
記住我
What is known about the topic?
Implementation of evidence into clinical practice requires facilitation to support changes in healthcare processes and outcomes. Facilitation is a multifaceted process that can be met through a variety of roles that include core aspects, such as education and capacity building, communication, collaboration and relationship building and project management. A combination of external (by individuals outside of the healthcare institution) and internal (by individuals within the healthcare institution) facilitation activities enable a successful implementation of evidence into clinical practice.What does this article add?
Facilitation varies by practice context and tailoring the facilitation approach to the contextual attributes and features of the healthcare setting can support sustainable practice improvements. The degree of facilitation including the range of activities that must be performed and the mix of individuals’ knowledge and skills is related to resource access, information needs, leadership engagement, and work structure of the unit/ward or health institution where the evidence implementation occurs. Determining which activities and roles (or which combinations) are required in a particular healthcare setting or situation is key to the effectiveness of facilitation as a strategy for implementation. Background and objectivesJBI defines evidence implementation as a ‘purposeful and enabling set of activities designed to engage key stakeholders with research evidence to inform decision-making and generate sustained improvement in the quality of healthcare delivery’.1 Integral to JBI's approach to evidence implementation are three pillars: context analysis, facilitation of change and evaluation of process and outcomes.1 Implementation researchers agree that a certain degree of facilitation is needed to support changes in clinical practice and improve health outcomes. Facilitation has been described as ‘a technique by which one person makes things easier for others’.2, Facilitation is also viewed as both an individual role and a process that includes project management, communication, relationship building and strong leadership.3,4 Although the role of facilitation is recognized as a critical component of evidence implementation, what constitutes effective facilitation is poorly understood.
JBI (based in Adelaide, Australia) and its collaborating entities from around the globe offer education and training on evidence implementation, known as the Evidence Implementation Training Program (EITP) (formerly known as the Clinical Fellowship Program). The program integrates the technical and practical aspects of evidence implementation, builds capacity in evidence-based healthcare and quality improvement, and provides support to healthcare professionals to become leaders in clinical practice behavior changes.5 In the 6-month program, participants, mainly clinicians, undertake an evidence implementation project to improve quality in their clinical setting. Every participant is assigned a facilitator, performs facilitation activities, and/or engages with other facilitators (other than the assigned facilitator) to initiate changes in clinical practice at their healthcare institution.
This article presents five cases of evidence implementation initiatives undertaken in various clinical contexts and in different geographical areas. The aim is to add to the evidence base on facilitation by describing facilitator roles and the activities performed to promote changes in clinical practice, and determining similarities and differences in cross-case comparisons. Five groups of JBI EITP trainers from the JBI Collaboration (Australia, USA, Kenya, Brazil and Spain) share their experiences of facilitation and provide a multinational perspective on how facilitation was operationalized to promote positive changes in clinical practice and health outcomes. These groups represent trainers who have held the most number of EITPs, and therefore, were experienced trainees in the field of evidence implementation. The selection of cases was purposive, and aimed for maximum variation in terms of geographic region, area of clinical practice (i.e. acute versus non-acute), clinical specialty (e.g. surgical, mental health, maternal health, etc.) and country income classification (i.e. high-income, middle-income and low-income countries). This offered the advantage of allowing comparisons to be made across several cases. Table 1 provides a summary of the cases.
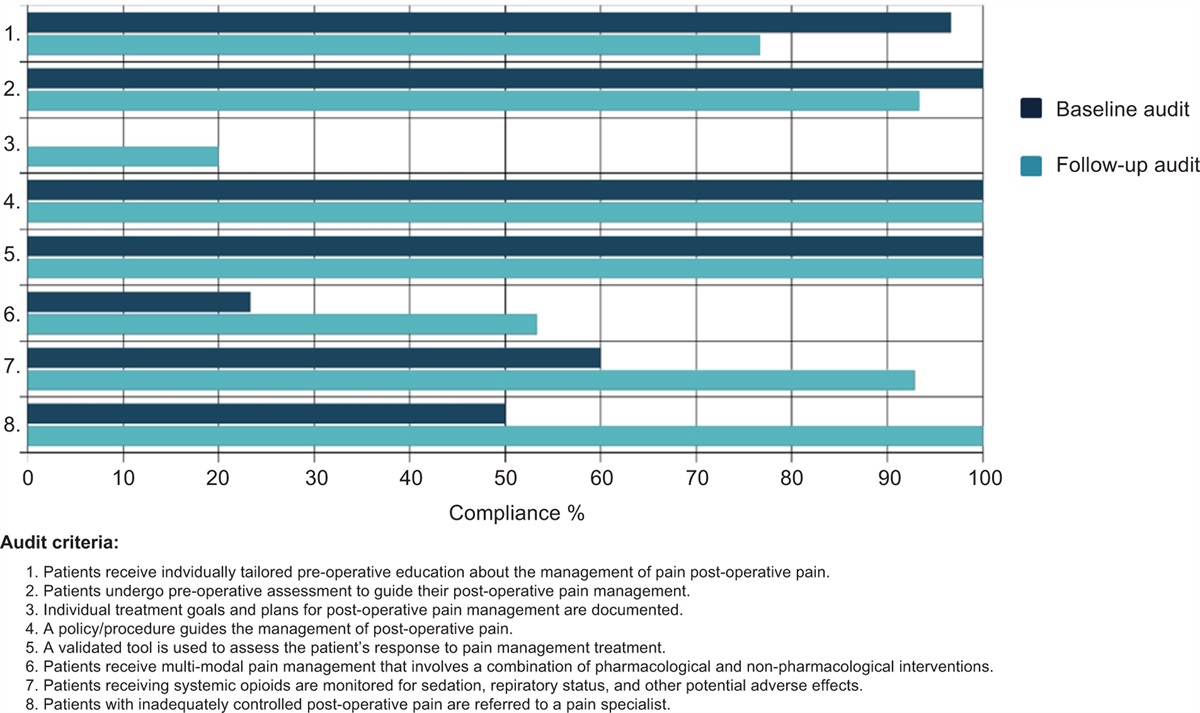
