
記住我



The 2030 Agenda for Sustainable Development aims at ending the AIDS epidemic by 2030 [1]. Despite progress in recent years, HIV/AIDS continue to be leading causes of death and disability, with more than 850 000 deaths worldwide mostly occurring in sub-Saharan Africa (SSA) [2,3]. Indeed, more than two-thirds of people infected with HIV are living in SSA [3].
Industrial mines have long been identified as potential hotspots for HIV transmission [4,5]. The opening of industrial mining projects can trigger multiple changes in local communities that are conducive to increased HIV infection risk, including in-migration of job seekers from areas with high HIV prevalence [6,7], a larger share of the (migrant) population living separately from their partners [8], a generally low level of risk aversion with respect to contracting HIV among populations exposed to substantial occupational risks [8,9], and a high propensity to engage in prostitution, extramarital relationships, and other risky sexual practices [6–13].
The large undeveloped mineral deposits in SSA have resulted in rapid growth in the mining sector in the region, raising major concerns regarding potential new increases in HIV transmission [14]. Most available studies on HIV in mining settings solely focus on specific population groups. For example, migrant miners from Mozambique were found to have a higher HIV prevalence than the general population [12]. Case studies found that miners have higher HIV prevalence in Lesotho and Eswatini, lower in Tanzania, whereas in Zambia and Zimbabwe, only minor differences were found [6,11,15]. Contrarily, higher mortality rates of HIV were found among male miners in Tanzania compared with other community members [16]. Conversely, sexually transmitted diseases, including HIV/AIDS, were less frequently reported in metal extraction areas [17]. Finally, HIV incidence near a coal mine in South Africa decreased slightly after opening but increased sharply 5 years after opening [18].
