
記住我






A total of 48 MPP children were included in this study. There were 16 (33.3%) cases in the embolism group (6 male; 10 female) and 32 cases (66.7%) in the non- embolism group (21 male; 11 female). The mean age of embolism and non- embolism patients was 7.13 ± 2.94 years and 6.08 ± 3.11 years, respectively. One child had obesity. There was no significant difference in age, BMI and gender between the two groups (P > 0.05).
Modified PIRO severity scoreBased on the modified PIRO severity score, half of the patients (2 patients with 4 points and 6 patients with 3 points) were at medium risk, whereas the other half (8 patients with 2 points) were at low risk in the embolism group. In the non- embolism group, 13 patients (3 patients with 4 points and 10 patients with 3 points) were at medium risk, whereas 19 (15 patients with 2 points, 4 patients with 1 points) were at low risk in the non-embolism group. There was no significant difference in the severity score between the two groups (P > 0.05).
Clinical manifestationsAll patients had a cough. All patients with embolism and 31 (97%) patients without embolism had a fever. And the MPP with embolism group had a higher fever than that of the non- embolism group (P < 0.05). All patients had no history of recent surgery, previous VTE and CVDs. One patient had been to ICU in embolism group and non- embolism group respectively. Six patients (37.5%) had more than one distribution of embolism (Table 1). In embolism group, 10 patients (62.5%) had pulmonary embolism, 3 patients (18.75%) had ventricle embolism, 2 patients (12.5%) presented cerebral and carotid artery embolism, one patient (6.25%) presented cerebral embolism, limb and spleen respectively. There was no significant difference in age, gender, BMI and time to CTA between the two groups (Table 2).
Table 1 The clinical symptoms and relevant involved vessels of pediatric MPP-associated embolismTable 2 Clinical characteristics and laboratory values of embolism in children with MPPLaboratory testsIn the embolism group, the values of D-dimer (closest to CTA/MRA), D-dimer (hospital admission), WBC (hospital admission), Fg (closest to CTA/MRA), C-reactive protein (CRP), neutrophil percent (N%), lactate dehydrogenase (LDH) and IgM (Immunoglobulin M) were significantly higher than that in the non-embolism group (P all < 0.05). The value of APTT in the embolism group was lower than that in the non- embolism group (P < 0.05). Nevertheless, PT, WBC (closest to CTA/MRA), Fg (hospital admission), PLT, IL-6, PCT, FER, CK, CKMB and ALT showed no significant difference between the two groups (P > 0.05) (Table 2). In the embolism group, two patients were tested for ACA, consequently, one patient was positive, whereas the other was negative. In addition, six patients were tested for ANA, and two patients (33.3%) showed positive (Table 1). In non-embolism group, there were six patients tested for ANA and fourteen patients tested for ACA. All the results were negative. Figure 1 shows the D-dimer values of patients (n = 16) tested over multiple days. Color-coded circles correspond to D-dimer values on different dates.
Fig. 1
D-dimer values of patients (n = 16) tested over multiple days. Color-coded circles correspond to D-dimer values on different dates
Imaging examinationPulmonary inflammatory consolidation was found in all the patients. Pulmonary embolism occurred on the same side as the pulmonary consolidation in 5 patients. The radiological abnormalities in the embolism-group were more severe than that in non- embolism group (Table 3). There were significant differences in pulmonary consolidation (⩾ 2/3 lobe), pleural effusion and atelectasis between two groups (P < 0.01). Nonetheless, the incidence of pleural thickening and necrotizing pneumonia showed no statistical difference between two groups (P > 0.05). Figure 2 shows the CTA images of pulmonary embolism, cerebral embolism and lower extremity embolism (Fig. 2).