Table 1 - Summary of cases Country/geographic region Income classification Area of clinical practice Clinical specialty Clinical topic Setting Key implementation outcomes Case 1 Australia/Asia Pacific High Acute Mental health Delirium prevention and management Emergency department, a specialty medical unit (constituting specialties including oncology, immunology, infectious diseases and other general medical specialties), haematology and bone marrow transplant, palliative care, heart and lung stream critical care wards, rehabilitation, mental health emergency services and an acute aged care ward in a tertiary hospital in a metropolitan area 12.3% decrease in the rate of hospital-acquired delirium (HAD) at postimplementation (8.1 occasions per 1000 separations at pre-implementation compared with 7.1 postimplementation) Case 2 United States/North America High Nonacute Mental health Workplace violence and aggressive behavior Acute care psychiatric inpatient units within an academic medical center in a metropolitan area 96% of staff in the participating units received relevant education on workplace violence and aggressionStaff de-escalated patients in 83% of the episodes postimplementation9.1% decrease in the rate of violence across all four inpatient behavior health units Case 3 Kenya/Africa Low Nonacute Infection control COVID-19 infection control Health facilities providing maternal and child health services (family planning clinics, antenatal clinics, care during childbirth/labour, postnatal care as well as child immunization clinics) in urban and rural areas 90% of healthcare workers showed competency in donning, use and doffing of personal protective equipmentStructures such as separate areas for triage, assessment and management and a handwashing station were put in place as a result of the project96% compliance to standardized infection prevention and control precautions Case 4 Brazil/South America Middle Acute Vascular Peripherally inserted central catheter (PICC) insertion Emergency department, ICU and other inpatient units in a tertiary hospital 96% of the nursing team across units and wards in the hospital received education on proper PICC insertionGood-to-excellent compliance with best practice recommendations on PICC insertion, maintenance, and removal Case 5 Spain/Europe High Acute Surgical Post-operative pain management Trauma unit of a hospital in an urban area Development and implementation of a validated pain assessment tool for surgical patients, which increased the number of patients who received multimodal pain treatment (including pharmacological and nonpharmacological interventions) from 10% at baseline to 63% at follow-upPatients who continued to experience pain were increasingly referred to pain specialists, which rarely occurred prior to the implementation initiativeIn Australia, delirium has been identified by the Australian Commission on Safety and Quality in Healthcare (ACSQHC) as a high priority area for quality improvement. 7 The ACSQHC released the Delirium Clinical Care Standard to ensure that patients at risk of delirium receive preventative strategies, and those with delirium receive the best possible treatment.6 In 2018, one of the largest tertiary hospitals in New South Wales recorded 299 episodes of hospital-acquired delirium; this delirium rate was higher compared with their peer hospitals. As a result, and in recognition of the Delirium Clinical Care Standard,6 the hospital launched a hospital-wide quality improvement initiative to facilitate the implementation of best practice in delirium care and optimize hospitalized patient outcomes.7
At the commencement of the project, a call for expressions of interest were sought from registered nurses in the hospital who were interested in acting as a change agent for each participating unit or ward. These nurses had to have a strong interest in delirium care and possess leadership skills and undergo the JBI EITP; they were referred to in the project as delirium champions.
Two experienced evidence implementation researchers who were the JBI EITP trainers assisted the delirium champions with the development of local ward or unit project plans, ensured projects progressed as planned and provided feedback and as-needed research support (e.g. access to evidence-based resources, data analysis) to the champions. Monthly meetings between delirium champions and JBI implementation researchers were organized to report project updates and discuss any issues that might impact the project.
Following completion of the JBI EITP, the delirium champions collectively performed a situational analysis via round table discussions and considered the following: resource availability, interdisciplinary relationships, workplace culture, leadership support, communication systems for information exchange, knowledge and skills of healthcare staff, and commitment to quality management. These confirmed the organization's overall readiness for change in terms of delirium practice. To conduct the audit, the delirium champions and the JBI implementation researchers collaborated to determine sample size and how each criterion was to be measured to determine compliance with best practice recommendations for delirium. The delirium champions allocated members of their project team to conduct baseline and follow-up audit and other data collection strategies. They held sessions with their project teams to identify ward/unit-specific barriers to compliance with the recommended practices on delirium.