In summary, although it has been commonly assumed in the extant literature that HIV transmission is higher in mining communities [4,5], causal evidence on mining impacts on HIV remains fragmented and inconclusive, and longitudinal studies on HIV transmission remain scarce [19]. In this article, we study the impact of 39 newly opened large industrial mining projects on HIV prevalence, HIV knowledge, and risky sexual practices using data from 16 SSA countries.
Methods Study designThis study used a quasi-experimental study design assessing the impact of newly opened mines on HIV prevalence and risk factors. Pseudo-panels around mines were created using regionally representative data from repeated cross-sectional household surveys.
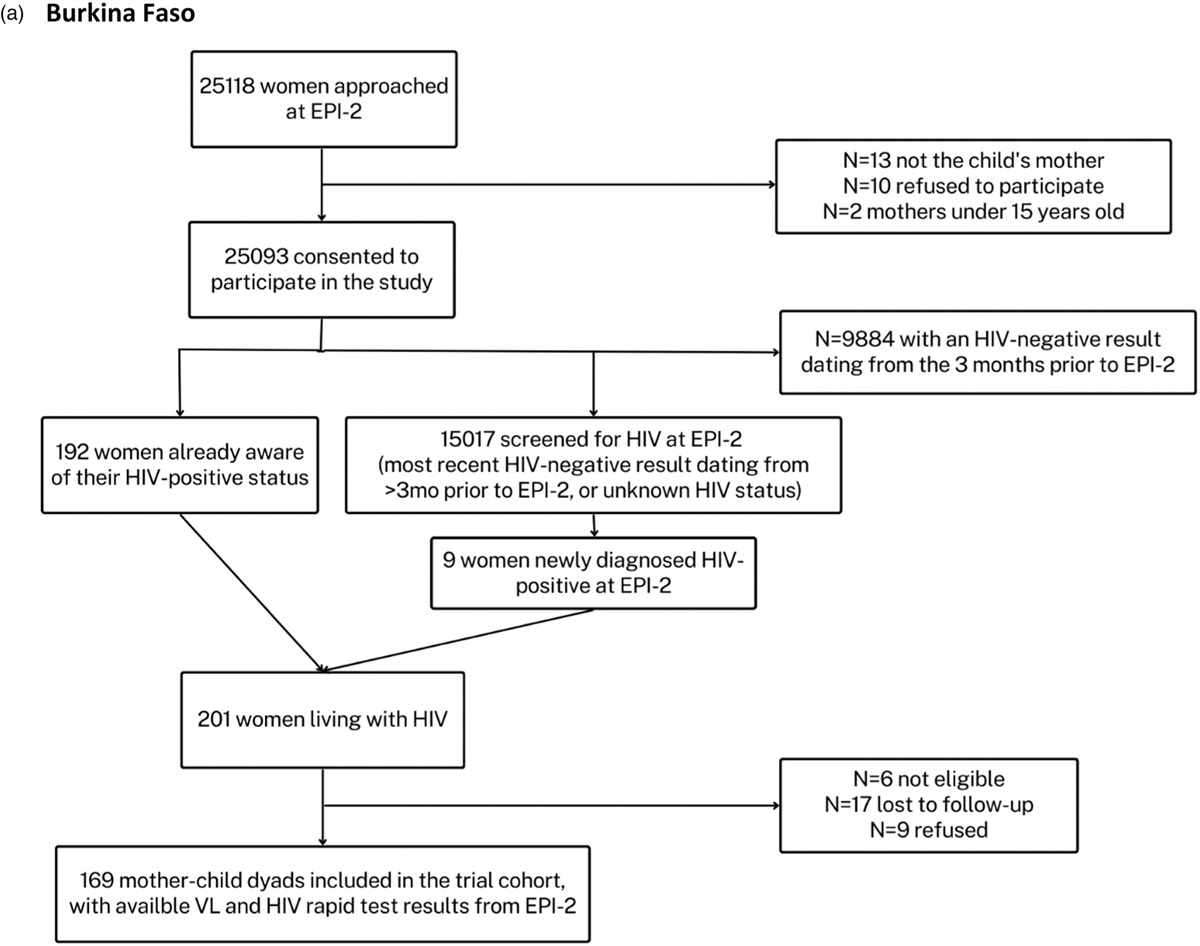
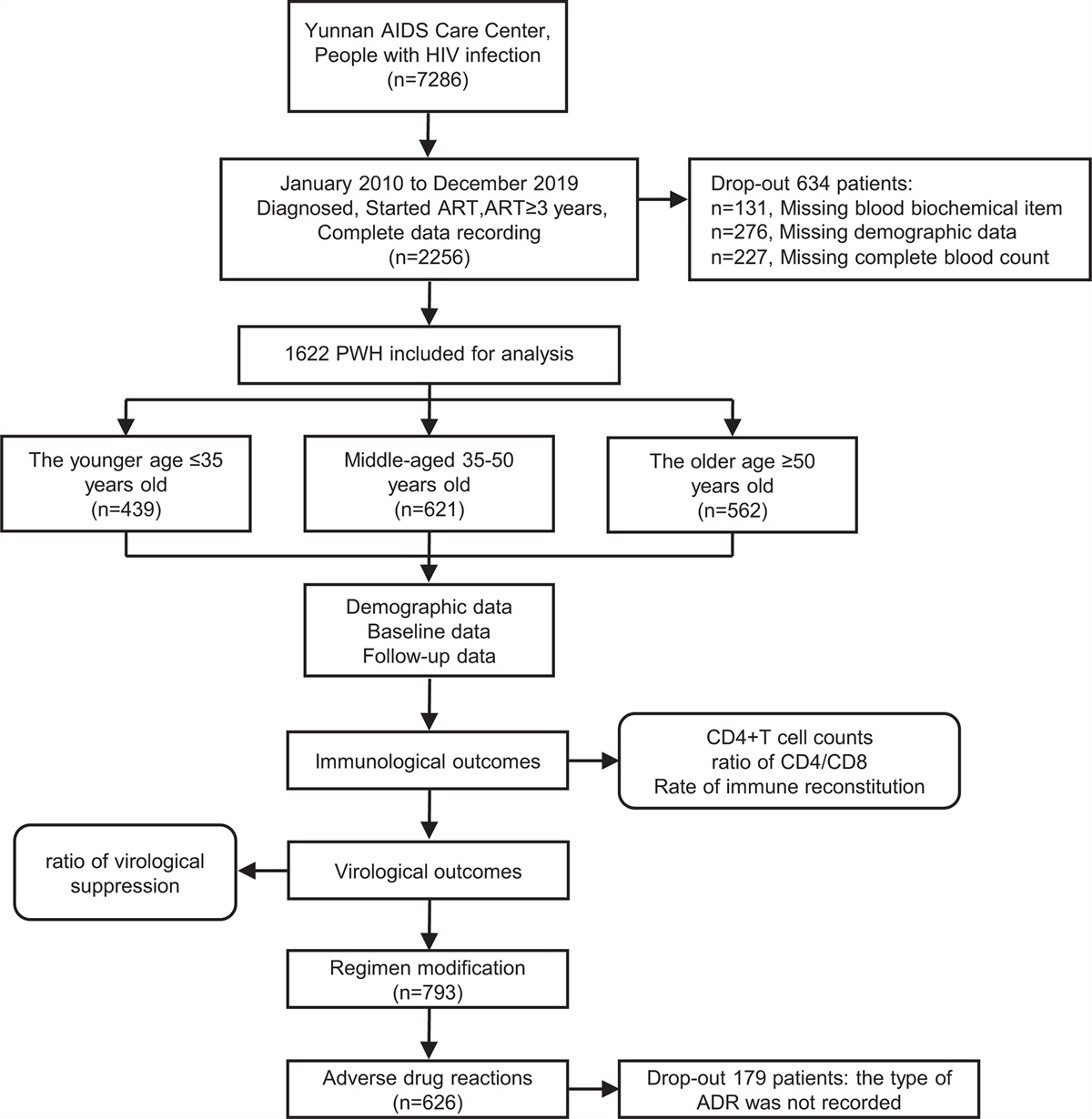
Data Demographic and Health SurveysThe Demographic and Health Survey (DHS) program provides georeferenced household and individual-level data that include HIV testing results from 31 countries in SSA. In these surveys, household members aged 15–49 years are invited for HIV testing. Along the data on individual and household characteristics, the location of the survey cluster is provided. To protect the confidentiality of the respondents, the locations of the clusters are offset by a random distance up to 2 km for urban clusters and up to 10 km for rural clusters [20]. DHS data are freely accessible upon request from the DHS website [20]. For this study, all DHS data that constituted a HIV module were initially included (Fig. 1).
