = 0.55 with drug-sensitive assay and 14% vs 26%, P = 0.36 with drug-tolerant assay, respectively) and at week 4 (53% vs 40%, P = 0.4 with drug-sensitive method and 65% vs 67%, P = 1.00 with drug-tolerant method, respectively). Finally, we analyzed the link between the concomitant use of immunosuppressants and the detection of ATIs. In patients who did not have ATIs at the baseline, taking an immunosuppressant did not prevent the occurrence of ATIs at week 4. Similarly, regardless of the presence or not of ATIs at baseline, taking an immunosuppressant did not modify the frequency of ATIs in patients at week 4. Thus, 35% of the patients with ATIs detected by the drug-sensitive assay at week 4 were taking immunosuppressants compared with 39% of the patients without ATIs (P = 0.71). Identical results were found using the drug-tolerant method because the same frequency of patients took immunosuppressants in the group with or without ATIs at week 4 (36% vs 40%, P = 0.76, respectively).
ToleranceAmong the 314 AEs reported in 91 patients during the study period, 56 were serious in 40 patients (38%). Among these AEs, 124 were considered to be related to IFX treatment, and infections represented the most commonly reported AEs (32.3%) (Table 3). Among the 69 patients analyzed, 32 infusion reactions were recorded in 27 patients, leading to withdrawal of IFX treatment in 20 patients. Twenty-seven of the infusion reactions (84%) occurred during the 3 first IFX infusions and, more particularly, 21 (66%) during the second one. No statistical association between the occurrence of infusion reactions and the presence of anti-drug antibodies at inclusion was found, and rates of infusion reactions were not different in patients without ATIs before restarting IFX compared with those in patients who had ATIs at inclusion (0.085 vs 0.083, P = 0.96 with drug-sensitive method and 0.09 vs 0.068, P = 0.54 with drug-tolerant method, respectively). However, the detection of ATI at week 4, regardless of the method used, was associated with a significantly increased risk of further infusion reactions during IFX treatment. Thus, the incidence of infusion reactions during this study is more than 3 times greater in patients with ATIs detected at week 4 with the drug-sensitive assay compared with that of patients without ATIs (0.26 vs 0.08, P = 0.001). Similar results were found using the drug-tolerant method (0.18 vs 0.07, P = 0.04). The concomitant use of immunosuppressants during IFX treatment was not protective against infusion reactions because 39.1% of the patients receiving immunosuppressants vs 34.8% of the patients not receiving immunosuppressants presented 1 or more infusion reactions during the follow-up. One patient was pregnant during the study and interrupted the treatment. No unexpected safety signals were observed.
 Table 3.:
Table 3.: Adverse events related to IFX
DISCUSSIONWe report here for the first time the results of a multicentre prospective study evaluating the efficacy, safety, and tolerability of retreatment with IFX after stopping for intolerance or LOR in adult CD patients. At the time of the increasing use of biologics targeting the Th17 pathway or leukocyte trafficking with anti-integrins (17) and at the dawn of new drugs such as anti-JAK or S1P inhibitors (18), restarting treatment with IFX in CD after intolerance or LOR may seem useless. However, the response and remission rates of these different new treatments are generally not better than those obtained with anti-TNFs, and it is not uncommon to observe patients resistant to 2 or even 3 different therapeutic mechanisms of action. Furthermore, the inclusion in a clinical trial of these patients refractory to several lines of treatment is not always feasible, and a surgical solution is often not possible or desirable. Therefore, studying the safety and efficacy of IFX retreatment remains a topical issue.