The delirium champions then convened to discuss strategies, which could be implemented hospital-wide for a collaborative approach to the development of resources and tools. Given the multifactorial causes of noncompliance to recommended practices, a multicomponent strategy was developed and implemented in the participating units/wards. Specifically, the delirium champions developed and tested a tool that addressed recommended practices for delirium screening, assessment, prevention, and management, collaborating with the hospital's Delirium and Cognitive Impairment Community of Practice. The delirium champions delivered face-to-face information sessions with relevant staff on the use of the delirium tool. Along with their project teams, the delirium champions collated delirium resources for the nursing staff and patients (and their families) and sought funding for the purchase of digital clocks and calendars, which were helpful for improving the orientation of patients. They also engaged with the patient flow manager so that patients who are at high risk for delirium can be identified and ‘flagged’ to nurse managers who oversee bed allocations and patient flow. Overall, the delirium champions acted as an ongoing resource person for the quality improvement activity and provided education about delirium as well as peer support.
In this instance, the delirium champions were the main drivers for the quality improvement initiative, with the JBI researchers (EITP trainers) acting as technical support and facilitating the implementation process.
Case study 2: reducing violence and aggressive behavior in an acute care psychiatric inpatient unit in Southeastern United StatesPatient violence against healthcare workers is a global concern, particularly in the mental health care setting.8, 11 In 2008, the American Psychiatric Nurses Association published a series of recommendations to address workplace violence, particularly violence targeting mental health nurses.9 The cause of this violence is often aggression. Aggression is defined as angry feelings or behaviors, such as yelling, screaming, swearing, name-calling, and bullying, which if not addressed often escalate to physical violence within the behavioral health unit.7 Violence reduction strategies in the behavioral health unit consist of both primary and secondary prevention strategies.10 Primary prevention strategies aim to stop violence before it occurs. Secondary prevention involves actions that assess for and reduce the impact and harm resulting from physical violence.
An academic teaching hospital in the Southeastern United States, in partnership with a nursing school within an academic medical center, conducted a project to assess compliance with evidence-based criteria regarding challenging behavior in the acute care psychiatric inpatient unit, specifically aggressive or violent behaviors toward staff. The project objectives were to engage a multidisciplinary team to determine compliance with evidence-based criteria for reducing aggressive and violent behavior, conduct a survey of crisis perceptions by staff, improve knowledge of best practices in the management of aggressive and violent behavior, and improve outcomes regarding the management of aggressive and violent psychiatric patients.11
There were several individuals within the hospital that engaged in different facilitative types of roles. The Chief Nursing Officer (CNO) served as a facilitative leader who identified the problem of increasing aggression and violence on the behavioral health unit, prioritized the problem with an alignment to managerial support, and provided funding for completion of the project. The behavioral unit manager functioned as a process facilitator who provided staff support to participate in the project, secured the unit videos for observation of aggressive and violent behaviors and the mock aggression code sessions. Additionally, the nursing education department staff functioned as internal process facilitators who administered the surveys and provided the Crisis Prevention Education/Training (CPE). The staff nurses functioned as operational facilitators by coordinating thirteen (13) mock aggression/violence codes, tracked mock code nursing staff and police attendance, participated in the codes, reviewed mock code videos for appropriate prevention interventions, and collected data on the dates, times, frequency, locale and code attendance.
JBI EITP trainees from the academic nursing school served as clinical expert facilitators. They were doctoral-prepared nursing faculty with expertise in psychiatric nursing, nurse anesthesia, and quality improvement intervention development. These facilitators who were external to the hospital conceptualized the project with the CNO, wrote the project proposal for approvals, designed the intervention implementation process, planned the mock codes, conducted data analysis, and composed the final project report. The lead EITP trainer, who was an implementation methods expert, helped the EITP trainees and staff nurses analyze and write up the project findings for dissemination.
The project highlighted that a decrease in violence rate and improvements in the use of de-escalation can be sustained through on-going yearly education, quarterly aggression and violence mock codes, and the conducting of future audits.