 Fig. 1:
Fig. 1: Flow chart showing the selection of Demographic and Health Surveys data around mining sites.
In larger cities, various external effects other than the implementation of a mining project can influence HIV status. Therefore, observations from within the boundaries of cities with more than 100 000 inhabitants were removed from the DHS dataset following the methodology described in Dietler et al.[21].
Mining dataInformation about the location, type, and operational status of large industrial mining projects in SSA was retrieved from the Standard&Poor's Global Market Intelligence dashboard on 8 February 2021. From the complete list, mines were included if they met the following criteria: information on production and extraction activities between 1980 and 2020 available; opened after 2003 (earliest year of available DHS data); located at least 20 km from another recently opened mine to avoid external effects from openings of other nearby mines; and DHS data available from both, the premining phase and after mine opening. The accuracy of the mining information was verified for a sub-sample of mines that were part of a larger research initiative [22].
Sample selectionFig. 1 illustrates the process for creating the final analytical data file. For each included mine, DHS data from the different survey rounds within a 50 km radius were selected using ArcGIS pro (Version 2.2.4; ESRI, Redlands, California, USA). Table A1, https://links.lww.com/QAD/C556 in the supplementary files shows basic properties of the included mines while more detailed information on the included DHS datasets are provided in Table A2, https://links.lww.com/QAD/C556.
Of the 356 mines that opened in SSA since 2003, 188 were in an isolated location. Of those, 39 had DHS data available both from the premining phase and after the start of operations (Fig. 2). The final dataset consisted of 33 086 individuals from 16 countries: Burkina Faso, Burundi, Côte d’Ivoire, Democratic Republic of the Congo, Ghana, Guinea, Kenya, Liberia, Mali, Mozambique, Rwanda, Sierra Leone, Tanzania, Togo, Zambia and Zimbabwe. The included mines opened between 2007 and 2018 (Table A1, https://links.lww.com/QAD/C556).
 Fig. 2:
Fig. 2: Left: location of industrial mines and study countries included in the final dataset. Right: visualization of mining and comparison areas around a selected mine. Source basemap: Esri, Maxar, GeoEye, Earthstar Geographics, CNES/Airbus DS, USDA, USGS, AeroGRID, IGN, and the GIS User Community.
Variables Exposure variableThe exposure variable was the opening of a new industrial mine. Households located within 10 km from the mines were considered as exposed to mines (Fig. 2). Households located between 10 and 50 km were used as the spatial comparison group. Previous literature suggests that the direct influence of mines on communities outside of a 10 km radius is limited [23,24]. Three mining phases were distinguished in our empirical analysis: premining phase (>3 years before start of extraction), construction phase (1–3 years before start of extraction), and operational phase (between start of extraction and closure). During the construction phase, mining communities are characterized by a large proportion of migrants [5]. Their potentially different health profile could be a source of bias for the estimation of community-level impacts. Therefore, data from this time period were excluded from analyses. The length of the construction phase was based on mining literature [25–27].
Outcome variablesOur primary study outcome was individuals’ HIV status. The DHS determines HIV status through laboratory testing using capillary blood from a finger prick. Individuals without a valid test result or age information were considered as missing.
For the indicators on HIV-related risk factors, the individual responses to the DHS questionnaires were used. The questions included for the creation of these indicators are listed in the supplementary files. To be considered as having comprehensive HIV knowledge, respondents needed to know that using condoms and having only one uninfected faithful partner are the two primary methods for preventing HIV infections, know that HIV positive people can look healthy, and reject two of the most common misconceptions (HIV can be transmitted through mosquito bites, supernatural means, or by sharing food). People responding ‘don’t know’ or with missing values were considered to lack knowledge. Similarly, respondents who had never heard of HIV/AIDS were considered not to know about the preventive measures.