For efficacy, restarting IFX treatment in our study made it possible to obtain remission without steroids at week 26 in 35% of the patients. It is difficult to compare our results with other studies because it is the first with a prospective design. However, our results seem comparable with those obtained by Gagnière et al. (14) in a retrospective study, which found 42% early clinical remission (4–8 weeks) after IFX reintroduction in 61 patients with CD who successively failed IFX and adalimumab. Similarly, clinical remission was obtained in 13 of the 29 patients (45%) 6 months after reintroduction of IFX in another retrospective study including patients successively treated with IFX and then adalimumab before restarting IFX (19). Finally, in the largest retrospective series published to date, Baert et al. (15) found a short-term and 1-year success in 88% and 73% of patients with CD, respectively. Beyond the biases inherent in the retrospective design which probably favor the results of IFX retreatment, the major difference with our study is the initial reason for stopping IFX. Indeed, in our work, all the patients initially stopped IFX for intolerance (30%) or LOR (70%), whereas in the study by Baert et al., nearly 80% of the patients stopped treatment while they were in response to IFX at the time of the initial discontinuation (remission or pregnancy). In practice, a prospective study from the GETAID had already shown that restarting IFX in patients who had stopped IFX after a corticosteroid-free remission for at least 6 months was effective and well tolerated in 88% of the patients who experienced a relapse (20). However, in the Belgian experience, the results of IFX reintroduction in the subgroup of patients (n = 28) who initially stopped IFX for LOR or intolerance are close to ours with 45% of response at 1 year (15). Another difference in our work from the data published so far is the IFX infusion regimen during the induction phase. We therefore chose to administer IFX at weeks 0, 4, and 8 based on the results of a retrospective Italian study, which concluded that this regimen had a better efficacy/safety ratio compared with the classic one (weeks 0, 2, and 6) used in the other studies cited above (21). Nevertheless, our study does not make it possible to conclude on the superiority of one induction regimen over the other in the absence of a direct comparison.
When a decision to resume IFX treatment is considered, safety concerns are at the forefront for gastroenterologists. Once again, the prospective design of our study and the exhaustive collection of AEs provide reliable and reassuring safety data for physicians and patients. Our study highlights the occurrence of AEs in many patients with the need to stop treatment in 32% of them. However, less than half of these AEs were related to IFX, and the frequency of serious AEs related to the treatment are low (6%). Among the AEs that can occur during IFX reintroduction, infusion reactions are particularly feared. In our study, 27 patients (39%) experienced infusion reactions, and of these, 20 patients (29%) had to discontinue IFX. Notably, treatment intolerance is a major cause of discontinuation of IFX whose frequency is comparable with that of the treatment success rate (29% vs 35%, respectively). However, these results are comparable with those observed in the published study by Gagnière et al. but almost twice as frequent as in the study by Baert et al., which found only 19.5% of the infusion reactions. This difference cannot be explained by the absence of premedication in our study, which was systematic before each IFX infusion and whose usefulness remains controversial in the literature (22). Indeed, the use of premedication with antihistamines has been shown to increase infusion reactions (23), whereas corticosteroids are believed to decrease the specific ATI formation that may reduce infusion reactions (24). The low use of immunosuppressants in our study (33% of patients) may be an explanation given that the combotherapy with immunosuppressants has been shown not only to improve the efficacy but also to reduce the risk of immunogenicity against IFX (25,26). Thus, in the literature, patients with inflammatory bowel disease treated with IFX who develop ATI have a 2-fold risk of infusion reactions and a 6-fold risk of serious infusion reactions (22). Similarly, in our study, detection of ATI at week 4 was associated with a 3-fold higher risk of infusion reactions. Unfortunately, we found no association between the concomitant use of immunosuppressants or the detection of ATI at baseline (with the 2 assays) and the occurrence of an infusion reaction.