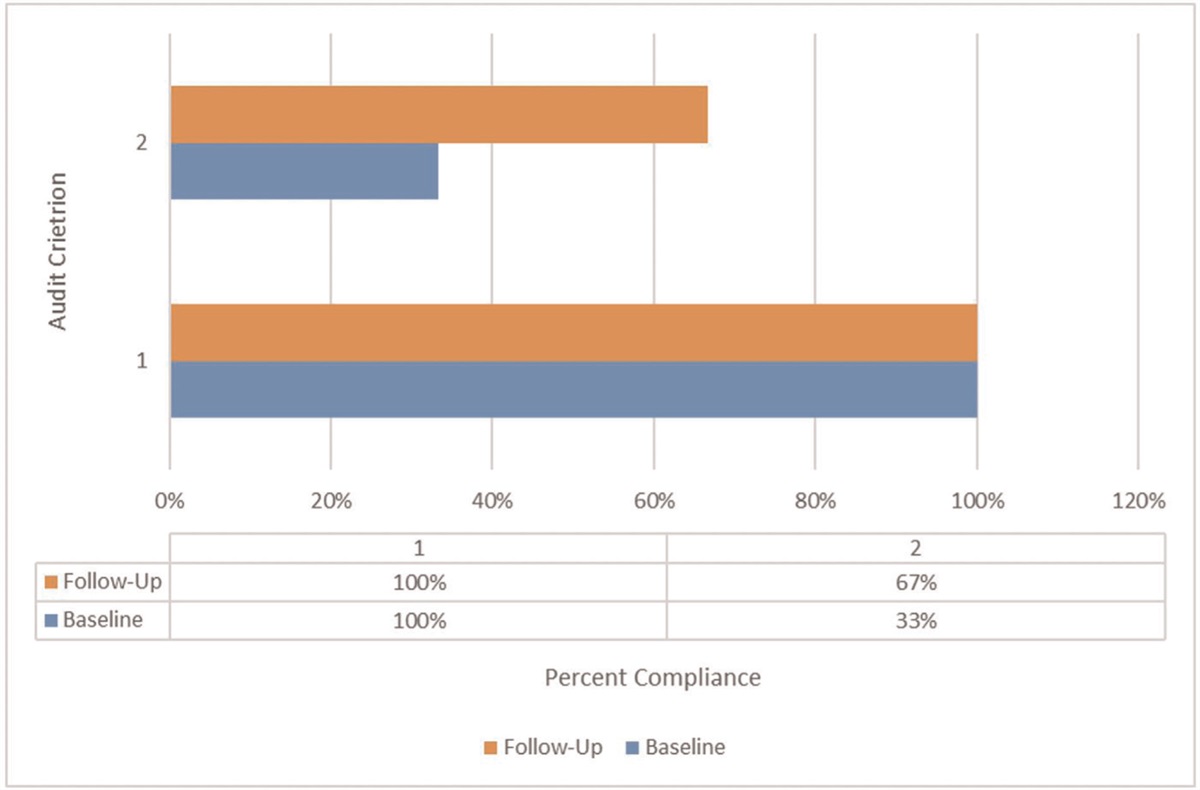
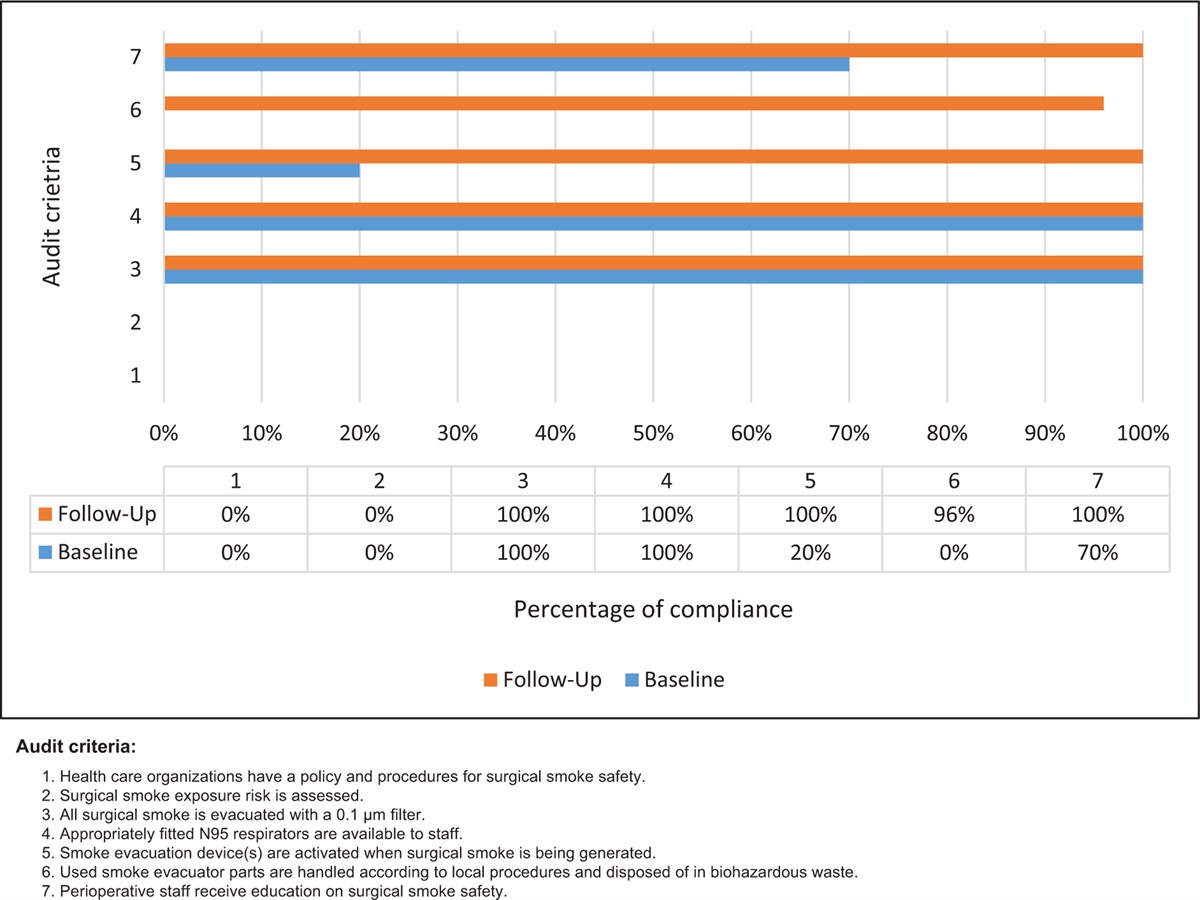
Case study 3: improving coronavirus disease 2019 infection control and prevention practices across different levels of healthcare facilities offering reproductive, maternal, and child health services in KenyaKenya has seen a steady fall in maternal and neonatal mortality as well as increased uptake of childhood immunization and family planning services attributable to provision of well tolerated and timely reproductive, maternal and child health (RMCH) services across different levels of health service delivery. 12,13 Unfortunately, in the wake of the COVID-19 pandemic, government-imposed curfews, the public's fear of contracting COVID-19 and stigma towards the disease have seen a reduction in utilization of these services. To prevent any loss of gains in RMCH, the Ministry of Health in Kenya issued a policy statement during the pandemic to ensure that these services are provided in a well tolerated manner so as to protect both health service seekers and healthcare providers. One way of doing this is to empower healthcare providers in this sector with skills in evidence implementation so that they can implement evidence-based infection prevention and control (IPC) recommendations for COVID-19. With support from an Australian charitable organization and JBI Adelaide, Afya Research Africa trained nine RMCH healthcare providers from different levels of health service provision (i.e. primary care, secondary care and tertiary care facilities) in evidence implementation using JBI's EITP. The project involved assessing and improving compliance to COVID-19 IPC measures in selected RMCH units.12
Four JBI EITP trainers from Afya Research Africa acted as facilitators. Two facilitators were content experts (both are consultant obstetricians/gynaecologists) whereas the other two were experienced implementation methods experts (doctors who have conducted numerous clinical audits in a variety of topics). These facilitators work in the participating health organizations, and therefore, had a good understanding of the local context. Their roles included delivering the EITP to participants and assisting in the development of individual project plans. This involved helping participants with the contextualization of evidence-based audit criteria as well as determination of appropriate measures of compliance to the criteria. They also provided project supervision and support, which involved ensuring adherence to set timelines, help with access to required resources such as audit software (i.e. JBI PACES software), relevant evidence (clinical guidelines, policy documents, etc.), as well as help with data analysis and presentation. Finally, their role involved setting up monthly meetings with participants in which project updates were highlighted. Key attributes and contribution of these facilitators include providing positive reinforcement, content and methods expertise and good communication skills.
