
記住我
The study was approved by the ethics committee of the Medical Association of North Rhine in Germany (id. no. 82/2021), and individual patient consent for the study was waived. The study was performed in accordance with the Declaration of Helsinki 1964 and its later amendments.
Study Design and Data SourceThis is a retrospective study, and all perioperative data were prospectively collected from the clinic's internal databases. All patients with isolated aortic valve stenosis, insufficiency, and/or endocarditis who underwent MIC-AVR were included in this study. Exclusion criteria were reoperation, aortic valve reconstruction, and need for additional cardiosurgical procedure.
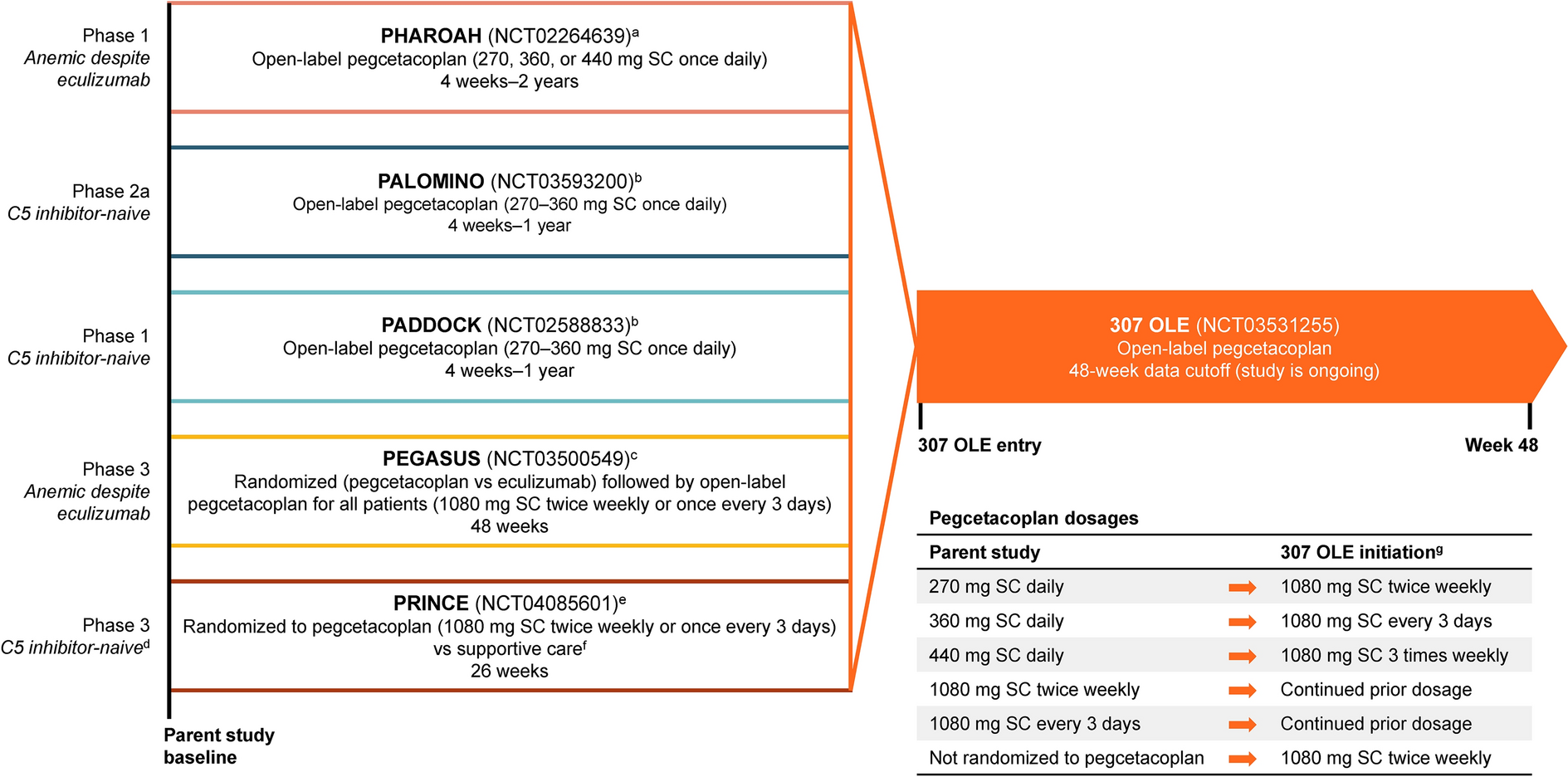
Between March 2015 and February 2021, 768 patients underwent MIC-AVR at our institution. Of those, 63 patients (42 in the RAMT group and 21 in the PUS group) underwent AKE in combination with Morrow resection. Aortic valve reconstruction was performed in seven patients in the PUS group, and four additional patients in the PUS group were excluded from the study because of previous AKE. After application of the inclusion and exclusion criteria, final data from 694 patients were used for statistical analysis. Of these, 441 (63.5%) patients were operated on using RAMT and 253 (36.5%) patients via PUS. After propensity score analysis, 202 matched patients from the RAMT group and 202 from the PUS group were evaluated (Fig. 1).