Finding predictive factors for the success of IFX retreatment was also a major objective of our study to better select the patients who could benefit from this strategy. Unfortunately, at baseline, no clinical or biological factors (including ATI) were predictive of response to IFX except a shorter duration between initial discontinuation and IFX restart. In particular, the reason for the initial discontinuation of IFX was not associated with a different efficacy of IFX retreatment. Here again, a combination therapy with immunosuppressants was not associated with a better therapeutic response. It should also be noted that the lack of data regarding TLIs and ATIs at the time of initial IFX discontinuation is a limitation of our study. At week 4, although TLIs are not associated with response, the presence of ATIs detected by either a drug-sensitive or drug-tolerant method is strongly associated with remission at week 26. This association between the efficacy of IFX and the absence of ATI is in line with the data in the literature (15). Because the use of immunosuppressants is known to be able to prevent or even suppress ATIs (27), their systematic prescription in this context may legitimately arise, although in our study, the use of immunosuppressants had no significant impact on the occurrence of ATIs. Once again, the low use of immunosuppressants in our study (33% of patients) may be an explanation for the lack of impact of these treatments on ATIs, but this study was not specifically dedicated to the analysis of this parameter and probably lacks power. Recent data describing the association between the HLA-DQA1*05 carriage and the occurrence of ATIs against IFX could perhaps allow us to better select the patients in whom a combination therapy would be essential (28). Another interest of our study was the comparison of the predictive value of IFX response and tolerance of 2 assays for ATI detection. The drug-tolerant method has not shown better performance than the drug-sensitive method, and the availability of the latter makes it highly recommendable in clinical practice.
Although our study has limitations and, in particular, the relatively short follow-up period and the absence of objective criteria to evaluate remission (i.e., endoscopy), it confirms on the one hand the effectiveness of IFX retreatment in therapeutic stalemate situations with reasonable safety and on the other hand the interest of early ATI measurement to predict response and tolerance. When a resumption of IFX is considered, a combination with an immunosuppressant and systematic detection of ATI at week 4 can be proposed, which should prompt consideration of another treatment in the event of positivity.
CONFLICTS OF INTERESTGuarantor of the article: Gilles Boschetti, MD, PhD.
Specific author contributions: G.B.: acquisition of data, statistical analysis, and drafting of the manuscript. M.N., D.L., X.R., C.G., A.A., A.B., C.Z., X.H., A.B., J.-C.G., Y.B., M.A., R.A., S.V., L.V., and F.C.: acquisition of data, inclusion of patients, and critical revision of the manuscript. S.P.: biological analysis and interpretation of data and critical revision of the manuscript. K.D. and J.L.: statistical analysis and critical revision of the manuscript. L.P.B.: study concept and design, drafting of the manuscript, and study supervision.
Financial support: Grant from the Association François Aupetit (AFA). Theradiag for the drug and anti-drug antibody tests.
Potential competing interests: G.B. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Celltrion, Takeda, Amgen, and Sandoz. D.L. declares counseling, boards, or transports fees from AbbVie, Biogaran, Biogen, Celltrion, Ferring, Fresenius-Kabi, Janssen, MSD, Novartis, Pfizer, Roche, Sandoz, Takeda, Theradiag, and Tillotts-Pharma. X.R. served as a speaker and advisory board member for AbbVie, MSD, Pfizer, Amgen, Takeda, Gilead, Janssen, and Theradiag. C.G. declares boards, speaker, or transports fees from AbbVie, Celltrion, Janssen, MSD, Pfizer, Takeda, and Vifor. A.A. served as a speaker and advisory board member for AbbVie, MSD, Pfizer, Amgen, Takeda, Gilead, and Janssen. A.B. declares counseling, boards, or transports fees from AbbVie, Amgen, Biogen, Celltrion, Ferring, Fresenius-Kabi, Janssen, Medtronic, MSD, OSE Immunotherapeutics, Pfizer, Roche, Takeda, Theradiag, and Tillotts-Pharma. C.Z. received board membership, consultancy, or lecture fees from AbbVie, Janssen, Pfizer, and Takeda. X.H. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Celltrion, Takeda, Amgen, and Sandoz. A.B. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Celltrion, Takeda, Amgen, and Sandoz. J.-C.G. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Celltrion, Takeda, Amgen, and Sandoz. Y.B. received grant supports from Innate Pharma, Janssen, Takeda, and Genentech/Roche and served as a speaker or an advisory board member for AbbVie, Amgen, Biogen, Boehringer-Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Ferring, Genentech, Gilead, IQVIA, Janssen, Novartis, Pfizer, Roche, Takeda, and Tillotts. M.A. received grant supports from Innate Pharma, Janssen, Takeda, and Genentech/Roche and served as a speaker or an advisory board member for AbbVie, Amgen, Biogen, Boehringer-Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Ferring, Genentech, Gilead, IQVIA, Janssen, Novartis, Pfizer, Roche, Takeda, and Tillotts. R.A. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Takeda, and Amgen. S.V. served as a speaker and advisory board member for AbbVie, MSD, Pfizer, Amgen, Takeda, Gilead, and Janssen. F.C. served as a speaker and advisory board member for AbbVie, Janssen, Ferring, Norgine, Tillotts, Pfizer, Takeda, and Amgen. M.N. received board membership, consultancy, or lecture fees from AbbVie, Adacyte, Amgen, Arena, Biogen, CTMA, Celltrion, Ferring, Fresenius-Kabi, Janssen, Mayoli-Spindler, MSD, Pfizer, and Takeda. S.P. served as a speaker for Theradiag, MSD, and Pfizer. K.D.: none. J.L.: none. L.P.-B. received grant supports from Innate Pharma, Janssen, Takeda, and Genentech/Roche and served as a speaker or an advisory board member for AbbVie, Amgen, Biogen, Boehringer-Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Ferring, Genentech, Gilead, IQVIA, Janssen, Novartis, Pfizer, Roche, Takeda, and Tillotts.
Study Highlights
WHAT IS KNOWN ✓ Although the therapeutic arsenal in Crohn's disease is expanding, reintroducing an antitumor necrosis factor treatment previously discontinued is still questionable. ✓ Data on infliximab (IFX) retreatment after intolerance or loss of response remain controversial and come from a retrospective study. WHAT IS NEW HERE ✓ Approximately 35% of patients with Crohn's disease achieve clinical remission at week 26 with IFX retreatment when previously discontinued for loss of response or intolerance. ✓ The detection of positive anti-drug antibodies at week 4 was predictive of IFX failure at week 26 and IFX infusion intolerance. ✓ Infusion reaction was the main reason for discontinuing IFX in almost 30% of cases. ✓ The concomitant use of an immunosuppressant did not prevent IFX reintroduction failure, immunization against IFX, or the occurrence of adverse reactions. AcknowledgmentsGETAID clinical operational team (Paris, France). All patients enrolled in the study.
REFERENCES 1. Knight DM, Trinh H, Le J, et al. Construction and initial characterization of a mouse-human chimeric anti-TNF antibody. Mol Immunol 1993;30:1443–53. 2. Targan SR, Hanauer SB, van Deventer SJ, et al. A short- term study of chimeric monoclonal antibody cA2 to tumor ne-crosis factor alpha for Crohn's disease. Crohn's Disease cA2 Study Group. N Engl J Med 1997;337:1029–35. 3. Hanauer SB, Feagan BG, Lichtenstein GR, et al., ACCENT I Study Group. Maintenance infliximab for Crohn's disease: The ACCENT I randomised trial. Lancet 2002;359:1541–9. 4. Colombel JF, Sandborn WJ, Rutgeerts P, et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn's disease: The CHARM trial. Gastroenterology 2007;132:52–65. 5. Gisbert JP, Panés J. Loss of response and requirement of infliximab dose intensification in Crohn's disease: A review. Am J Gastroenterol 2009;104:760–7. 6. Vande Casteele N, Khanna R, Levesque BG, et al. The relationship between infliximab concentrations, antibodies to infliximab and disease activity in Crohn's disease. Gut 2015;64:1539–45. 