In addition, there was a process of facilitation carried out by individual project participants (a mix of doctors, nurses and clinical officers) in each of the nine project sites. Each participant led an audit team that was involved in assessing and improving compliance to COVID-19 IPC practices in their RMCH units. This process enabled participants to develop communication, interpersonal and leadership skills, as well as encouraging stakeholder engagement and involvement so that the aims of the project could be achieved. Specifically, participants had to acquire buy-in for the project from hospital administrators (bottom-up approach) and staff members in their units. They led the process of measuring compliance to evidence-based IPC recommendations, identifying barriers to compliance and developing ways of overcoming such barriers. The participants also had to provide on-going educational support to the staff in their units for sustained compliance to recommendations. Wherever possible, strategies and solutions to overcome barriers were shared and adopted by participants as necessary in their local facility.
At the conclusion of the project, there was a modest improvement in COVID-19 IPC measures across the nine included sites providing evidence that empowering RMCH service providers in sub-Saharan Africa (SSA) can lead to well tolerated delivery of services during the pandemic.12 Further, the project provided insights into the impact of context (in this case, level of health service delivery) on evidence implementation in SSA.12
Case study 4: improving practices on the use of peripherally inserted central catheter in a large tertiary hospital in BrazilAs with other intravenous therapies, the use of peripherally inserted central catheter (PICC) may cause complications related to obstruction, displacement, and infectious processes, mainly because of inadequate maintenance.14 Major complications can include bloodstream infection, venous thrombosis, obstruction, fracture and migration of the device, and leakage.15–17 To avoid such complications, healthcare professionals need to implement best practices in handling the PICC. In Brazil, PICC insertion and removal is performed by a trained nurse using an ultrasound. An implementation project related to PICC management in adult and pediatric patients was conducted in a highly complex teaching hospital, specializing in cardiology and pneumology, in São Paulo, Brazil. The project was conducted across six inpatient units, six ICUs, and in the emergency room.
