
記住我




Heparin-induced thrombocytopenia (HIT) is a prothrombotic life-threatening adverse immune reaction caused by heparin administration. This is due to antibodies formed against complexes of platelet factor 4 (PF4) and heparin (anti-PF4/heparin).1
A subset of anti-PF4/heparin antibodies, namely, immunoglobulin G (IgG), in high titers has platelet-activating properties that cause HIT.2,3 In addition, these antibodies activate monocytes and endothelial cells leading to thrombocytopenia and a thrombin-induced hypercoagulable state.4–7
Heparin-induced thrombocytopenia is an atypical immune response when compared with other immune-mediated diseases caused by adaptive immunity.8–10 Consequently, heparin-naive patients can develop IgG antibodies as early as day 4 like a secondary adaptive immune response, and HIT antibodies are relatively short-lived unlike those from a secondary adaptive immune response.11,12 Polyanions such as bacterial surfaces10 and nucleic acids13 also induce conformational changes in PF4 in a manner similar to heparin, leading to HIT in patients without heparin exposure. However, the mechanisms have not been fully understood.
Severely injured trauma patients are at an increased risk of tissue damage, which release nucleic acids such as DNA and RNA into their circulation. This suggests that trauma severity can be a risk factor for the formation of anti-PF4/heparin, independent of heparin administration. Although this has been demonstrated in a previous study, all patients had received either unfractionated heparin (UFH) or low-molecular-weight heparin for thromboprophylaxis, and those requiring intensive care were excluded.14 Therefore, the impact of trauma severity on HIT independent of heparin administration was not directly addressed.
In this study, we aimed to conduct a prospective, multicenter observational study to evaluate the hypothesis that severely injured patients develop HIT antibodies more frequently than non–severely injured ones, possibly independent of heparin administration.
PATIENTS AND METHODS Patients and Study DesignThis prospective observational study was multicentered and was conducted in Tohoku University Hospital (Sendai, Japan), Hokkaido University Hospital (Hokkaido, Japan), Japan Red Cross Maebashi Hospital (Gunma, Japan), Tokyo Saiseikai Central Hospital (Tokyo, Japan), and Kagawa University Hospital (Kagawa, Japan). We have not performed prior sample size calculations because it was a new field of research. The ethical committees of each of the hospitals approved the protocol of this study. All of this research and protocol were approved by Ethics Committee of Tohoku University Graduate School of Medicine (2018-1-156).
All patients gave written informed consent, and the study was conducted in accordance with the Declaration of Helsinki.
We confirmed that this study complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Digital Content, Supplementary Data 1, https://links.lww.com/TA/C394).
We prospectively enrolled trauma patients from March 2018 to February 2019. The inclusion criteria were age 18 years or older and Injury Severity Score (ISS) of ≥9. Injury Severity Score was calculated based on the Abbreviated Injury Scale (AIS) 90, using radiology reports and clinical findings. Anatomical injury sites were divided into head and neck, face, chest, abdomen, pelvis and extremities, and skin. Trauma was classified into blunt, penetrating, or other. This study included patients who did not receive any heparin, as well as those who received it as only flushes and as treatment. Prophylaxis and treatment of venous thrombosis was performed by attending physicians' discretion based on risk of each patient.
Data CollectionDuring hospitalization, clinical information including changes in the platelet count and timing of heparin administration was collected. The blood samples were drawn at day 0 (on admission), days 5 and 6, days 7 to 9, days 10 to 12, days 13 to 15, and day 30 or at the time of transfer to another department or hospital, whichever came first. If the patient was transferred or died within 30 days, the cases were treated as censoring events. The patients' sera drawn at the above timing were shipped with dry ice to the reference laboratory (Division of Transfusion Medicine, National Cerebral and Cardiovascular Center) for the assessment of HIT antibodies and were stored at −70°C until use.
