
記住我
What is known about the topic?
The prevalence of coronavirus disease 2019 (COVID-19) is higher among frontline healthcare workers (HCWs) due to their occupational exposure. Given the healthcare-associated infections, critical protective measures must be introduced for HCWs. Clinical audits are useful tools for evaluating the existing practice and implementing the best practice related to the protection of nurses against COVID-19 in the emergency department.What does this article add?
A clinical audit can be used as a suitable tool to improve our performance. This tool is very effective in analyzing and examining the current situation and applying appropriate interventions with the aim of resolving issues and problems. Interventions including educational programs and meetings can facilitate the implementation of evidence in clinical practice. Top-level healthcare managers might use these results to implement the suggested interventions in their settings to improve the protection of nurses working in the emergency department against COVID-19. IntroductionThe novel coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with typical symptoms of fever and respiratory tract infections in patients.1 This disease, which originated in Wuhan, China in December 2019, has been spreading around the world quickly. The first case of this infectious disease in Iran was announced on February 19, 2020, in Qom.2 Thus, Iran's Ministry of Health and Medical Education (MOHME) established the scientific committee of COVID-19 on February 24 to release and update diagnostic and therapeutic guidelines.3
The prevalence of COVID-19 is higher among frontline healthcare workers (HCWs) due to their occupational exposure. In Italy, HCWs accounted for 10.5% of all COVID-19 cases in April 2020, of which 43.2% included nurses and midwives.4 Results of a systematic review and meta-analysis indicated that the number of HCWs infected with SARS-CoV-2 ranged between 4.2% in China to 17.8% in the United States.5 Findings of a Chinese study showed that 17.5% of HCWs were infected in emergency departments.6 These HCWs are often asymptomatic carriers of the infection, transmitting it silently in both clinical and community contexts.7
The prolonged exposure of HCWs to COVID-19 patients, along with high workload, stress, and anxiety as a result of the COVID-19 pandemic and sometimes limited awareness regarding personal protection or shortage of personal protective equipment, especially at the beginning of the pandemic, have put HCWs at risk of acquiring COVID-19.8
The impact of COVID-19 infection on HCWs is substantial, leading to medical resources shortage and partial closure of hospitals, among other things. Therefore, critical protective measures for HCWs must be introduced. Hand sanitization and respiratory protection for both workers and patients were emphasized by hospitals. Also, identifying at-risk people and monitoring them were other actions taken in hospitals and healthcare settings.9,10 Training HCWs about different aspects of infection and standard precautions was an effective method in China at the beginning of the pandemic.11
Given that the importance of protecting HCWs is undeniable as patients cannot be stopped from treatment and transmitting the infection from HCWs to the community is at high risk, also considering that the emergency department is the first point in hospitals where patients face healthcare providers, this research aims to evaluate the current practice and implement the best practice related to the protection of nurses in the emergency department against COVID-19 at a teaching hospital in Tabriz, Iran.
ObjectivesThis evidence implementation project aimed to improve the protection of nurses against COVID-19 in the emergency department at a teaching hospital in Tabriz, Iran.
The specific objectives were:
To determine current compliance with best practice recommendations for the protection of nurses against COVID-19 in the emergency department. To identify barriers and facilitators to improving compliance and develop strategies to address areas of non-compliance. To evaluate changes in compliance with the evidence-based practice recommendations following the implementation of strategies to address the barriers and to enhance the facilitators. MethodsThis evidence implementation project used the JBI Evidence Implementation framework.12 The JBI Implementation approach is grounded in the audit and feedback process along with a structured approach to the identification and management of barriers to compliance with recommended clinical practices. It consists of seven stages including, (1) identification of practice area for change, (2) engagement of change agents, (3) assessment of context and readiness to change (i.e., situational analysis), (4) review of practice (i.e., baseline audit) against evidence-based audit criteria, (5) implementation of changes to practice, (6) re-assessment of practice using a follow-up audit and (7) consideration of the sustainability of practice changes.
This evidence implementation project used the JBI Practical Application of Clinical Evidence System (JBI PACES), and Getting Research into Practice (GRiP) audit and feedback tool.12 The JBI PACES and GRiP framework for promoting evidence-based healthcare involves three phases of activity:
1. Establishing a team for the project and undertaking a baseline audit based on the criteria informed by the evidence. 2. Reflecting on the results of the baseline audit, and designing and implementing strategies to address non-compliance found in the baseline audit, informed by the GRiP framework. 3. Conducting a follow-up audit to assess the outcomes of the interventions implemented to improve practice and to identify future practice issues to be addressed in subsequent audits. SettingThis implementation project was undertaken in the emergency department of a teaching hospital in Tabriz, Iran with 35 active beds and 37 nurses.