Two experienced nurses with senior roles in the participating hospital and a nursing professor from an affiliated university delivered the JBI EITP. The EITP trainers who work in the participating hospital identified project leads (EITP participants) for each participating site. The trainers conducted a workshop on audit and feedback to the project leads, assisted with the development of project plans, provided feedback and methodological support to the participating sites, ensured progress of the project, and assisted with the analysis of audit results. Within each participating site, the project leads organized a team of four nurses who acted as PICC champions and facilitated the identification of barriers relevant to their units. The project team examined availability of resources within their units, their communication system and the knowledge and skills of the staff relevant to the care of patients with PICC. They also evaluated the care delivered by nurses to pediatric and adult patients with PICC during their hospitalization, against best practice recommendations. As many of the barriers identified were common across sites, PICC champions collaborated to develop strategies which focused on sourcing educational materials and improving the knowledge of the staff regarding best practice for handling PICCs. Two specialist cardiology nurses provided additional facilitation support by assisting the PICC champions in developing educational resources, with education delivered to all nursing staff. The PICC champions then delivered the education to the nurses, technicians and nursing assistants within their units.
Education sessions on this topic continue on a regular basis since the commencement of the project in 2018. On-going audits of PICC practices continue to show good to excellent compliance with best practice recommendations on PICC insertion, maintenance, and removal.
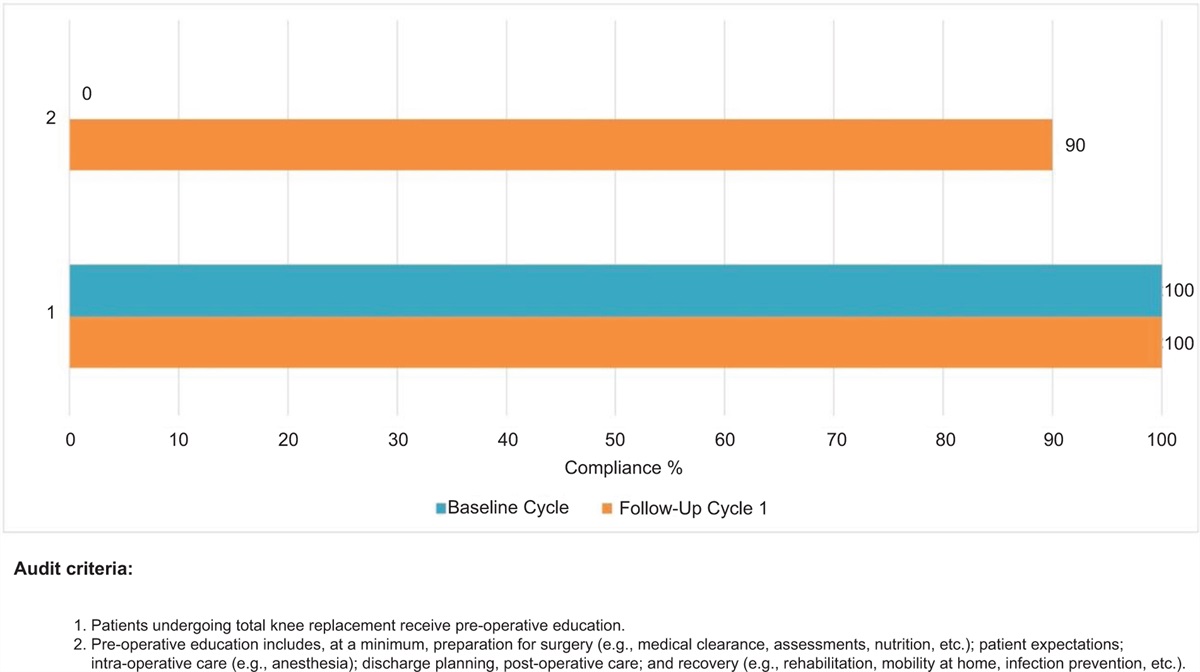
Case study 5: improving postoperative pain management among surgical trauma patients in an acute hospital ward in SpainPoorly controlled postsurgical pain can slow down recovery, impair function and quality of life, increase morbidity, prolong the hospital stay and increase the cost of care.18 Research suggests that postoperative pain is poorly managed in greater than 80% of surgical patients.18 In Spain, similar outcomes have been observed, with data indicating that more than 50% of surgical patients present with moderate or severe postoperative pain.19,20 Effective postoperative pain management has, therefore, been considered a priority in many healthcare systems in Spain. One of the initiatives that achieved success was an implementation project related to post-operative pain management among surgical patients in the trauma unit of an urban hospital in Galicia.21
Facilitation for this project occurred at different levels of the hospital system. The project commenced with the establishment of an implementation team committed to transformational change. The team consisted of eight individuals including the supervisor of the trauma unit (acted as project lead) and two of their nursing staff, two nurses from the quality unit, the supervisor from the teaching unit, a nurse from the pain unit and a supervisor from another hospital unit (this hospital unit is integrated in the same health area as the participating trauma unit and share the same management board). The project lead participated in the JBI EITP, and was responsible for coordinating the clinical audits, development of the project proposal and evaluation of findings and preparation of report.