7. Kennedy NA, Heap GA, Green HD, et al., UK Inflammatory Bowel Disease Pharmacogenetics Study Group. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn's disease: A prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol 2019;4:341–53. 8. Lichtenstein L, Ron Y, Kivity S, et al. Infliximab-related infusion reactions: Systematic review. J Crohns Colitis 2015;9:806–15. 9. Pauchard I, Nancey S, Hacard F, et al. Efficacy and safety of infliximab tolerance induction in patients with inflammatory bowel diseases who experienced acute infusion reactions. Dig Dis 2018;36:417–26. 10. Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as induction and maintenance therapy for Crohn's disease. N Engl J Med 2016;375:1946–60. 11. Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for Crohn's disease. N Engl J Med 2013;369:711–21. 12. Gisbert JP, Marín AC, McNicholl AG, et al. Systematic review with meta-analysis: The efficacy of a second anti-TNF in patients with inflammatory bowel disease whose previous anti-TNF treatment has failed. Aliment Pharmacol Ther 2015;41:613–23. 13. Singh S, George J, Boland BS, et al. Primary non-response to tumor necrosis factor antagonists is associated with inferior response to second-line biologics in patients with inflammatory bowel diseases: A systematic review and meta-analysis. J Crohns Colitis 2018;12:635–43. 14. Gagniere C, Beaugerie L, Pariente B, et al. Benefit of infliximab reintroduction after successive failure of infliximab and adalimumab in Crohn's disease. J Crohns Colitis 2015;9:349–55. 15. Baert F, Drobne D, Gils A, et al. Early trough levels and antibodies to infliximab predict safety and success of reinitiation of infliximab therapy. Clin Gastroenterol Hepatol 2014;12:1474–81. 16. Ben-Horin S, Yavzori M, Katz L, et al. The immunogenic part of infliximab is the F(ab')2, but measuring antibodies to the intact infliximab molecule is more clinically useful. Gut 2011;60:41–8. 17. Torres J, Mehandru S, Colombel JF, et al. Crohn's disease. Lancet 2017;389(10080):1741–55. 18. Sabino J, Verstockt B, Vermeire S, et al. New biologics and small molecules in inflammatory bowel disease: An update. Therap Adv Gastroenterol 2019;12:1756284819853208. 19. Brandse JF, Peters CP, Gecse KB, et al., North Holland GUT Club. Effects of infliximab retreatment after consecutive discontinuation of infliximab and adalimumab in refractory Crohn's disease. Inflamm Bowel Dis 2014;20:251–8. 20. Louis E, Mary JY, Vernier-Massouille G, et al. Maintenance of remission among patients with Crohn's disease on antimetabolite therapy after infliximab therapy is stopped. Gastroenterology 2012;142:63–70. 21. Felice C, Pugliese D, Guidi L, et al. Retreatment with infliximab in inflammatory bowel disease: Tolerability and effectiveness of different Re-induction regimens. DDW2014, Abstract 342. 22. Steenholdt C, Svenson M, Bendtzen K, et al. Severe infusion reactions to infliximab: Aetiology, immunogenicity and risk factors in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2011;34:51–8. 23. Cheifetz A, Smedley M, Martin S, et al. The incidence and management of infusion reactions to infliximab: A large center experience. Am J Gastroenterol 2003;98(6):1315–24. 24. Farrell RJ, Alsahli M, Jeen YT, et al. Intravenous hydrocortisone premedication reduces antibodies to infliximab in Crohn's disease: A randomised controlled trial. Gastroenterology 2003;124:917–24. 25. Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn's disease. N Engl J Med 2010;362:1383–95. 26. Lin Z, Bai Y, Zheng P. Meta-analysis: Efficacy and safety of combination therapy of infliximab and immunosuppressives for Crohn's disease. Eur J Gastroenterol Hepatol 2011;23:1100–10. 27. Strik AS, van den Brink GR, Ponsioen C, et al. Suppression of anti-drug antibodies to infliximab or adalimumab with the addition of an immunomodulator in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2017;45(8):1128–34. 28. Sazonovs A, Kennedy NA, Moutsianas L, et al., PANTS Consortium. HLA-DQA1*05 carriage associated with development of anti-drug antibodies to infliximab and adalimumab in patients with Crohn's disease. Gastroenterology 2020;158(1):189–99.
留言 (0)