Three additional outcome variables were used to assess changes in risky sexual behaviors. First, whether a respondent had multiple sexual partners within the 12 months prior to the survey. If the respondent did not remember the time since last intercourse it was assumed to be more than 12 months ago. Second, high-risk sexual partnerships in the 12 months preceding the survey is a sexual relationship with a person that is not the spouse or living with the respondent was considered as a high-risk partnership. The third indicator was lack of condom use in a high-risk sexual partnership in the last 12 months.
CovariatesSeveral covariates were considered for adjustment for underlying differences in the study population at varying distances to the mines and over time. Sex was used as a dichotomous term (man/woman). Categories for the highest attained educational level included no education, primary school, secondary school, and higher education. Household wealth was categorized in the DHS data into quintiles based on household possessions [28]. Employment in the last 12 months was included as dichotomous variable. Residency was defined as either urban or rural. Finally, an indicator combining marital status and polygyny was created with categories including not in consensual union (single, divorced, or widowed), monogamous relationship, and polygenic relationship.
Statistical analysesA difference-in-differences approach was applied using the interaction term between living close (less than 10 km) to a new mine and active mining (operational phase) to identify the causal effect of mine openings. Changes in HIV indicators close to the mine were compared with changes in surrounding areas at 10–50 km distance. In this difference-in-difference approach, if mine openings had no impact on HIV prevalence and changes in HIV-related risk factors and assuming that the likelihood of a mine opening is not correlated with other factors affecting these outcomes, parallel trends between mining and comparison areas would be expected [29]. Hence, a positive beta-coefficient for the interaction between proximity to the mine and mines being active suggests that the initiation of mining resulted in increases in the outcomes.
For each outcome variable, logistic regression models with different adjustment sets were used. To account for the pseudo-panel structure of the data, a mine-level fixed effect was used in all models. Potential covariates and mediators were selected a priori based on previous literature [6,29]. Both, factors that are not a result of the mine openings as well as factors that can directly or indirectly be impacted by the mine (e.g. employment or wealth) were considered. Variables with a P value below 0.2 in the univariate analyses with HIV status were included in the final adjustment sets. All considered covariates fulfilled this inclusion criterion. The basic adjustment set was age in years (including second order term), sex, survey year, residency, educational level, employment and household wealth quintiles. The model for HIV status and comprehensive knowledge about HIV additionally included the type of relationship as covariate. To explore potential effects of HIV prevalence on HIV knowledge and risky sexual practices, separate models were used for these outcomes adjusting for HIV status.
Stratified analyses for sex, age group, and country-level HIV prevalence were conducted. Countries were classified as high-prevalence if the HIV prevalence in 2011 (median DHS survey year) exceeded 3% (obtained from [30]). The P values for the comparison baseline characteristics were derived using Pearson's chi-squared for categorical variables and Wilcoxon rank-sum test for age. Analyses were performed in R version 3.5.1 (The R Foundation; Vienna, Austria) and Stata version 16.0 (Stata Corporation; College Station, Texas, USA).
ResultsTable 1 outlines descriptive statistics for treatment and control areas. There were no statistically significant differences between the study areas in the premining phase among the outcome variables. However, in the premining phase, respondents in the mining areas were on average older (median age 29 vs. 28; P = 0.019), had a lower education level (P < 0.001), and were more often living in a polygenic relationship and less frequently single (P < 0.001).