Seroconversion and Serological Assays for HIT AntibodiesAntigen immunoassay was performed using a commercially available enzyme-linked immunosorbent assay (ELISA) kit to detect anti-PF4/heparin IgG antibodies (PF4-IgG; Genetic Testing Institute, Waukesha, WI). The ELISA results were expressed as optical density (OD), and the cutoff value was set at 0.4 OD, as per the manufacturer’s instructions. We defined seroconversion as testing negatively on day 0 followed by a positive test afterward. If the patient had already tested positive on day 0, seroconversion was defined as an OD increase by more than 30% or by at least 0.4 OD, according to a previous study.15
The washed platelet activation assay was performed as described in detail elsewhere.2,16 In brief, washed platelets, prepared from HIT antibody-sensitive healthy volunteers, were used. Platelet microparticles, activated by HIT antibodies in a heat-inactivated serum, were quantified by flow cytometry. Positivity was defined as washed platelet activation in the presence of a therapeutic concentration of UFH (0.1 U/mL) or low-molecular-weight heparin (0.3 U/mL), but not at very high concentrations (100 U/mL), in addition to activation inhibition by the addition of an anti-FcγRII antibody (IV.3; Stemcell Technologies, Vancouver, Canada). If the serum did not activate the washed platelets in the presence of a therapeutic concentration of UFH or low-molecular-weight heparin, but the control tested positive, then it was defined as negative. The microparticle assay was evaluated against serotonin release assay in the previous article. Overall agreement between the two assays was 96%.17
Since the washed platelet activation assay is demanding and labor intensive,2 and HIT induced by antibodies with platelet-activating properties is exclusively caused by anti-PF4/heparin antibodies of IgG class,18 we first performed the assay for the sample that tested ELISA positive and demonstrated the highest OD in the time-series samples of each patient. If the sample tested negative, we defined the patient as a nonseroconverter in the washed platelet activation assay. If the sample tested positive, then the washed platelet activation assay was performed for all time-series samples.
Seroconversion Rate DifferencesTo clarify the seroconversion rate difference of anti-PF4/heparin IgG in ELISA and HIT antibodies, assessed by washed platelet activation assay, patients were divided based on the trauma severity into mild (ISS 9–15), moderate (ISS 16–24), and severe injury groups (ISS ≥25), according to a previous study.19
In addition, we investigated the influence of heparin administration on seroconversion rates. For this purpose, patients were divided based on the purpose of heparin administration into no heparin (patients did not receive any heparin during the study period), heparin flush (patients only received heparin flushes for catheter patency), and heparin treatment groups (patients received heparin for anticoagulation during invasive treatments including surgery, catheter embolization, and thromboprophylaxis). Only UFH was used for thromboprophylaxis in this study, with no patients receiving low-molecular-weight heparin.
We also analyzed sex and seroconversion rate because sex is also listed as a risk for HIT.
Time to Seroconversion and Subsequent DisappearanceWe investigated the period of time (days) required to achieve seroconversion of anti-PF4/heparin IgG in ELISA or HIT antibodies, detected by the washed platelet activation assay, after the onset of trauma, and the subsequent disappearance rate on day 30. We analyzed only the group that was able to have a blood sampling on the 30th day.
Statistical AnalysisContinuous variables are presented as medians and quartiles, and categorical variables as frequencies and percentages. The Fisher’s exact test was used to compare categorical data among the groups, whereas numerical data were compared using the Kruskal-Wallis test. All p values from paired comparisons were adjusted with the Bonferroni correction for multiple comparisons.
All statistical analyses were performed with EZR statistical software (Saitama Medical Center, Jichi Medical University, Saitama, Japan, available at http://www.jichi.ac.jp/saitama-sct/SaitamaHP.files/statmedEN.html),20 which is a modified version of the R commander (R Foundation for Statistical Computing, Vienna, Austria). A p value of <0.05 indicated statistical significance.