Ethical considerationsThis project was registered as a quality improvement activity within the hospital; therefore, it did not require ethical approval. Despite this, the audit activity and the quality improvement process were overseen by the ethical committee in our organization to ensure all ethical considerations are in agreement with safeguarding the rights, safety, and dignity of the participants.
Phase 1: Stakeholder engagement and baseline auditThe audit team consisted of a lecturer who presented the results of each phase to the whole stakeholders and audit team, one head nurse who was the coordinator in the ward, a PhD in health policy who designed the project and managed the audit team in all phases, a quality assurance specialist at the hospital for conducting the interventions in phase 2, two MSc nurses for collecting data, and one PhD for analyzing the data. The audit criteria, which were derived from the best available evidence,13 included the following ten items:
I. HCWs receive standardized infection prevention and control (IPC) training. II. HCWs show competency in the assessment, donning, use, and doffing of personal protective equipment (PPE). III. HCWs have been made aware of information relating to the current COVID-19 situation. IV. All patients presenting to a healthcare facility suspected of COVID-19 are triaged. First-line triage may be undertaken face-to-face, by telephone or telemedicine, or other online services. V. Separate areas are made available for triage, assessment, and management. VI. Suspected COVID-19 cases are identified as soon as possible, tested, and isolated in appropriate facilities. VII. Social distancing (according to local advice) is established at the triage station. VIII. A handwashing station is provided at the triage station for HCWs, patients, and visitors. IX. Standardized IPC precautions are taken by all HCWs (e.g. hand hygiene, cough etiquette, risk assessment to determine PPE [mask, gown, apron, gloves, and eye protection] requirements, correct use of PPE, and environmental cleaning). X. A point-of-care risk assessment of the patient is undertaken which includes taking temperature, documenting symptoms (or absence of), and asking about self-quarantine.The audit criteria were translated into Persian by two of the researchers and were assessed by interviewing nurses. All of the 37 nurses, who provided services in three shifts, were involved in the study to answer criteria 1 through 10. A meeting was conducted to familiarize the members with the project and discuss the audit criteria and data collection procedures. The data collection process included direct observation, interview, and a checklist (Appendix 1, https://links.lww.com/IJEBH/A88, https://links.lww.com/IJEBH/A89) for checking the compliance of three audit criteria. The baseline audit to detect current practices and implement the best practice related to the protection of nurses against COVID-19 in the emergency department was carried out in the first week of August 2021. Table 1 shows the evidence-informed audit criteria in the project (baseline and follow-up audit) as well as a description of the sample and approaches to measure compliance with the best practice for each audit criterion.
Audit criterion Sample Method(s) used to measure compliance with best practice Healthcare workers receive standardized infection prevention and control (IPC) training Baseline: 37 nursesFollow up: 37 nurses Interviewing nursesUsing the checklist Healthcare workers show competency in assessment, donning, use and doffing of personal protective equipment (PPE) Baseline: 37 nursesFollow up: 37 nurses Interviewing nursesUsing the checklist Healthcare workers have been made aware of information relating to the current COVID-19 situation Baseline: 37 nursesFollow up: 37 nurses Interviewing nursesUsing the checklist All patients presenting to a healthcare facility suspected of COVID-19 are triaged. First line triage may be undertaken face-to-face, by telephone or telemedicine, or other online service Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklist Separate areas are made available for triage, assessment and management Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklist Suspected COVID-19 cases are identified as soon as possible, tested, and isolated in appropriate facilities Baseline: 37 nursesFollow up: 37 nurses Interviewing nursesUsing the checklist Social distancing (according to local advice) is in place at the triage station Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklist A handwashing station is provided at the triage station for use by healthcare workers, patients and visitors Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklist Standardized IPC precautions are taken by all healthcare workers (e.g. hand hygiene, cough etiquette, risk assessment to determine PPE [mask, gown, apron, gloves, and eye protection] requirements, correct use of PPE, and environmental cleaning) Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklist A point-of-care risk assessment of the patient is undertaken which includes taking temperature, documenting symptoms (or absence of), and asking about self-quarantine, at the least Baseline: 37 nursesFollow up: 37 nurses ObservationInterviewing nursesUsing the checklistCOVID-19, coronavirus disease 2019.