Table 1 - Descriptive statistics of study population stratified by distance to mine and mining phase Mining phase Premining phase (4+ years before mine opening) Operational phase (after mine opening) Distance to mine Comparison area (10–50 km) Mining area (0–10 km) P value∗ Comparison area (10–50 km) Mining area (0–10 km) P value∗ N 15 089 594 16 635 768 HIV-positive 947 (6.7%) 34 (5.8%) 0.39 963 (6.0%) 52 (7.3%) 0.14 Comprehensive knowledge 7621 (56.2%) 309 (57.1%) 0.67 8906 (57.0%) 404 (58.0%) 0.61 Multiple sex partners 871 (7.6%) 33 (6.7%) 0.44 1164 (8.9%) 69 (11.2%) 0.049 High-risk sexual partners 2023 (21.0%) 72 (17.3%) 0.072 2531 (22.5%) 140 (25.5%) 0.096 No condom at high-risk sex 1188 (12.3%) 46 (11.1%) 0.44 1382 (12.3%) 98 (17.9%) <0.001 Female 8087 (53.6%) 328 (55.2%) 0.44 9023 (54.2%) 398 (51.8%) 0.19 Age, median (IQR) 27 (20, 37) 29 (21, 38) 0.019 28 (20, 38) 28 (21, 37) 0.85 Highest level of education <0.001 0.002 No education 4242 (29.5%) 251 (43.1%) 4712 (29.1%) 188 (25.8%) Primary 4516 (31.4%) 159 (27.3%) 4226 (26.1%) 183 (25.1%) Secondary 5161 (35.9%) 156 (26.8%) 6562 (40.6%) 340 (46.7%) Higher 459 (3.2%) 17 (2.9%) 665 (4.1%) 17 (2.3%) Type of relationship <0.001 0.87 Single, divorced, widowed 5610 (40.2%) 186 (31.9%) 6292 (38.9%) 286 (39.3%) Monogamous relationship 6669 (47.8%) 274 (47.0%) 7759 (48.0%) 343 (47.1%) Polygenic relationship 1684 (12.1%) 123 (21.1%) 2114 (13.1%) 99 (13.6%) Rural 10 469 (69.4%) 399 (67.2%) 0.25 11 115 (66.8%) 438 (57.0%) <0.001Data obtained from Demographic and Health Survey (DHS) datasets near 39 industrial mines in 16 sub-Saharan African countries. IQR, interquartile range; percentages indicate proportion of nonmissing observations.
∗P values derived using Pearson's chi-squared (categorical variables) or Wilcoxon rank-sum test (age).
HIV prevalence increased from 6% in the premining phase to 7.3% in the operational phase, while it decreased from 6.7 to 5.8% in the comparison areas (Table 1). The percentage of people with comprehensive knowledge about HIV increased slightly over time to a similar extent in mining and comparison areas. All risky sexual behaviors become disproportionally more frequent in mining areas compared with the areas located further away.
The same results were found in the logistic regression models (Table 2). When accounting for baseline differences and general trends in HIV rates, mine openings roughly doubled the odds of being HIV-positive [crude OR: 1.93, 95% CI: 1.19–3.14; adjusted OR (aOR): 2.14, 95% CI: 1.29–3.55].
Table 2 - Estimates of the impact of mine openings on HIV status, HIV knowledge, and risky sexual behaviors Outcome Crude modelaOR (95% CI) Adjusted modelbOR (95% CI) Adjusted modelb (incl. HIV status)OR (95% CI) HIV-positive 1.93 (1.19–3.14)∗ 2.14 (1.29–3.55)∗ n.a. Comprehensive knowledge 0.81 (0.63–1.04) 0.76 (0.59–0.99)∗ 0.76 (0.59–0.99)∗ Multiple sex partners 1.61 (1.02–2.55)∗ 1.64 (1.01–2.67)∗ 1.72 (1.06–2.82)∗ High-risk sexual partners 1.45 (1.03–2.05)∗ 1.20 (0.80–1.80) 1.26 (0.84–1.91) No condom at high-risk sex 1.77 (1.18–2.67)∗ 1.55 (0.99–2.43) 1.68 (1.07–2.66)∗The crude and adjusted odds ratio (OR) quantify the interaction effect of proximity to a mine (<10 vs. 10–50 km) and mining activity (operational vs. premining phase). OR and corresponding 95% confidence intervals (95% CI) were derived using logistic regression models. CI, confidence interval; n.a., not applicable; OR, odds ratio.
aMine-level fixed effect only.
bAdjusted for age (incl. second order term), sex, survey year, residency (urban/rural), educational level, wealth quintile, and employment during the prior 12 months. Models for HIV status and HIV knowledge additionally adjusted for type of relationship.
∗P less than 0.05, statistically significant.
In the crude analyses, a tendency towards reduced HIV knowledge was found (OR: 0.81, 95% CI: 0.63–1.04). Whenever adjusting for potential confounders and mediators, the effect was also statistically significant (aOR: 0.76, 95% CI: 0.59–0.98). Further adjustment to check whether the increased HIV prevalence in mining areas influences these associations did not substantially affect the results.
Risky sexual practices became more frequent with mine openings. The crude OR for having multiple sex partners, having sexual intercourse with high-risk sexual partners, and abstaining from condoms during high-risk sex were 1.61 (95% CI: 1.02–2.55), 1.45 (95% CI: 1.03–2.05) and 1.77 (95% CI: 1.18–2.67), respectively. After adjustment for potential confounders, there was still a tendency towards more risky sexual behaviors in mining areas, although some associations were not statistically significant anymore. The point estimates for these associations increased when additionally adjusting for HIV status.