Fig. 1
Patient flow chart. PS, propensity score; PUS, partial upper sternotomy; RAMT, right anterior mini-thoracotomy
At the start of the study, PUS was the standard surgical access for isolated AVR surgery in our department. Since March 2017, RAMT has become the first-line strategy for the surgical treatment of all isolated aortic valve pathologies (Supplementary Material). During this period of study, preoperative computer tomography (CT) of the aorta was performed in all patients who required an isolated AVR to determine whether the patient was suitable for the RAMT procedure [18]. In cases of severe calcification of the aorta or pelvic arteries, severe anatomical conditions, or strong adhesions of the lungs, PUS serves as an alternative surgical access benefiting from considerable advantages of the MIC techniques [9, 13,14,15].
The primary endpoint was 30-day mortality. Secondary endpoints were cardiopulmonary bypass (CPB) time and aortic clamping time, conversion to MS, surgical revision, postoperative respiratory failure, hemodialysis, wound healing disorders, length of intensive care and hospital stay, and estimated survival at 4 years.
Follow-UpDischarged patients were assessed directly in our outpatient clinic after 3 months and yearly thereafter or were contacted by mail or telephone interview during a 3-month late closing interval ending in April 2021 with completion of 98%. Telephone contact with the patients was used to assess the current physical condition and to request further cardiovascular interventions and check-ups by the referring cardiologists and family doctors, who were also contacted if additional information was needed.
Operative TechniqueAll patients were intubated with a single-lumen endotracheal tube, and transesophageal echocardiography (TEE) was performed in all patients for monitoring heart and valve function during the operation.
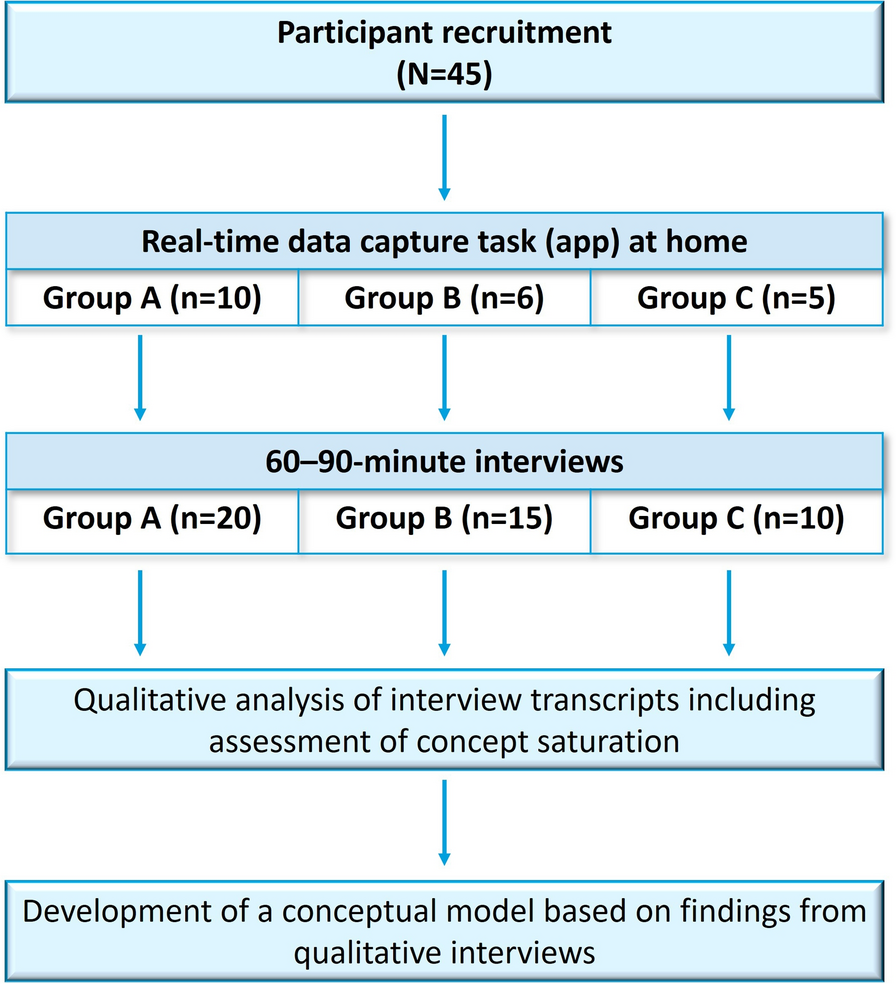