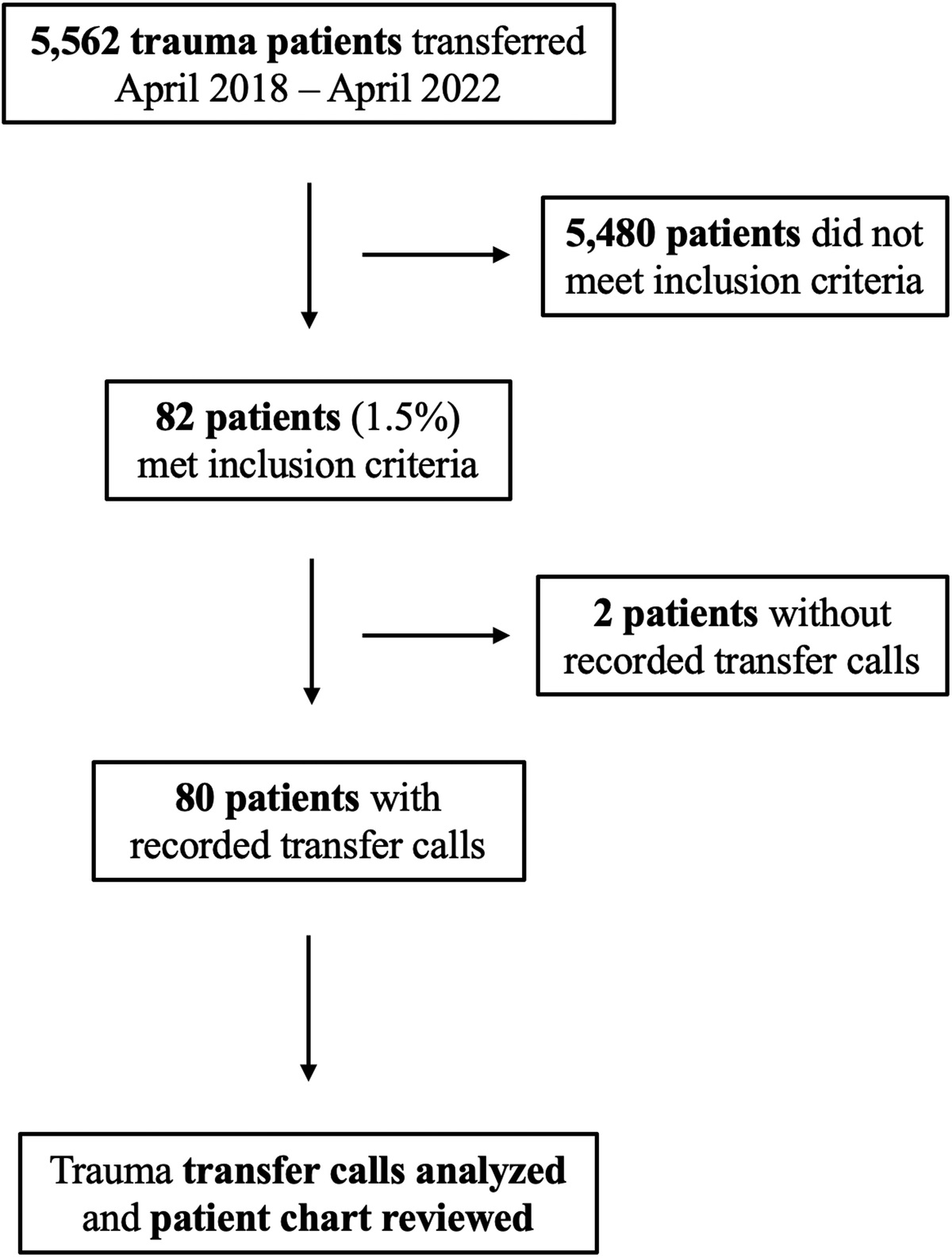
RESULTSA total of 192 patients were initially enrolled in this study. Four patients were excluded because of missing data, three because of burns as the cause of admission, and one whose age was younger than 18 years (Fig. 1).
 Figure 1:
Figure 1: Flow diagram of patient inclusion in this study.
Characteristics of the Study PopulationA total of 184 patients were included in the analyses. Among them, 55, 62, and 67 patients were classified into the mild, moderate, and severe injury groups, respectively (Table 1). Regarding the injured body region, the prevalence of head and neck, and chest injuries increased significantly with increasing trauma severity. The lowest platelet levels tended to decrease with increasing severity of trauma: trauma severity mild group (median, 150 × 109/L), trauma severity moderate group (median, 141 × 109/L), and trauma severity severe group (median, 101 × 109/L).