The members of the team served as champions for the innovation, assisted in data collection, engaged with relevant staff to obtain buy-in and their input for development of strategies, design of implementation strategies and their implementation, and performed data analysis. Nurses from the trauma unit trained their colleagues around best practices in pain management and led the development of care plans, and resources and information sheets for patients. Nurses from the quality unit facilitated the approval of the new care plans by the hospital's Protocols Committee and the inclusion of this innovation in the nursing record system (called GACELA). A pain committee was also organized, consisting of anesthesiologists and the management board (Medical and Nursing Directors). The role is focused on improving awareness about pain assessment and management across the hospital, organizing communication channels and collaboration across healthcare professionals, development of guidelines, processes and protocols and ensuring the implementation of the new practices. Implementation researchers from the Spanish Centre for Evidence Based Nursing and Healthcare who conducted the JBI EITP provided peripheral support in terms of evidence implementation methodology and as-needed follow-up with the project lead to ensure that the project progressed as planned.
DiscussionThe cases presented in this article highlighted that facilitation is a multifaceted process that can be met through a variety of roles that address aspects of education and capacity building, collaboration, action planning, problem solving and evaluation. Despite variations in settings, clinical areas of implementation and target population, clear commonalities regarding facilitation activities were identified across cases. Additionally, facilitation in all cases appeared to be collaborative, with multiple ‘players’ within and outside of the health organization being involved in the process. This has been recognized by other researchers in the field, with some referring to it as blended facilitation where a team-based approach that leverages the complementary skills and expertise of external and internal facilitators is used.22–24 Although there are commonalities, facilitation activities involved some level of local contextualization where there were unique or additional activities performed to accommodate the local needs and requirements of the health organization involved in each case, as well as methodological guidance or assistance with the development, implementation and analysis of findings and/or disseminating the findings. In this article, where cases of facilitation occurred as part of the JBI EITP, numerous contextual factors influenced the success of the implementation initiative.
The degree of facilitation including the range of activities that needed to take place and the mix of individuals’ knowledge and skills set appeared to be related to resource access, information needs, leadership engagement and work structure of the unit/ward or health institution where the evidence implementation occurred. For example, in case 1 (Australia) external facilitators provided technical research support (i.e. for skills related to evidence implementation process) to achieve the intended outcomes of the project whereas in case 2 (USA), the external facilitators offered the project team clinical expertise on the topic area. Case 2 (USA) facilitators from within the organization were also a mix of senior leadership and frontline clinicians to perform a range of roles including provision of funding, administration of surveys, training and education, data collection and implementation of strategies whereas in other cases, there was an emphasis on the role of frontline clinicians and junior staff. What this highlights is that facilitation should be flexible so that it responds to the local context. This is similar to the findings of a systematic review on facilitation, which identified tailoring of approach to accommodate the needs of the practice context as being associated with positive healthcare outcomes.25 These experiences are also in line with the findings of a study conducted by Nguyen et al. in 2020,26 where the facilitation strategies applied in two different practice settings, although similar, were applied in different ways between contexts.26 One site had fewer resources and staff, which made it challenging for facilitators to balance teaching and capacity building with making the changes to the practice. The other site, on the other hand, had an existing infrastructure that allowed the facilitators to focus on capacity building. A similar approach was reported in another study, which described strategies for facilitation based on the contextual characteristics of a neonatal ICU implementing antibiotic stewardship.27 Hence, knowing which activities and roles (or which combinations) are required in a particular setting or situation is key to the effectiveness of facilitation as a strategy for implementation. The examples of facilitation provided in this article show how complex the interactions are between the participants (facilitators) and their activities (facilitation) and the context in which evidence implementation takes place.
ConclusionThe cases reported in this article outline the specific roles or activities performed by facilitators of evidence implementation initiatives conducted in various clinical areas in different geographical locations. The cases highlight the complex nature of facilitation as a strategy for evidence implementation, indicating that contextual attributes and features define the range of knowledge, skills and activities that should take place for facilitation to be effective. Although there appears to be some core components, tailoring and adaptation of the facilitation process (or roles) is required. This article calls for future studies that will link facilitation strategies with specific context attributes and features to assist in the design of evidence implementation initiatives.
AcknowledgementsConsent for publication: All authors consented to the publication of this manuscript.
Availability of data and materials: not applicable.
Authors’ contributions: L.L., D.S. conceptualized the manuscript; S.M., B.P., R.R. assisted in writing the manuscript; L.L., A.M., L.A.-M., D.P., J.B., M.B., V.P., E.I.G.-M., C.M. wrote the case studies.
Conflicts of interestAll authors are JBI EITP trainers or have previously been a trainer. L.L., A.M. are paid employees of JBI Adelaide.