Audit results were analyzed following the baseline audit to identify gaps between the current practice and the best practice recommendations. One of the project team members summarized areas of excellent (over 75%), moderate (50–75%), and low (< 50%) performance and announced it to others in the meeting sessions. Three sessions were held and all the members brainstormed barriers to the best practice, identified strategies, and resources to overcome the barriers, and implemented strategies. One of the nurses in the team moderated these sessions. In these sessions, all of the team members were encouraged to participate in identifying barriers and strategies. All of the viewpoints were written on the board and were discussed and prioritized by the team members. We used the JBI GRiP tool to recognize barriers in practice and suggest changing strategies for possible improvement. Also, the resources needed for the implementation of strategies were discussed by the audit team. We discussed the GRiP report in three face-to-face meetings and gathered the opinions of the key stakeholders. Phase 2 was conducted between September and November 2021.
Phase 3: Follow-up audit post-implementation of change strategyA follow-up audit was carried out for three days in December 2021 using the same approaches as the baseline audit to evaluate changes in nurses’ compliance with the same evidence-based audit criteria. The baseline audit included all of the 37 nurses, with a similar number involved in the follow-up audit. Results of the follow-up audit and any other details about the process were disseminated back to stakeholders through four sessions, held 15 days apart.
The changes in compliance were measured by descriptive statistics embedded in JBI-PACES in the form of percentage changes from the baseline.
Results Phase 1: Baseline auditThe results of the baseline audit showed that the compliance rates were as follows: criterion 1 (receiving standardized infection prevention) and criterion 2 (competency of HCWs) were 95% and 97%, respectively. When it comes to criterion 3 (HCWs’ awareness) and criterion 4 (triaging of all suspected patients), the compliance rates were 86% and 41%, respectively. Also, the compliance rates for criterion 5 (availability of separate areas for triage) and criterion 6 (identifying, testing, and isolating suspected cases) were 86% and 84%. Finally, the compliance rates for criterion 7 (social distancing at the triage station), criterion 8 (provided handwashing station at the triage station), criterion 9 (taking standardized IPC precautions by all HCWs), and criterion 10 (undertaking a point-of-care risk assessment of the patient) were 30%, 22%, 70% and 95%.
Phase 2: Strategies for Getting Research into Practice (GRiP)Five barriers to compliance with the best practice were identified and strategies to overcome these barriers – as summarized in Table 2 – were formulated and then implemented by the project team. Barriers, their brief descriptions, strategies for overcoming the barriers, resources needed for the improvement, and the resulting outcomes for each barrier are described in the following.
Table 2 - Getting Research into Practice matrix Barrier Strategy Resources Outcomes Staff shortage in emergency departments and lack of time to triage for suspected COVID-19 patients due to nursing workloads Hiring more than one nurse in charge of patient triageModifying procedures Hiring extra staffDeveloping guidelines, policies and procedures Optimization of services in the triage of suspected COVID-19 patients Weaknesses in adhering to proper social distancing by patients due to lack of space Developing physical space suitable for the triage unit Financial resourcesGuidelinesMeetings Improvement in the physical space of the triage unit Weaknesses in using absentia methods for patients’ triage Running face-to-face educational sessions for nurses Face-to-face trainingEducational slides & videosHuman resources Improvement of the absentee triage process Weaknesses in adhering proper social distancing in the triage unit due to negligence of patients, nurses and managers Applying educational strategiesRaising the awareness of managers, nurses, and patientsContinuous control by the head nurse about policies and proceduresExplaining patients that distancing is an effective way to protect them against infection WorkshopMeetingsEducational pamphlets for patientsNew rulesRe-assessment tools Increasing adherence to social distancingIncreasing the commitment of managers and nurses regarding social distancing Lack of an appropriate place for hand washing in the triage unit Allocating an appropriate place for hand hygiene GuidelinesRedesigning the triage unitFinancial resources Improving the hand hygiene processCOVID-19, coronavirus disease 2019.
Barrier 1: Staff shortage in the emergency department and lack of time to triage suspected COVID-19 patients due to nursing workloads.