TABLE 1 - Demographics and Laboratory Data in the Patient Groups Stratified by Trauma Severity Patient Characteristic ISS 9–15 (n = 55) ISS 16–24 (n = 62) ≥25 ISS (n = 67) p Age, y 65 (44–78) 58 (42–74) 64 (47–73) 0.55 Sex (male) 37 (67.3) 43 (69.4) 46 (68.7) 0.98 Mechanism of injury 0.68 Blunt 53 (94.6) 61 (96.8) 64 (92.8) Penetrating 0 0 1 (1.4) Other 3 (5.4) 2 (3.2) 4 (5.8) Injured body region Head and neck 15 (27.3) 33 (53.2) 48 (71.6) <0.001 Face 4 (7.3) 6 (9.7) 10 (14.9) 0.40 Chest 16 (29.1) 29 (46.8) 48 (71.6) <0.001 Abdomen 14 (25.4) 18 (29.0) 19 (28.4) 0.92 Pelvis and extremities 30 (54.5) 29 (46.8) 35 (52.2) 0.69 Skin and soft tissues 14 (25.5) 16 (25.8) 15 (22.4) 0.91 Purpose of heparin administration 0.15 None 18 (32.7) 18 (29.0) 11 (16.4) Flushes 14 (25.5) 21 (33.9) 29 (43.3) Prophylaxis (with or without flushes) 23 (41.8) 23 (37.1) 27 (40.3) Platelet count nadir, ×109/L 150 (111.0–192.0) 141 (98.0–194.5) 101 (70.5–138.5) <0.001 Thrombosis 5 (9.1%) 5 (8.1%) 6 (9.0%) 1.0 In hospital mortality 0 1 (1.6) 3 (4.5) 0.39Numerical data are presented as medians (1st quartile–3rd quartile). Categorical data are presented as number (%).
ELISA, enzyme-linked immunosorbent assay; ISS, Injury Severity Scores; PF4, platelet factor 4.
The overall seroconversion rate of anti-PF4/heparin IgG antibodies evaluated with ELISA was 26.6% (n = 49), and that of HIT antibodies detected with the washed platelet activation assay was 16.3% (n = 30). There was a significant difference in the seroconversion rate among the three trauma severity groups, evaluated with ELISA (p = 0.016) and the washed platelet activation assay (p = 0.046) (Table 2). The seroconversion rate of both ELISA and the washed platelet activation assay was higher with increasing severity, although the proportion of patients who received heparin was not significantly different among the groups (Table 1).
TABLE 2 - Seroconversion Rates of Anti-PF4/Heparin IgG Antibodies and HIT Antibodies in the Patient Groups Stratified by Trauma Severity Anti-PF4/Heparin IgG (ELISA) Mild Injury Group (ISS 9–15)*p < 0.05 compared with mild injury group adjusted with the Bonferroni correction.
ELISA, enzyme-linked immunosorbent assay; ISS, Injury Severity Scores; PF4, platelet factor 4.
The seroconversion rate is significantly different among the three groups divided by the purpose of heparin administration, with the highest rate among the heparin treatment group in both assays (p < 0.001). However, seroconversion was also observed in patients who had not received heparin in both assays (Table 3). Seroconversion rate depending on heparin administration (i.e., no heparin vs. heparin flush vs. heparin treatment) is available in Supplemental Digital Content (Supplementary Table 1, https://links.lww.com/TA/C395).
TABLE 3 - Seroconversion Rates of Anti-PF4/Heparin IgG Antibodies and HIT Antibodies in the Patient Groups Divided by Purpose of Heparin Administration Anti-PF4/Heparin IgG (ELISA) No Heparin*p < 0.001 compared with no-heparin group adjusted with the Bonferroni correction.
ELISA, enzyme-linked immunosorbent assay; ISS, Injury Severity Scores; PF4, platelet factor 4.
Thirty-two (32 of 126) males and 17 (17 of 58) females were ELISA positive, and there was no statistical difference between groups (p = 0.59). The platelet activation assay was positive in 22 (22 of 126) men and 8 (8 of 58) women, with no statistical difference (p = 0.67).
Time to Seroconversion After Trauma and Subsequent DisappearanceTable 4 shows the period required to achieve seroconversion after trauma among the patients who developed anti-PF4/heparin IgG and HIT antibodies in the washed platelet activation assay divided by purpose of heparin administration. There were no significant differences between the three groups based on the purpose of heparin administration (no heparin, heparin flush, and heparin thromboprophylaxis). Most patients developed antibodies between days 5 and 10 of trauma.