A detailed description of the PUS technique has been published previously [9]. The surgical access was performed through a 5–6-cm skin incision followed by J-shaped upper mini-sternotomy at the fourth intercostal space. A central cannulation for CPB through the ascending aorta and right atrium was preferred by most of this patient group (Fig. 2).
Fig. 2
Operative site of an aortic valve replacement via the partial superior sternotomy. A For subanular insertion of Ethibon 2–0 U-sutures. B Inserting the U-sutures into the Magna Ease® aortic valve prosthesis. C After closure of the aorta. D Immediately after wound closure. This figure was created entirely by the authors for this article, has never been published before, and was not based in whole or in part on a previously published figure
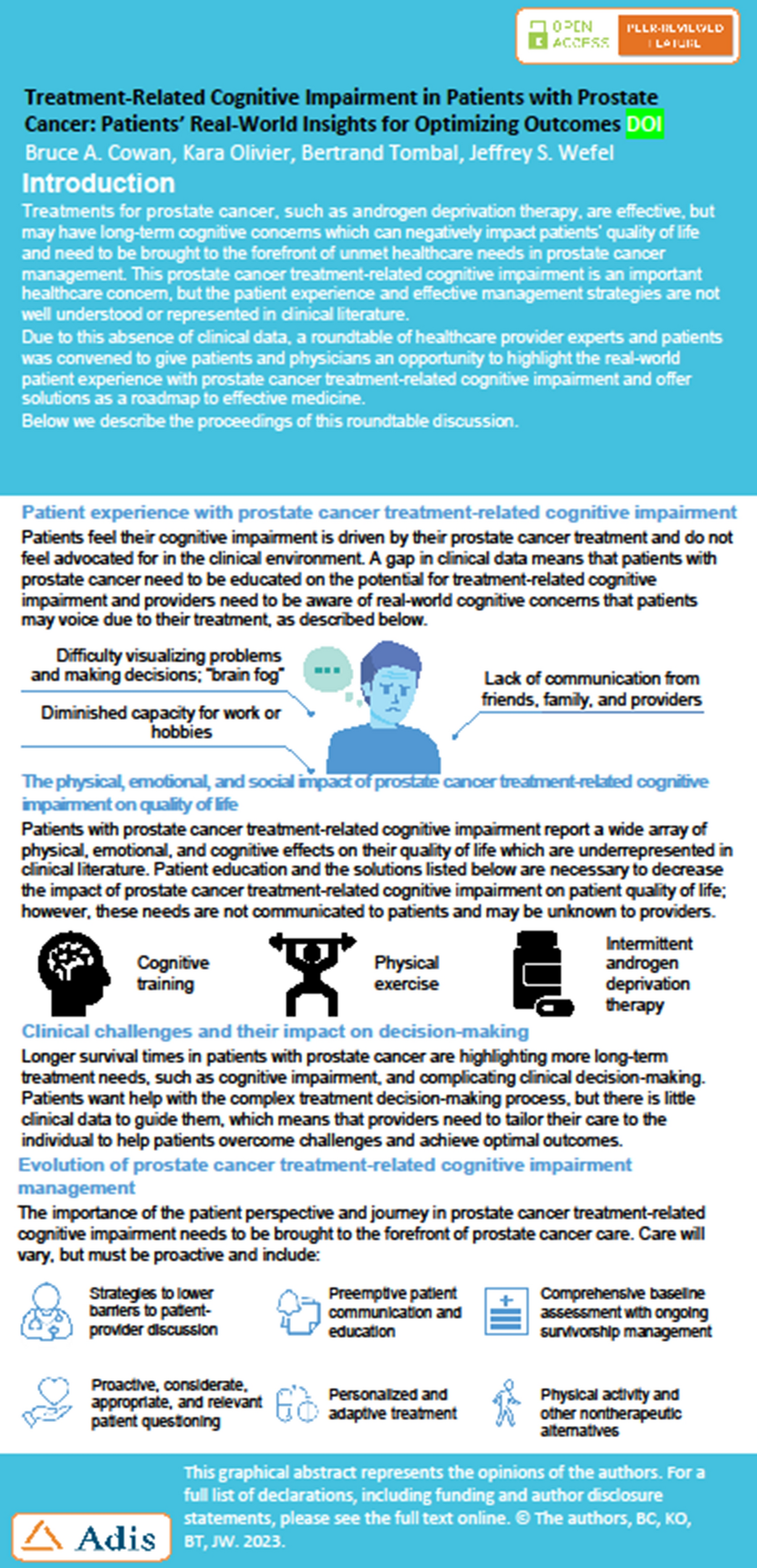
For the RAMT group, the access was performed through a 3–5-cm skin incision at the second or third right intercostal space. A detailed description of the surgical technique has been published previously [3]. Cannulation for CPB was achieved through the common femoral artery in 436 (98.7%) patients and the common femoral vein in all patients in the unmatched cohort. Additional cannulation of the jugular vein was necessary in 102 (23.1%) patients. Femoral cannulation was performed primarily surgically through a 2-cm skin incision below the inguinal ligament. Since January 2019, percutaneous femoral cannulation for CPB guided by ultrasound sonography was performed in combination with the use of a vascular closure device (VCD) MANTA™ (Essential Medical Inc., Malvern, PA, USA) for femoral artery closure. Except for the automated suturing with Cor-Knot® (Cor-Knot®, LSI Solutions, USA), there is no difference between AVR using RAMT and the traditional sternotomy approach (Fig. 3).
Fig. 3