Since the COVID-19 pandemic began, nurses have been overwhelmed with work as the number of patients referred to emergency departments doubled. The strategies for this barrier included hiring more than one nurse in charge of patient triage and modifying procedures. This happened by applying two nurses from other wards in the crowded working rounds. The resources included hiring additional employees and developing guidelines, policies, and procedures. The content of these guidelines was about how to devote a nurse from another ward, calculating his/her working time and wage. These guidelines were developed based on the hospital's rules and context. The resulting outcome was the optimization of services in the triage of suspected COVID-19 patients.
Barrier 2: Weaknesses in adhering to proper social distancing by patients due to lack of space
For this barrier, we attempted to develop a physical space suitable for the triage unit. Therefore, the required resources were financial resources, guidelines, and meetings. Two meetings were held with the hospital manager and were organized and moderated by one of the nurses in the team. The result of the meetings was devoting an empty room in the emergency department for patient triage. The outcome of this barrier was the improvement in the physical space of the triage unit.
Barrier 3: Weaknesses in using absentia methods for patients’ triage
The strategy to overcome this barrier was running three face-to-face educational sessions for nurses through educational slides and videos. All of the nurses in the emergency department participated in these sessions based on their working rounds. The content of the meetings that was provided by two of the nurses in the project team was absentia methods of patient triage. These methods are suitable for patients with mild symptoms, in a way that telephone calls were used for this reason. Based on the oral feedback from participating nurses, the meetings and the content were acceptable. The expected outcome was the improvement of using absentia methods of patient triage.
Barrier 4: Weaknesses in adhering to proper social distancing in the triage unit due to the negligence of patients, nurses, and managers
For this barrier, we attempted to apply educational strategies, raise the awareness of the managers, nurses, and patients, perform continuous control monitoring by the head nurse about policies and procedures, and persuade patients that distancing is an effective way to protect them against infection. We held workshops and meetings, offered educational pamphlets for 37 patients, set new rules, and used a structured checklist as a re-assessment tool. The workshops, meetings, and pamphlets were all about the importance of social distancing, and the content of which was developed based on the international guidelines for social distancing in COVID-19. The outcomes included increased adherence to social distancing and managers’ and nurses’ increased commitment to social distancing.
Barrier 5: Lack of an appropriate place for hand washing in the triage unit
The only strategy for overcoming this barrier was allocating an appropriate place for hand hygiene. The required resources for overcoming this barrier were guidelines, redesigning the triage unit, and financial resources, as the most important factor. The expected outcome for this barrier was improving the hand hygiene process; however, this barrier was the only barrier that we could not reach the expected outcome due to the lack of financial resources.