Stratified analyses revealed geographical differences in the impact of mine openings on HIV prevalence (Fig. 3). Largest impacts on HIV infection risk were seen in countries with an overall high HIV prevalence (i.e. >3% among the adult population) with an estimated OR of 2.26 (95% CI: 1.32–3.45). No impact was found in low-prevalence countries (OR: 1.01, 95% CI: 0.30–3.42). Further analysis among population sub-groups showed that there were no substantial differences in the impact on men and women with regards to HIV infections. In contrast, substantial differences in the effect size between age groups were found (Fig. 3). The strongest impact was seen among people aged between 20 and 29 years (OR: 3.50, 95% CI: 1.50–8.16).
 Fig. 3:
Fig. 3: Stratified analyses for the impact of mine openings on HIV status, HIV knowledge, and risky sexual behaviors. The crude odds ratio for the interaction effect of proximity to a mine (<10 vs. 10–50 km) and mining activity (operational vs. premining phase) together with their 95% confidence intervals are shown on the log-scale. Results are stratified for country HIV prevalence, sex, and age group.
The same age group also showed the most substantial reductions in HIV-related knowledge. The strongest negative effects of mine opening on HIV knowledge were seen among the age groups between 20 and 39 years (Fig. 3). No effects were seen among the other age groups. Furthermore, particularly the male population in mining areas had decreased knowledge about HIV (OR: 0.70, 95% CI: 0.48–1.02).
Sexually risky behaviors become particularly more frequent upon mine opening among the population between 20 and 29 years (Fig. 3). In mining communities, this age group showed increased trends towards more risky behaviors in terms of having multiple sexual partners (OR: 4.20, 95% CI: 1.35–13.08), having high-risk sexual partners (OR: 2.02, 95% CI: 1.14–3.56) and abstaining condoms at high-risk sex (OR: 2.15, 95% CI: 1.08–4.30) compared with nonmining areas. In addition, men were particularly more likely to abstain from condoms (OR: 2.19, 95% CI: 1.27–3.77) whereas no significant effect was seen among women (OR: 1.49, 95% CI: 0.78–2.86). Furthermore, the impact of mine openings on the odds of people having multiple sexual partnerships was stronger in countries with low overall HIV prevalence (OR: 2.17, 95% CI: 1.26–3.76) compared with high-prevalence countries (OR: 0.90, 95% CI: 0.37–2.14).
DiscussionIn this article, we analyzed the impact of mine openings on HIV prevalence, HIV knowledge, and risky sexual behaviors, exploring 39 major mine openings across 16 SSA countries. We find that on average mining operations increase HIV prevalence by about 20% (from 5.8 to 7.3%), whereas surrounding areas simultaneously experienced a decrease from 6.7 to 6.0%. This corresponds to an almost two-fold increase in the odds of being HIV-positive after mine opening. Those living in high HIV prevalence countries and adults between 20 and 29 years were particularly affected. The populations living in operational mining sites had less knowledge about HIV, particularly men and the age group between 20 and 39 years. In addition, men close to operational mining sites were less likely to use condoms during high-risk sexual intercourse and there was an overall tendency towards increased risky sexual behaviors. Taken together, these findings suggest that mining activities significantly increase the risk of HIV in local populations.
Changes in HIV risk factorsIn the mining sites included in this study, risky sexual behaviors became more frequent and the knowledge about HIV decreased after mine opening. These findings are surprising for two reasons. Firstly, migrants in mining sites have been found to have higher education than the host population [31]. Nevertheless, mining areas continue to be environments conducive to risky sexual behaviors. Secondly, health management plans of mining projects often include HIV education programs for the workforce and the wider community [4,32]. The lack of knowledge and the lower condom use indicate that despite these programs, negative impacts on HIV transmission risks remain. Further research to assess the effectiveness of HIV mitigation programs to reach and educate affected communities is needed.
High-risk population groups in mining areasIn the stratified analyses, several particularly affected population groups were identified. Firstly, effects on HIV prevalence were stronger in high-prevalence countries. Work-related migration was found to predominantly increase risky sexual practices in host communities [7]. Such risky behaviors may have a stronger impact in settings where HIV is already widespread in the community. Furthermore, internal migrants from urban areas can promote HIV transmission in the often remote rural mining sites with previously few HIV infections [6,7,13]. If external migration from other countries is minimal, these effects may not be as pertinent in low-prevalence countries. Secondly, the strongest impacts were seen among the working-age population group, which is in line with a study on migrant miners in Eswatini and Lesotho [6]. Thirdly, the comparable impact of mine openings on HIV prevalence in men and women challenges the notion that HIV risks predominantly increase because of the influx of male work migrants. These findings suggest that the increased HIV prevalence in mining areas could be the result of both, external introductions from migrants and local transmission facilitated by widespread risky sexual behaviors [33]. In summary, these results underline the importance of systematically considering underlying individual-level and community-level risk factors when designing appropriate strategies for mitigating HIV risks in mining areas.