References 1. Jordan Z, Lockwood C, Munn Z, Aromataris E. The updated JBI model for evidence-based healthcare. The Joanna Briggs Institute. Int J Evidence Based Healthc 2019; 17:58–71. 2. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care 1998; 7:149–158. 3. Berta W, Cranley L, Dearing J, Dogherty E, Squires J, Estabrooks C. Why (we think) facilitation works: insights from organizational learning theory. Implement Sci 2015; 10:141. 4. Dogherty E, Harrison M, Graham I. Facilitation as a role and process in achieving evidence-based practice in nursing: a focused review of concept and meaning. Worldviews Evid Based Nurs 2010; 7:76–89. 5. McArthur A, Munn Z, Lizarondo L, et al. The ripple effect of evidence implementation: a descriptive evaluation of JBI's Evidence-based Clinical Fellowship Program. JBI Evid Implement 2021; 19:142–148. 6. Australian Commission on Safety and Quality in Health Care. Delirium clinical care standard. ACSQHC. Sydney. 2016. 7. Cody S, Lizarondo L, McArthur A, et al. Improving the quality of delirium practices in a large Australian tertiary hospital: an evidence implementation initiative. Aust J Adv Nurs 2021; 38:3–12. 8. American Psychiatric Nurses Association (APNA). Violence prevention: APNA 2016 position statement. 2016; Available at: https://www.apna.org/news/violence-prevention/. [Accessed 6 December 2021]. 9. American Psychiatric Nurses Association. (2008). Workplace violence: APNA 2008 position statement. 10. American Association of Occupational Health Nurses (AAOHN). Preventing workplace violence: the occupational and environmental health nurse role. Workplace Health Saf 2014; 62:48–50. 11. Badeaux J, Triche T, Bennett M. Reduction of aggressive and violent behavior toward behavioral health unit staff and other patients: a best practice implementation project. JBI Evid Implement 2020; 19:177–189. 12. Metto D, Kiptoon S, Esiromo M, et al. Improving the capacity of healthcare professionals to stem the spread of Covid-19 in Kenya: final report. Available at: https://bit.ly/3lDETEq. [Accessed 6 December 2021]. 13. Keats E, Macharia W, Singh N, et al. Accelerating Kenya's progress to 2030: understanding the determinants of under-five mortality from 1990 to 2015. BMJ Glob Health 2018; 3:e000655. 14. Cotogni P, Pittiruti M. Focus on peripherally inserted central catheters in critically ill patients. World J Crit Care Med 2014; 3:80–94. 15. Leroyer C, Lasheras A, Marie V, et al. Prospective follow up of complications related to peripherally inserted central catheters. Med Mal Infect 2013; 43:350–355. 16. Parás-Bravo P, Paz-Zulueta M, Sarabia-Lavin R, et al. Complications of peripherally inserted central venous catheters: a retrospective cohort study. PLoS One 2016; 11:e0162479. 17. Nolan ME, Yadav H, Cawcutt KA, Cartin-Ceba R. Complication rates among peripherally inserted central venous catheters and centrally inserted central catheters in the medical intensive care unit. J Crit Care 2016; 31:238–242. 18. Gan T. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res 2017; 10:2287–2298. 19. Gallego JI, Rodríguez de la Torre MR, Vázquez-Guerrero JC, Gil M. Estimation of the prevalence and severity of postoperative pain and relation with patient satisfaction. Rev Soc Esp Dolor 2004; 11:197–202. 20. Galí J, Puig C, Carrasco G, et al. [Experience in the multidisciplinary management of acute postoperative pain]. Experiencia en el tratamiento multidisciplinar del dolor agudo postoperatorio. Rev Calidad Asistencial 2004; 19:296–303. 21. García-Monasterio EI, Alvárez-Vázquez JC, Morado-Quiñoá P, et al. Postoperative pain management among surgical trauma patients in an acute ward: a best practice implementation project. JBI Database System Rev Implement Rep 2019; 17:1941–1953. 22. Pimentel C, Mills W, Palmer J, et al. Blended facilitation as an effective implementation strategy for quality improvement and research in nursing homes. J Nurs Care Qual 2019; 34:201–216. 23. Smith S, Liebrecht C, Bauer M, Kilbourne A. Comparative effectiveness of external vs blended facilitation on collaborative care model implementation in slow-implementer community practice. Health Serv Res 2020; 55:954–965. 24. Connolly SL, Sullivan JL, Ritchie MJ, Kim B, Miller CJ, Bauer MS. External facilitators’ perceptions of internal facilitation skills during implementation of collaborative care for mental health teams: a qualitative analysis informed by the i-PARIHS framework. BMC Health Serv Res 2020; 20:165. 25. Moussa L, Garcia-Cardenas V, Benrimoj S. Change facilitation strategies used in the implementation of innovations in healthcare practice: a systematic review. J Chang Manag 2019; 19:283–301. 26. Nguyen A, Cuthel A, Padgett D, et al. How practice facilitation strategies differ by practice context. J Gen Intern Med 2020; 35:824–831. 27. Quinn J, Gephart S, Davis M. External facilitation as an evidence-based practice implementation strategy during an antibiotic stewardship collaborative in neonatal intensive care units. Worldviews Evid-based Nurs 2019; 16:454–461.
留言 (0)