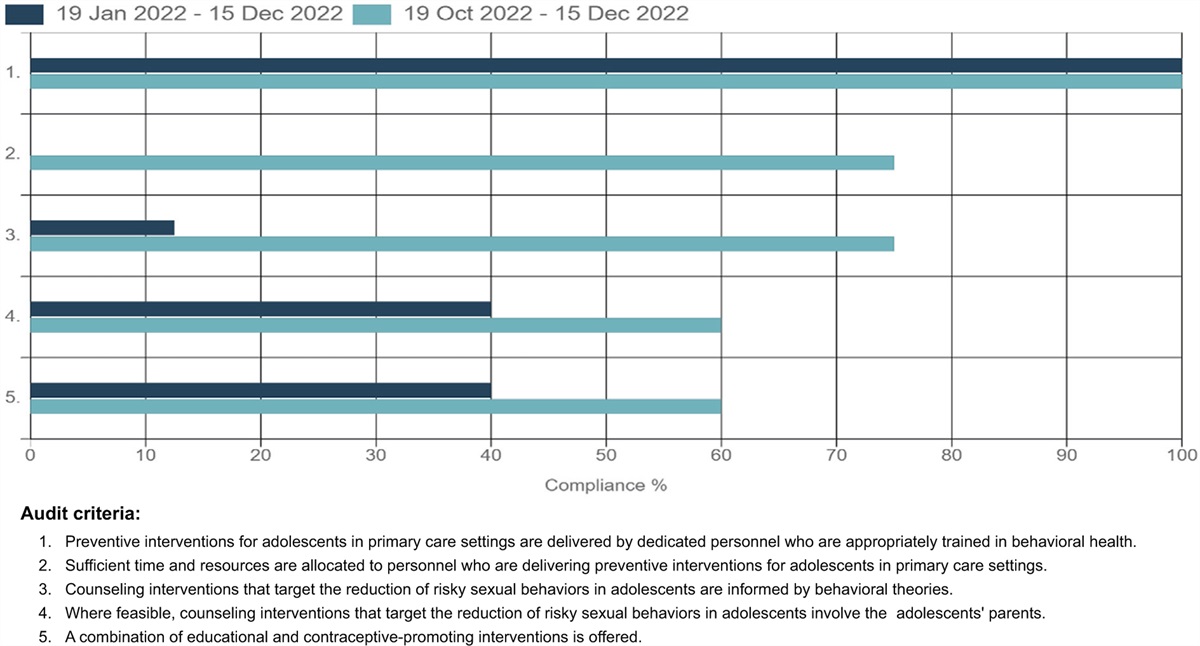
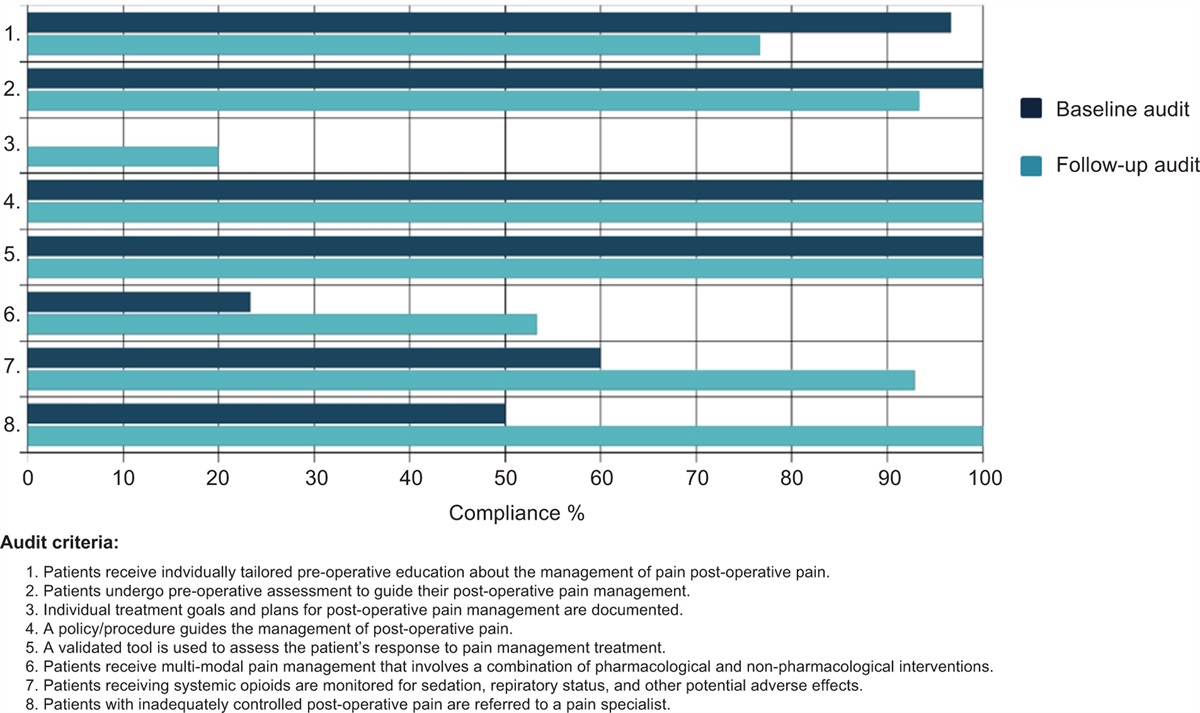
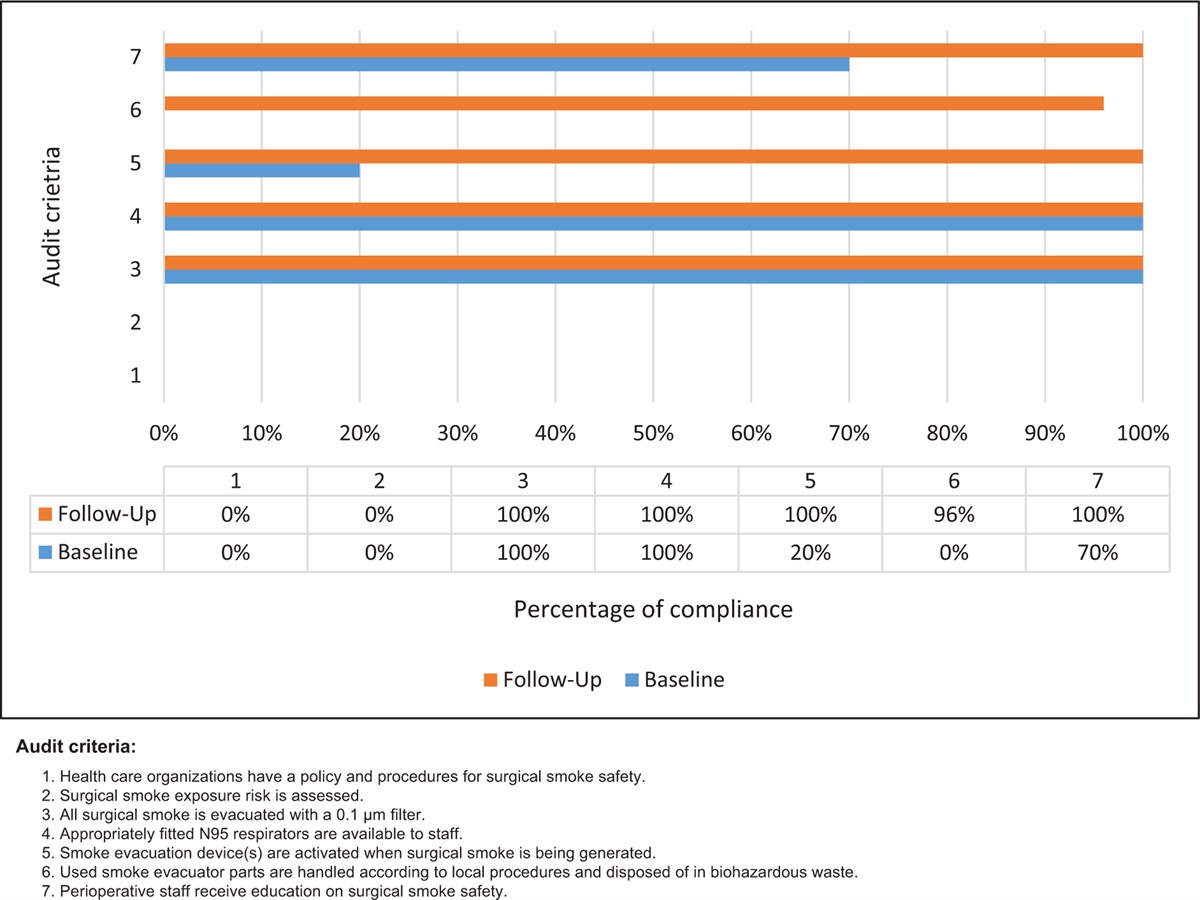
Phase 3: Follow-up auditThe compliance rate of all the audit criteria (in percentages), as examined in the follow-up audit, together with the results from the baseline audit are displayed in Fig. 1. The comparison of the follow-up audit results with those of the baseline audit showed an overall improvement in compliance with the best practice recommendations. There was a significant improvement, especially in criteria 4 and 7. The other criteria showed no significant change. Criterion 1 improved from 95% to 97%, criterion 3 increased from 86% to 95%, criterion 5 improved from 86% to 89%, criterion 6 increased from 84% to 89%, criterion 8 improved from 22% to 27%, criterion 9 increased from 70% to 84% and criterion 10 improved from 95% to 97%. Criterion 2 remained at a compliance rate of 97%.
 FIGURE 1:
FIGURE 1: Compliance with best practice audit criteria in comparison to that of the baseline (%).
DiscussionIn the current best practice implementation project, we aimed to evaluate and improve the evidence-based practices in protective measures against COVID-19 among nurses in an emergency department in Tabriz, Iran. Following a baseline and follow-up audit cycle using the JBI-GRiP tool, in this project, we achieved improvements in compliance of all except one criterion with the best practice in the field of protective measures against COVID-19 among nurses in the emergency department.