The need to mitigate HIV transmission risks in the context of natural resource extraction projectsGiven the evidence that HIV risk is strongly linked to industrial mining in SSA, there is a need to examine the current regulatory measures to mitigate potential risks to public health. Interestingly, compared with other health aspects, HIV risks in mining settings have recently received increased attention among international funding institutions and potential impacts on HIV transmission are commonly part of mitigation strategies of large industrial mines [5,32]. The mines in our sample have opened relatively recently, and should therefore, already reflect these trends. However, the public health expertise that is required for the identification and management of health impacts is often limited [34,35]. Often, vulnerable population groups are not identified, and hence, not specifically targeted by mitigation measures of mining companies [36]. The conduct of health impact assessment as part of the licensing of mining projects and continuous monitoring of community health are promising approaches for context-specific identification of high-risk groups and mitigation measures, as well as assuring the effectiveness of health interventions from mine construction to closure [15,34]. Such efforts to reduce HIV risks should also consider the role of often nearby artisanal and small-scale mining (ASM) activities [37]. In addition, this approach is similarly relevant for other industrial resource extraction activities, including oil and gas projects as contexts and activities are often very similar [38].
LimitationsAlthough the present study used the largest currently available dataset on trends in HIV prevalence in industrial mining areas in SSA, the approach also had limitations. First, the dataset consists of repeated cross-sectional surveys with independent samples of respondents rather than a consistent cohort. Adjusting for potential confounders and using trends in nearby, similar populations as comparison could alleviate this problem but we cannot rule out residual confounding through unmeasured factors. Yet, effects were seen predominantly among the working-age groups suggesting that the identified effects are indeed mining-related. Second, ASM activities located in proximity to industrial mines can also contribute to increased HIV transmission [37]. Informal mining activities are particularly present around gold mines, which make up the largest fraction of included mines [39]. As these activities are usually not established at the same time as the industrial mines, the difference-in-differences approach accounted for potential effects from ASM. Third, the effects are obtained for the combined sample of individuals exposed to industrial mines across SSA. The sample size did not allow for mine-level analyses to assess potential differences in impacts on HIV risks. Further research is needed to identify factors that affect the magnitude of impacts of individual mines. Fourth, impacts of mines may have extended beyond a 10 km radius, for example, along access roads or through other migratory patterns [7]. Also, the artificially introduced spatial inaccuracies to the true locations of the DHS clusters could have led to exposure misclassification. However, both factors are expected to bias the estimates towards the null and hence would rather lead to an underestimation of the true effect [40]. Finally, the prevalence estimates may not reflect the true prevalence of the study areas because of participation bias in the DHS surveys [41].
ConclusionOur analysis of 39 newly opened mines across 16 countries in SSA suggests that despite mitigation efforts, mining projects continue to be high-risk settings for HIV transmission characterized by lower HIV knowledge of the population and more frequent risky sexual practices. In light of the ambitious goals of the international community for curbing the HIV epidemic, efforts to reduce HIV risks in mining settings need to be strengthened.
AcknowledgementsFunding: funding for this study was received from the r4d programme (grant number 169461), a joint funding scheme by the Swiss National Science Foundation (SNSF) and the Swiss Agency for development and Cooperation (SDC).
Conflicts of interestThere are no conflicts of interest.