TABLE 4 - Period Required to Achieve Seroconversion After the Onset of Trauma and Antibody Disappearance Rate on Day 30 Among the Patients Who Developed Antibodies Divided by Purpose of Heparin Administration Antibodies All Patients Who Developed Antibodies Purpose of Heparin Administration No Heparin Heparin Flush Heparin Prophylaxis p Anti-PF4/heparin IgGs (ELISA) Period required to achieve seroconversion, d 8 (7.0–9.0) 7 (6.5–8.5) 9 (8.0–9.0) 8 (7.0–9.0) 0.45 Disappearance rate of anti-PF4/heparin IgGs on day 30* 10/35 (28.6%) 2/3 (66.7%) 1/8 (12.5%) 7/24 (29.2%) 0.19 HIT antibodies (washed platelet activation assay) Period required to achieve seroconversion, d 8 (7.0–10.5) 6 9 (8–9.5) 8 (7–10.5) 0.22 Disappearance rate of HIT antibodies on day 30* 14/23 (60.9%) 1/1 (100%) 1/5 (20%) 12/17 (70.6%) 0.12*Only patients whose blood samples were available on day 30 were analyzed.
Numerical data are presented as the median (1st quartile–3rd quartile). Categorical data are presented as number (%).
ELISA, enzyme-linked immunosorbent assay; PF4, platelet factor 4.
Table 5 shows the period required to achieve seroconversion after trauma among the patients who developed anti-PF4/heparin IgG and HIT antibodies in the washed platelet activation assay stratified by trauma severity. There were no significant differences between the three groups based on the severity of trauma.
TABLE 5 - Period Required to Achieve Seroconversion After the Onset of Trauma and Antibody Disappearance Rate on Day 30 Among the Patients Who Developed Antibodies Stratified by Trauma Severity Antibodies All Patients Who Developed Antibodies ISS Mild Injury Group (ISS 9–15) Moderate Injury Group (ISS 16–24) Severe Injury Group (≥25 ISS) p Anti-PF4/heparin IgGs (ELISA) Period required to achieve seroconversion, d 8 (7.0–9.0) 8 (8.0–9.0) 8 (7.0–9.0) 8 (7.0–9.0) 0.61 Disappearance rate of anti-PF4/heparin IgGs on day 30* 10/35 (28.6%) 3/5 (60%) 2/11 (18.2%) 5/19 (26.3%) 0.3 HIT antibodies (washed platelet activation assay) Period required to achieve seroconversion, d 8 (7.0–10.5) 8.5 (7.5–9.5) 8 (7.0–9.0) 8.5 (8.0–10.5) 0.68 Disappearance rate of HIT antibodies on day 30* 14/23 (60.9%) 3/4 (75%) 4/7 (57.1%) 7/12 (58.3%) 1.0*Only patients whose blood samples were available on day 30 were analyzed.
Numerical data are presented as the median (1st quartile–3rd quartile). Categorical data are presented as number (%).
ELISA, enzyme-linked immunosorbent assay; ISS, Injury Severity Scores; PF4, platelet factor 4.
In addition, we analyzed the antibody disappearance on day 30. Only patients who achieved seroconversion during the study period were evaluated. As a result, we analyzed 35 patients who developed anti-PF4/heparin IgG antibodies and 23 patients who developed HIT antibodies, detected by the washed platelet activation assay. Overall, anti-PF4/heparin IgG and HIT antibodies were no longer detected on day 30 in 28.6% (n = 10) and 60.9% (n = 14), respectively (Table 4, Table 5).
DISCUSSIONThis study found that trauma severity (assessed by ISS) is associated with the development of HIT antibodies, even among those who did not receive any heparin or only received them as flushes. Heparin administration enhanced the development of antibodies, resulting in the highest seroconversion rate in severely injured patients. Our results also suggest that traumatic injury itself may trigger HIT immune response since the period required to achieve seroconversion after the onset of trauma was not significantly different between patients who received heparin and those who did not.