The audit cycle showed that six (out of ten) criteria have reached compliance above 75% at the baseline and all of them were improved in the follow-up audit except one. The first audit criterion [HCWs receive standardized infection prevention and control (IPC) training] reached 95% and 97% of compliance with the standards at the baseline and follow-up audits. Since the beginning of the COVID-19 pandemic in the world, online or face-to-face training about infection prevention and control measures has been presented to nurses, other HCWs, and medicine and nursing students.14 Results of a study showed that there was some good knowledge about the prevention and control of COVID-19 among HCWs in Ethiopia even though the practice was poor. Access to vast information sources was the reason for high knowledge about the prevention and control of COVID-19. On the other hand, lack of time, shortage of personal protective equipment, and heavy workload led to poor practice.15
The results of the current study showed that HCWs were reasonably compliant with the best practice in assessing, donning, using, and doffing personal protective equipment both in baseline and follow-up audits (criteria 2 and 9). Results of a study indicated that lack of personal protective equipment, limited access to medications, together with a shortage of human resources were the main challenges of cancer treatment at the beginning of the pandemic.16 Due to the high risk of developing COVID-19 infection among HCWs, patients, and their caregivers, lack of access to personal protective equipment during the pandemic has become a critical concern worldwide, leading to stress among staff.17 Since the current study was conducted after the fifth wave of the pandemic in Iran, when the rate of COVID-19 infection and death had been decreasing, the supply of personal protective equipment was adequate. Based on the results of the current study, nurses in the emergency department were aware of the current COVID-19 situation in both audit phases. Results of research conducted in Iran showed that nurses had good knowledge about the COVID-19 pandemic, which was obtained through media including websites, WhatsApp messenger, and TV.18 This finding substantiates recent studies conducted during the current and previous pandemics.19
The baseline and follow-up audit results of the current study showed that the triage system of COVID-19 suspected patients complied with the best practice – 81% in both phases of criterion 4 and 95% versus 97% in criterion 10. Different triage algorithms and tools are used in different settings.20 In this infection control measure, the contact history of the patient as well as the main complaint, medical history, signs, and symptoms are obtained so that the patient can be prescreened to ensure that the process can continue.21 Results of an Iranian study showed that the telephone-based COVID-19 triage system, according to patients’ symptoms and activation of home isolation, has been effective in decreasing the unnecessary referrals of patients to the hospital.22 Another triage system in Iran was based on the teleconsultation strategy, which provided a reliable triage of COVID-19 infection using radiology experts from all over the world.23
The baseline audit in the current study showed that social distancing in the triage station of acute care setting was not compliant with the best practice (the compliance rate was 22%). This criterion was improved after the intervention; however, the compliance rate in the follow-up audit was 62%. The social distancing policy of 1.8 m was announced and implemented in Iran on March 27, 2020. The policy was endorsed by social media and supported through different campaigns. This policy has shown to be effective in reducing infection cases and deaths from COVID-19.24 Results of a similar study indicated that the risk of acquiring COVID-19 was high among HCWs due to non-compliance with workplace social distancing policies, especially during lunchtime.25
The results of the baseline audit in the current research showed that handwashing station provisions for nurses and patients were 22% compliant with the best practice, which remained the same after the follow-up audit (27%). Results of another study showed that there is adequate knowledge and awareness among nurses regarding the importance of hand washing in preventing COVID-19 infection.26 The non-compliance with hand hygiene practices was due to a lack of financial resources to provide a station in the triage. In his review, Desye likewise found that the shortage of financial resources was the main challenge in providing water, sanitation, and hygiene services in low-income countries.27
Strengths and limitations of the studyTo the best of our knowledge, this was the first study that assessed the current practice and implemented the best practice for nurses’ protection against COVID-19 infection in Iran. However, one of the criteria in the current project did not improve after the intervention (handwashing station). Given that financial resources were demanded to set up a place for hand hygiene, it was infeasible in the middle of the year without a specific budget. We plan to re-audit this item after 3–6 months to observe the improvement.
ConclusionWe used a clinical audit cycle in the current evidence implementation project to evaluate the existing practice and implement the best practice related to the protection of nurses against COVID-19 in the emergency department of a teaching hospital in Tabriz, Iran. The results of the audit process showed an improvement in protective measures against COVID-19. It can be concluded that interventions such as nursing education through various approaches including face-to-face training, providing educational pamphlets, and conducting workshops and meetings can facilitate the implementation of evidence into practice. Further follow-up audits will be required to monitor the process change. Other interventions can be implemented as needed. The results of this study can be used in other similar contexts to improve protective measures against COVID-19 for nurses and other HCWs at hospitals.
AcknowledgementsThe authors would like to acknowledge the support of the Joanna Briggs Institute, all the Sina hospital's staff for getting involved in this audit project, Tabriz University of Medical Sciences and Research Center for Evidence Based Medicine.
Conflicts of interestThere are no conflicts of interest.