References 1. UN. Transforming our world: the 2030 Agenda for Sustainable Development. New York: United Nations; 2015. 2. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396:1204–1222. 3. Jahagirdar D, Walters MK, Novotney A, Brewer ED, Frank TD, Carter A, et al. Global, regional, and national sex-specific burden and control of the HIV epidemic, 1990–2019, for 204 countries and territories: the Global Burden of Diseases Study 2019. Lancet HIV 2021; 8:e633–e651. 4. ICMM. Good practice guidance on HIV/AIDS, tuberculosis and malaria. London, UK: International Council on Mining and Minerals; 2008. 5. IFC. Projects and people: a handbook for addressing project-induced in-migration. Washington DC: International Finance Corporation; 2009. 6. Corno L, de Walque D. Mines, migration and HIV/AIDS in Southern Africa. J Afr Econ 2012; 21:465–498. 7. Coffee M, Lurie MN, Garnett GP. Modelling the impact of migration on the HIV epidemic in South Africa. AIDS 2007; 21:343–350. 8. Campbell C. Migrancy, masculine identities and AIDS: the psychosocial context of HIV transmission on the South African gold mines. Social Sci Med 1997; 45:273–281. 9. Martins-Fonteyn E, Loquiha O, Wouters E, Raimundo I, Hens N, Aerts M, et al. HIV susceptibility among migrant miners in Chokwe. Int J Health Services 2016; 46:712–733. 10. Muchadenyika D. Women struggles and large-scale diamond mining in Marange, Zimbabwe. Extr Ind Soc 2015; 2:714–721. 11. Clift S, Anemona A, Watson-Jones D, Kanga Z, Ndeki L, Changalucha J, et al. Variations of HIV and STI prevalences within communities neighbouring new goldmines in Tanzania: importance for intervention design. Sex Transm Infect 2003; 79:307–312. 12. Baltazar CS, Horth R, Inguane C, Sathane I, César F, Ricardo H, et al. HIV prevalence and risk behaviors among Mozambicans working in South African mines. AIDS Behav 2015; 19: (Suppl 1): S59–67. 13. Baltazar SC, DeLima YV, Ricardo H, Botão C, Chitsondzo Langa D, da Costa P, et al. HIV prevalence and TB in migrant miners communities of origin in Gaza Province, Mozambique: the need for increasing awareness and knowledge. PLoS One 2020; 15:e0231303. 14. United Nations Economic Commission for Africa. Minerals and Africa's development: the international study group report on Africa's mineral regimes. Addis Abeba: United Nations Economic Commission for Africa; 2011. 15. Knoblauch AM, Divall MJ, Owuor M, Nduna K, Ng’uni H, Musunka G, et al. Experience and lessons from health impact assessment guiding prevention and control of HIV/AIDS in a copper mine project, northwestern Zambia. Infect Dis Poverty 2017; 6:114. 16. Lyatuu I, Winkler MS, Loss G, Farnham A, Dietler D, Fink G. Estimating the mortality burden of large scale mining projects—evidence from a prospective mortality surveillance study in Tanzania. PLoS Global Public Health 2021; 1:e0000008. 17. Lyatuu I, Loss G, Farnham A, Lyatuu GW, Fink G, Winkler MS. Associations between natural resource extraction and incidence of acute and chronic health conditions: evidence from Tanzania. Int J Environ Res Public Health 2021; 18:6052. 18. Tanser F, Bärnighausen T, Dobra A, Sartorius B. Identifying ‘corridors of HIV transmission’ in a severely affected rural South African population: a case for a shift toward targeted prevention strategies. Int J Epidemiol 2018; 47:537–549. 19. Westwood E, Orenstein M. Does resource development increase community sexually transmitted infections? An environmental scan. Extr Ind Soc 2016; 3:240–248. 20. USAID. The DHS Program. n.d. 21. Dietler D, Farnham A, Loss G, Fink G, Winkler MS. Impact of mining projects on water and sanitation infrastructures and associated child health outcomes: a multicountry analysis of Demographic and Health Surveys (DHS) in sub-Saharan Africa. Globalization Health 2021; 17:70. 22. Farnham A, Cossa H, Dietler D, Engebretsen R, Leuenberger A, Lyatuu I, et al. Investigating health impacts of natural resource extraction projects in Burkina Faso, Ghana, Mozambique, and Tanzania: protocol for a mixed methods study. JMIR Res Protocols 2020; 9:e17138. 23. Dietler D, Loss G, Farnham A, de Hoogh K, Fink G, Utzinger J, et al. Housing conditions and respiratory health in children in mining communities: an analysis of data from 27 countries in sub-Saharan Africa. Environ Impact Assess Rev 2021; 89:106591. 24. von der Goltz J, Barnwal P. Mines: the local wealth and health effects of mineral mining in developing countries. J Dev Econ 2019; 139:1–16. 25. KPMG International. Mining projects: Seeking greater value. In: KPMG International Cooperative; 2013. 26. Sloss L. Coal mine site reclamation. IEA Clean Coal Centre. 2013. 27. ICMM, IPIECA, Equator Principles Association. CSBI Timleline Tool: a tool for aligning timelines for project execution, biodiversity management and financing. In: Cross Sector Biodiversity Initiative; 2013. 28. Filmer D, Pritchett LH. Estimating wealth effects without expenditure data-or tears: an application to educational enrollments in states of India. Demography 2001; 38:115–132. 29. Bärnighausen T, Oldenburg C, Tugwell P, Bommer C, Ebert C, Barreto M, et al. Quasi-experimental study designs series-paper 7: assessing the assumptions. J Clin Epidemiol 2017; 89:53–66. 30. UNAIDS. HIV estimates with uncertainty bounds 1990-Present. 2021.
留言 (0)