Heparin-induced thrombocytopenia immune response has several features of an atypical immune-mediated disease. First, heparin-naive patients can develop IgG antibodies as early as day 4, similar to a secondary adaptive immune response.11 Moreover, HIT patients reexposed to heparin following the disappearance of HIT antibodies do not necessarily form HIT antibodies again,15 and HIT antibodies are relatively short-lived unlike those from a secondary adaptive immune response.12 These suggest that a T cell–independent innate immune reaction is involved in the underlying mechanism of HIT antibody formation.8–10 There is an innate immune response to enhance bacterial phagocytosis, producing anti-PF4/polyanion antibodies, which recognize the PF4 bound to polyanions on the bacterial surface, with properties similar to that of HIT antibodies.10 Heparin-induced thrombocytopenia could be a misdirected antibacterial host defense mechanism. In fact, a previous study demonstrated that healthy adults have B cells that produce PF4/heparin-specific antibodies following in vitro stimulation with proinflammatory molecules containing deoxycytosine-deoxyguanosine in their peripheral blood.21 This suggests that healthy individuals have preexisting inactive/tolerant PF4/heparin-specific B cells and that breakdown of the tolerance leads to activation and antibody production in patients developing HIT. Inflammation21–23 and the release of DNA and RNA13 in the blood through tissue destruction and necrosis may cause the breakdown of B cell tolerance in trauma patients, resulting in the rapid and temporal development of HIT antibodies. This would depend on the severity of the trauma, but not on heparin administration. In addition, antibodies induced by such T cell–independent immune reactions decline rapidly,9,21 consistent with our results, which showed that a large proportion of patients, even severely injured ones, who had developed anti-PF4/heparin IgG and HIT antibodies, lost them within 30 days of trauma onset.
In innate immunity, programming of the adaptive immune response where T cells are involved may be caused by activation of professional antigen-presenting cells.8 Anti-PF4/heparin antibody production is suppressed with peripheral immune tolerance. When PF4 reacts with glycosaminoglycans of the T cell surface, the inhibitory effect of regulatory T cells on nonregulatory ones can be suppressed. Thus, while PF4/heparin (or other polyanions) complexes are present, they suppress the inhibitory effect of regulatory T cells and consequently break down peripheral immune tolerance, leading to temporal production of anti-PF4/heparin antibodies.24 If PF4/heparin complexes disappear, peripheral immune tolerance revives and inhibits antibody production.25,26 Since many PF4 can be released by the activation and consumption of platelets in severely injured trauma patients, this may be another mechanism of how anti-PF4/heparin IgG antibodies can develop in this population, even in those who do not receive heparin.
As shown in Table 2, approximately one third of moderately and severely injured patients developed anti-PF4/heparin IgG antibodies, and the proportion of antibodies with platelet-activating properties was higher in severely injured patients. This is despite the fact that the proportion of patients treated with heparin was almost similar (around 40%), independent of trauma severity. These results suggest that severely injured trauma patients are at an increased risk for developing HIT antibodies when they are treated with heparin, consistent with the results of a previous study.14 In that randomized, double-blinded study, all trauma patients received either UFH or low-molecular-weight heparin for more than 5 days for thromboprophylaxis.14 The severity of trauma assessed by AIS was significantly correlated with the seroconversion rates of immunoassay (ELISA) and the washed platelet activation assay (heparin-induced platelet activation test). Trauma patients who underwent major surgery for humeral, hip, femoral, tibial, or pelvic fractures, or extended tissue trauma, exhibited significantly higher seroconversion rates than those who underwent minor surgery. Among trauma patients who underwent major surgery and received UFH for thromboprophylaxis, the combined seroconversion rate of anti-PF4/heparin IgG and HIT antibodies detected by the heparin-induced platelet activation test was around 9%, much lower than the 48% seroconversion rate of our severely injured patients who were treated with heparin. This discrepancy may be attributed to the fact that our study included more severely injured trauma patients, since the AIS of almost all patients in the previous study was 3 or less, and those who required intensive care treatment or therapeutic dose anticoagulants were excluded from the study.
Unexpectedly, some proportion of seroconverted patients, even those severely injured, lost HIT antibodies within 30 days of trauma onset. Therefore, we may consider the possibility of readministering heparin to patients with HIT even within 30 days of trauma onset, if the HIT antibody detected by the washed platelet activation assay is negative.