References 1. Lai C-C, Ko W-C, Lee P-I, et al. Extra-respiratory manifestations of COVID-19. Int J Antimicrob Agents 2020; 56:106024. 2. WHO. Coronavirus disease 2019 (COVID-19) Situation Report – 31. Geneva: WHO; 2020. 3. MOHME. Iran's Diagnostic Therapeutic Flowchart for COVID-19; 1st ed. (DTFC1); 2020. 4. Kursumovic E, Lennane S, Cook TM. Deaths in healthcare workers due to COVID-19: the need for robust data and analysis. Anaesthesia 2020; 75:989–992. 5. Sahu AK, Amrithanand VT, Mathew R, et al. COVID-19 in health care workers – a systematic review and meta-analysis. Am J Emerg Med 2020; 38:1727–1731. 6. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020; 323:1061–1069. 7. Gómez-Ochoa SA, Franco OH, Rojas LZ, et al. COVID-19 in health-care workers: a living systematic review and meta-analysis of prevalence, risk factors, clinical characteristics, and outcomes. Am J Epidemiol 2021; 190:161–175. 8. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect 2020; 105:100–101. 9. Chersich MF, Gray G, Fairlie L, et al. COVID-19 in Africa: care and protection for frontline healthcare workers. Global Health 2020; 16:1–6. 10. Jeon YW, Park ES, Jung SJ, et al. Protection of healthcare workers against COVID-19 at a large teaching hospital in Seoul, Korea. Yonsei Med J 2020; 61:631. 11. Zhou P, Huang Z, Xiao Y, et al. Protecting Chinese healthcare workers while combating the 2019 novel coronavirus. Infect Control Hosp Epidemiol 2020; 41:745–746. 12. Porritt K, McArthur A, Lockwood CZM. JBI Handbook for Evidence Implementation. Adelaide: JBI; 2020. 13. Marin T, Magtoto L. Evidence summary. Coronavirus disease 2019 (COVID-19): healthcare workers in acute care settings – triage. The JBI EBP Database 2021; JBI-ES-1303-4. 14. Ng Y-M, Or PLP. Coronavirus disease (COVID-19) prevention: virtual classroom education for hand hygiene. Nurse Educ Pract 2020; 45:102782. 15. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health 2020; 48:72. 16. Jazieh AR, Akbulut H, Curigliano G, et al. Impact of the COVID-19 pandemic on cancer care: a global collaborative study. JCO Global Oncol 2020; 6:1428–1438. 17. Ranney ML, Griffeth V, Jha AK. Critical supply shortages – the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med 2020; 382:e41. 18. Nemati M, Ebrahimi B, Nemati F. Assessment of Iranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Arch Clin Infect Dis 2020; 15:e102848. 19. Kim JS, Choi JS. Middle East respiratory syndrome–related knowledge, preventive behaviours and risk perception among nursing students during outbreak. J Clin Nurs 2016; 25:2542–2549. 20. Levenfus I, Ullmann E, Battegay E, Schuurmans MM. Triage tool for suspected COVID-19 patients in the emergency room: AIFELL score. Braz J Infect Dis 2020; 24:458–461. 21. Wang Q, Wang X, Lin H. The role of triage in the prevention and control of COVID-19. Infect Control Hosp Epidemiol 2020; 41:772–776. 22. NeJhaddadgar N, Ziapour A, Zakkipour G, et al. Effectiveness of telephone-based screening and triage during COVID-19 outbreak in the promoted primary healthcare system: a case study in Ardabil province, Iran. J Public Health 2020; 30:1301–1306. 23. Davarpanah AH, Mahdavi A, Sabri A, et al. Novel screening and triage strategy in Iran during deadly coronavirus disease 2019 (COVID-19) epidemic: value of humanitarian teleconsultation service. J Am Coll Radiol 2020; 17:734. 24. Saki M, Ghanbari MK, Behzadifar M, et al. The impact of the social distancing policy on COVID-19 incidence cases and deaths in Iran from February 2020 to January 2021: insights from an interrupted time series analysis. Yale J Biol Med 2021; 94:13–21. 25. Al Maskari Z, Al Blushi A, Khamis F, et al. Characteristics of healthcare workers infected with COVID-19: a cross-sectional observational study. Int J Infect Dis 2021; 102:32–36. 26. Honarvar B, Lankarani KB, Kharmandar A, et al. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health 2020; 65:731–739. 27. Desye B. COVID-19 pandemic and water, sanitation, and hygiene: impacts, challenges, and mitigation strategies. Environ Health Insights 2021; 15:11786302211029447.
留言 (0)