
記住我

Recognizing the tradeoffs between continuity of care and provider fatigue, in 2017, the Accreditation Council for Graduate Medical Education began allowing programs the discretion to schedule first-year residents (interns) to work continuously for 24 hours at a time, with an additional 4 hours for ensuring education and safe and effective care transitions.1 This was an increase from the previous limit of 16 hours implemented in 2011 and was accompanied by increased expectations for supervision.2
Identifying the optimal schedule for physician trainees to witness the natural history of disease and the consequences of their interventions, time for educational activities, promotion of trainee well-being, and maximization of patient safety have been complicated. Proponents of strict and limited work-hour regulations have referenced cognitive impairments that are associated with moderate sleep deprivation3–5 and the potential contribution of fatigue to reduced well-being and increased errors, whereas advocates of more flexible duty hours have pointed out the potential dangers of delaying medical care, an increased frequency of error-prone handoffs, reduced continuity of care, and negative impacts on well-being that accompany less connectedness to their patients with limited duty hours.6
These discussions culminated in national, prospective trials showing that flexible work hour policies for surgical residents were noninferior to call schedules adhering to the 16-hour limit7 and that, among 63 randomized internal medicine residency programs, there were no significant differences between safety and provider alertness in hospitals with 24 + 4-hour shifts compared with 16-hour shifts. However, these studies also noted that attitudes differed significantly between interns and program directors about the impact of shift length.8–10
Although survey data have suggested that patients express greater concern about fatigue and working hours than about continuity of care,11 little research has evaluated the effect of intern work hours on the patient experience as well as the perceptions of the other members of the interdisciplinary care team, such as nurses.
In this prospective, controlled, mixed-methods study, we analyzed survey data from patients, interns, residents, attendings, and nurses in both “extended” (24 + 4-hour max) and “limited” (16-hour max) duty-hour intern call systems on 2 adjacent general medicine services that share identical nursing, pharmacy, and ancillary support staff. We also examined differences in objective outcome measures of patient care, including length of stay, intensive care unit (ICU) transfers, 30-day readmission rates, medication orders entered in error, rate of complications, and mortality.
METHODSPartners Healthcare Human Research Committee institutional review board approval was obtained in August 2017. Perceptions and attitudes of interns, residents, attendings, nurses, and patients were collected using anonymous paper surveys.
General Medicine Team UnitsInterns and residents were assigned to a general medicine team with either an extended duty-hour or limited duty-hour schedule. Both teams shared the same nursing, pharmacy, and ancillary support staff. Patient admission criteria were identical, up to a cap of 10 patients per intern. Each team consisted of 2 attending physicians, 2 supervising residents, and 4 interns who could collectively be assigned up to 20 patients. Interns on the extended duty-hour team experienced 24 + 4-hour shifts every 4 days from 7 am to 11 am the following day, with 4-hour protected off-pager for in-hospital rest in private call rooms from 2:00 to 6:00 am (extended duty hours); no new admissions could be assigned to an intern after 1 am, so that the last 10 hours of the shift was protected from new admissions. Interns on the limited duty-hour team experienced a “long call” admitting shift every 3 days with a maximum single-day work hour limit of 16 hours. Day interns on the limited duty-hour team transferred care to a single “twilight” intern each evening. In a 24-hour period, there were 2 transitions of care (or “hand-offs”) in the extended-duty team and 3 transitions of care in the limited duty-hour team. Interns were assigned to the teams based on preference (30% extended; 27.5% limited) or, if they expressed no preference, were randomly assigned (42.5%). Per Accreditation Council for Graduate Medical Education rules, both units maintained a maximum weekly work hour limit of 80 hours.
SurveysSurveys (Supplement 1, https://links.lww.com/JPS/A467) were developed in consultation with a statistician and reviewed and revised by the internal medicine program director. Resident and intern surveys were finalized after consultation with a group of residents.