This study has some limitations. Infections and sepsis have been shown to be at high risk for developing HIT.27 However, data regarding infections were not available for this study, and thus, we were unable to evaluate the influence of infection and sepsis on HIT immune responses in trauma patients. This should be addressed in future studies. In addition, because of our relatively small sample size, we did not perform a multivariate analysis to identify other risk factors for developing HIT antibodies. Therefore, we cannot exclude other confounding factors that may influence anti-PF4/heparin antibody seroconversion. Similarly, we are unable to completely distinguish between the impact of trauma severity and that of heparin administration and to evaluate the relationship between no heparin administration and seroconversion in trauma patients.
Regarding the analysis for the antibody disappearance rate, we included only those whose blood samples were available on day 30, which may have led to selection bias. However, among the patients who developed antibodies, the mean OD value of anti-PF4/heparin IgG antibodies did not significantly differ based on blood sample availability (data not shown).
CONCLUSIONOur results demonstrated that seroconversion of HIT antibodies was observed commonly in trauma patients, and up to one third of severely injured trauma patients develop HIT antibodies with platelet-activating properties when they are treated with heparin. Heparin-induced thrombocytopenia antibody development may be related to trauma severity, with high disappearance rate on day 30. We should consider HIT as a differential diagnosis in patients who develop thrombocytopenia and unexpected thromboembolism between days 5 and 10 after the onset of trauma, irrespective of heparin administration. Our findings provide deep insights for understanding the HIT immune reactions in trauma patients, which may lead to the appropriate diagnosis and treatment of these patients.
AUTHORSHIPM.F., T.M., S.M., and S.K. participated in the study design, analyzed the data, and drafted the manuscript. A.S. participated in the study design and drafted the manuscript. M.F. assessed patient clinical data. T.M. and S.M. performed the serological assays. A.M., M.H., N.M., N.U., T.O., S.I., K.S., Y.F., K.K., and T.H. drafted the manuscript. All authors read and approved the final version of the manuscript. S.K. is the principal investigator and takes primary responsibility for the manuscript.
ACKNOWLEDGMENTSWe thank all the investigators who contributed to this multicenter prospective cohort study, in addition to Eri Sugimori, Kazuyoshi Nakai, Shu Seguchi, and Isami Kakutani at the National Cerebral and Cardiovascular Center for their technical assistance.
This research was supported in part by the General Insurance Association of Japan, Japanese Society of Cardiovascular Anesthesiologist Grant-in-Aid for Young Researchers, a Health and Labor Sciences Research Grant from the Ministry of Health, Labor and Welfare of Japan, the Intramural Research Fund (27-1-2) for Cardiovascular Disease of the National Cerebral and Cardiovascular Center, a grant from SENSHIN Medical Research Foundation, and a grant-in-aid from the Takeda Science Foundation.
DISCLOSURES.M. received research support from Daiichi Sankyo Co., Ltd. (Tokyo, Japan) and Mitsubishi Tanabe Pharma Corporation (Osaka, Japan) and is currently working at Central Blood Institute, Blood Service Headquarters, Japanese Red Cross Society. The remaining authors have disclosed that they do not have any conflicts of interest.