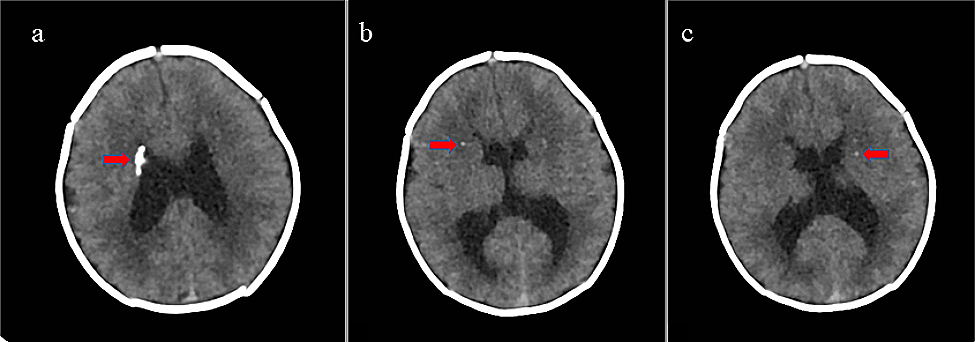
Table 3 Imaging of Embolism and non-Embolism children with MPPFig. 2
A Chest CTA showed a filling defect in the left upper pulmonary artery. B MRA examination of the head showed that the cavernous sinus segment of the left internal carotid artery, the middle cerebral artery and its branches were not developed. C CTA of lower limbs showed that the right posterior tibial artery was not developed locally
TreatmentThe average time from the onset of symptoms to admission for all patients was approximately 10 days, with no difference between the two groups (P > 0.05) (Table 2). Antibiotic treatment was similar for all MPP patients. Before admission, most patients had been initially treated with oral cephalosporins and macrolides. After admission, they were intravenously administered with azithromycin or doxycycline (age ≥ 8 years). Methylprednisolone was administered for anti-inflammatory treatment to patients with refractory Mycoplasma pneumoniae pneumonia. For patients with the value of D-dimer > 5.0 mg/L, patients were subcutaneously injected with 0.01 mL/kg of low molecular weight heparin(LMWH) every twelve hours for prophylactic anticoagulation until the value of D-dimer < 5.0 mg/L. For patients with embolism, they were applied LMWH to anticoagulate for 2 weeks. Two children were used urokinase(4400u/kg/h) for thrombolysis for 3 to 5 days. Patients were treated with rivaroxaban orally until the embolism disappeared after reexamination. The detailed information of patients before and after admission is shown in Table 4.
Table 4 Treatment before and after admissionOutcomeNo death and recurrent thrombosis occurred in all children. Pulmonary CTA revealed that the filling defect disappeared in all children with pulmonary embolism after 1 to 3 months. Three children with cardiac thrombus disappeared after 0.5–3 months. Three children with cerebral embolism were followed up for 1 year. Limb activity of one child was better than before, however, sequelae including hand shaking and slightly poor fine movement were evident. Two children still have some symptoms, such as unclear pronunciation, unstable walking alone, reduced muscle volume, decreased muscle strength, postural tremor, shaking of holding objects, etc. MRA of the head revealed that the distal end of the branch blood vessel had not developed without a change from the previous one. The establishment of certain softening foci accompanied the cerebral infarction.
Risk factors for embolism caused by MPPThe univariate analysisThe univariate analysis showed significant differences between the embolism group and non-embolism group in Tmax, CRP, D-dimer (closest to CTA/MRA), N%, pulmonary consolidation (⩾ 2/3 lobe), pleural effusion and atelectasis(P < 0.05).
ROC CurvesThe ROC analysis was used to explore the predictive factors for MPP with embolism, and the critical value with maximum sensitivity and specificity was also presented in Fig. 3. ROC analysis showed that D-dimer (closest to CTA/MRA), pulmonary consolidation (⩾ 2/3 lobe) and pleural effusion were significant in diagnosing MPP with embolism. When the cut-off value for the D-dimer (closest to CTA/MRA) was set at 3.55 μg/L, the sensitivity, specificity and AUC in recognized MPP with embolism were 0.875, 0.781 and 0.781, respectively in Table 5.
Fig. 3
ROC curve for predictive values of the independent correlation factors of MPP with embolism in children
Table 5 Predictive values of the independent correlation factors for Embolism children with MPPThe Multivariate logistic regression analysisSeven significant independent variables in the univariate analysis were performed for multiple logistic regression. D-dimer (closest to CTA/MRA) > 3.55 μg/L, pulmonary consolidation (⩾ 2/3 lobe) and pleural effusion played a significant role in predicting the MPP with embolism, with the odds ratio (OR) values of 1.255, 8.050, and 25.321, respectively (Table 6).
Table 6 Risk factors for embolism children with MPP
留言 (0)