Operative setup of an aortic valve replacement via right anterior mini-thoracotomy. A Before implanting an Inspiris Resilia® aortic valve. B By implanting the aortic valve prosthesis. C Introduction of Cor-Knot® to fix the aortic valve prosthesis. D Femoral artery occlusion with MANTA® System. E Immediately after wound closure. This figure was created entirely by the authors for this article, has never been published before, and was not based in whole or in part on a previously published figure
Statistical AnalysisPropensity score matching was performed. The propensity score for each patient was calculated by logistic regression with adjustment for 12 key baseline variables: age, gender, body mass index (BMI), New York Heart Association score (NYHA) ≥ 3, hypertension, diabetes mellitus, prior stroke, acute endocarditis, urgent indication for surgery, left ventricular ejection fraction (LVEF), aortic valve stenosis, and European System for Cardiac Operative Risk Evaluation II (EuroSCORE II). When matching patients 1:1, a difference in propensity score of 0.7% (0.007) was tolerated.
Data on the matched and unmatched groups were analyzed using descriptive statistics, with categorical variables presented as absolute values and frequencies (%) and the continuous variables presented as the median and interquartile range (IQR) or mean ± standard deviation (SD). Comparisons between the RAMT and PUS groups were carried out using a t-test or Mann-Whitney U test for continuous variables as appropriate depending on distribution and a Fisher's exact or chi-square test for categorical variables. To test for normal distribution of the continuous variables, the Kolmogorov-Smirnov test was used. Cohen's d was used for the continuous variables with significant difference. A Cohen’s d value of > 0.8 indicates a major effect. Survival analyses were presented as Kaplan-Meier curves. In addition, hazard ratios (HRs) were calculated by Cox regression. In all cases, a two-tailed p value of < 0.05 was considered statistically significant. All statistical tests were performed using IBM SPSS Statistics software version 24.0 (IBM Corp., Armonk, NY, USA).
留言 (0)