REFERENCES 1. Greinacher A. Clinical practice. Heparin-induced thrombocytopenia. N Engl J Med. 2015;373(3):252–261. 2. Maeda T, Nakagawa K, Murata K, Kanaumi Y, Seguchi S, Kawamura S, et al. Identifying patients at high risk of heparin-induced thrombocytopenia-associated thrombosis with a platelet activation assay using flow cytometry. Thromb Haemost. 2017;117(1):127–138. 3. Warkentin TE, Sheppard JA, Moore JC, Cook RJ, Kelton JG. Studies of the immune response in heparin-induced thrombocytopenia. Blood. 2009;113(20):4963–4969. 4. Hughes M, Hayward CP, Warkentin TE, Horsewood P, Chorneyko KA, Kelton JG. Morphological analysis of microparticle generation in heparin-induced thrombocytopenia. Blood. 2000;96(1):188–194. 5. Rauova L, Hirsch JD, Greene TK, Zhai L, Hayes VM, Kowalska MA, et al. Monocyte-bound PF4 in the pathogenesis of heparin-induced thrombocytopenia. Blood. 2010;116(23):5021–5031. 6. Padmanabhan A, Jones CG, Bougie DW, Curtis BR, McFarland JG, Wang D, et al. Heparin-independent, PF4-dependent binding of HIT antibodies to platelets: implications for HIT pathogenesis. Blood. 2015;125(1):155–161. 7. Visentin GP, Ford SE, Scott JP, Aster RH. Antibodies from patients with heparin-induced thrombocytopenia/thrombosis are specific for platelet factor 4 complexed with heparin or bound to endothelial cells. J Clin Investig. 1994;93(1):81–88. 8. Khandelwal S, Arepally GM. Immune pathogenesis of heparin-induced thrombocytopenia. Thromb Haemost. 2016;116(5):792–798. 9. Zheng Y, Yu M, Podd A, Yuan L, Newman DK, Wen R, et al. Critical role for mouse marginal zone B cells in PF4/heparin antibody production. Blood. 2013;121(17):3484–3492. 10. Krauel K, Potschke C, Weber C, Kessler W, Furll B, Ittermann T, et al. Platelet factor 4 binds to bacteria-inducing antibodies cross-reacting with the major antigen in heparin-induced thrombocytopenia. Blood. 2011;117(4):1370–1378. 11. Greinacher A, Kohlmann T, Strobel U, Sheppard JA, Warkentin TE. The temporal profile of the anti-PF4/heparin immune response. Blood. 2009;113(20):4970–4976. 12. Warkentin TE, Kelton JG. Temporal aspects of heparin-induced thrombocytopenia. N Engl J Med. 2001;344(17):1286–1292. 13. Jaax ME, Krauel K, Marschall T, Brandt S, Gansler J, Furll B, et al. Complex formation with nucleic acids and aptamers alters the antigenic properties of platelet factor 4. Blood. 2013;122(2):272–281. 14. Lubenow N, Hinz P, Thomaschewski S, Lietz T, Vogler M, Ladwig A, et al. The severity of trauma determines the immune response to PF4/heparin and the frequency of heparin-induced thrombocytopenia. Blood. 2010;115(9):1797–1803. 15. Warkentin TE, Sheppard JA. Serological investigation of patients with a previous history of heparin-induced thrombocytopenia who are reexposed to heparin. Blood. 2014;123(16):2485–2493. 16. Maeda T, Noguchi T, Saito S, Yoshioka R, Horibe E, Miyanaga S, et al. Impact of heparin-induced thrombocytopenia on acute coronary artery thrombosis in patients undergoing PCI. Thromb Haemost. 2014;112(3):624–626. 17. Lee DH, Warkentin TE, Denomme GA, Hayward CP, Kelton JG. A diagnostic test for heparin-induced thrombocytopenia: detection of platelet microparticles using flow cytometry. Br J Haematol. 1996;95(4):724–731. 18. Warkentin TE, Arnold DM, Nazi I, Kelton JG. The platelet serotonin-release assay. Am J Hematol. 2015;90(6):564–572. 19. Palmer CS, Gabbe BJ, Cameron PA. Defining major trauma using the 2008 Abbreviated Injury Scale. Injury. 2016;47(1):109–115. 20. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. 21. Zheng Y, Wang AW, Yu M, Padmanabhan A, Tourdot BE, Newman DK, et al. B-cell tolerance regulates production of antibodies causing heparin-induced thrombocytopenia. Blood. 2014;123(6):931–934. 22. Bito S, Miyata S, Migita K, Nakamura M, Shinohara K, Sato T, et al. Mechanical prophylaxis is a heparin-independent risk for anti-platelet factor 4/heparin antibody formation after orthopedic surgery. Blood. 2016;127(8):1036–1043. 23. Paparella D, Scrascia G, Galeone A, Coviello M, Cappabianca G, Venneri MT, et al. Formation of anti-platelet factor 4/heparin antibodies after cardiac surgery: influence of perioperative platelet activation, the inflammatory response, and histocompatibility leukocyte ant
留言 (0)