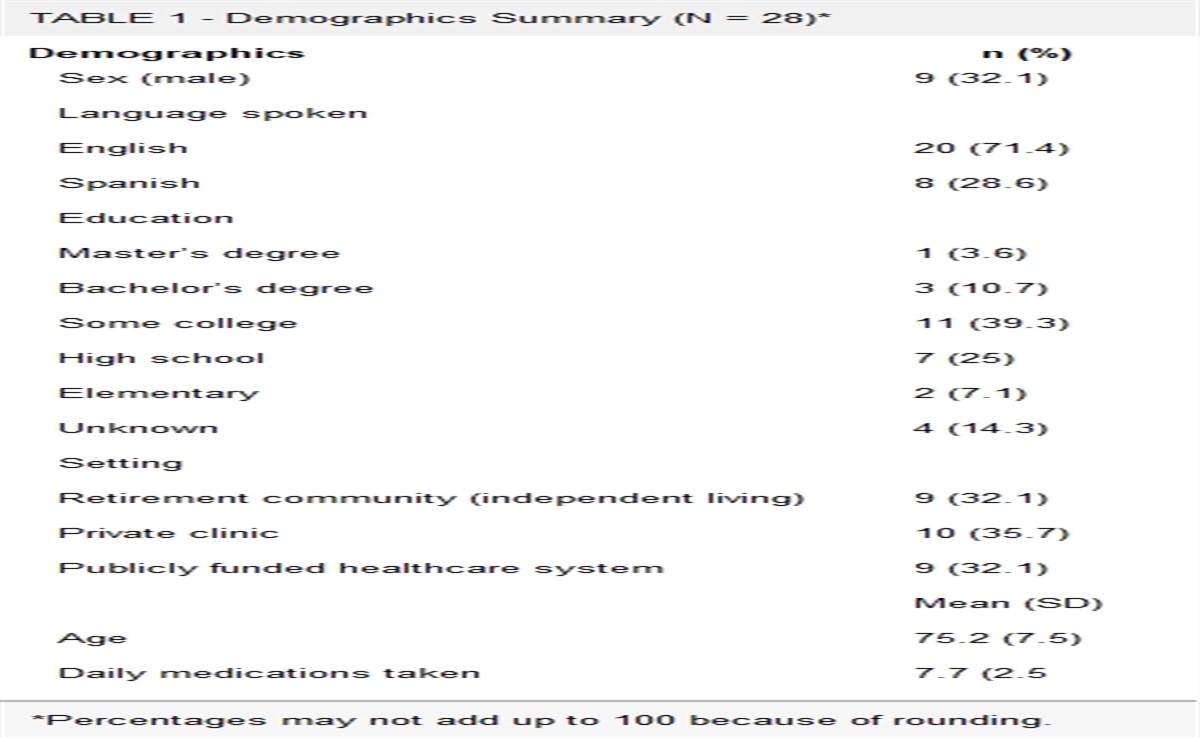
Patients (Table 1) were randomly sampled, consented, and completed anonymous surveys, from September 2017 to May 2018. Patients were only told that the study aimed to evaluate the care by the interdisciplinary care team. Patients were not told about differences in work hours. Patients were asked how many times they saw their doctor or the medical team, how well the doctors knew their medical issues, how well the doctors listened, and their overall satisfaction. Patients were offered to have the survey questions and possible answers read to them by the surveyor, who recorded the patient’s responses and verbatim comments. Patients were excluded if they were non-English speakers or were not oriented to person and place.
TABLE 1 - Patient Demographics, Anonymous Survey Responses, and Objective Outcomes Patients Extended Duty Limited Duty χ2P Value 95% CI Total participants 228 221 Mean Age, y 60.5 60.8 0.984 0.12 to 0.48 Women, % 52.6 50.2 0.429 2.3 to 2.49 Patients who reported unfavorable ratings, n (%) Overall satisfaction of the medical team 12 (5.2) 11 (5.0) 0.936 0.02 to 0.38 How well the doctors listen 15 (6.6) 15 (6.8) 0.901 0.02 to 0.32 How well the doctors know their problems 14 (6.1) 22 (9.9) 0.135 3.61 to 3.98 Objective data ICU transfers 3 5 0.453 −0.035 to 0.015 Average length of stay, d 7.62 6.96 0.301 −0.589 to 1.909 Patients who developed complications during admission 69 63 0.469 −0.064 to 0.104)For each survey item, the response choice was dichotomized into a binary response of negative effect (“unfavorable”) versus no effect or positive effect. Of patient surveys, 439 of 449 (97.8%) answered every analyzed survey question; 7 (1.6%) of the patient surveys had 1 question unanswered, and 1 (0.72%) had 3 analyzed questions unanswered. P < 0.05 was used to identify significance.
CI, confidence interval.
Physician surveys evaluated perceptions of intern tiredness, overall satisfaction, and performance, including quality of presentations, completion of physical exams, and incorrect order placement. For interns, residents, and attendings, individual surveys were distributed and collected weekly for the 2017–2018 academic year starting in September, to first allow interns and junior residents to become adjusted to general hospital workflows, through May 2018. Surveys were not collected during holidays because of changes in resident coverage schedules. To evaluate changes over the course of the rotation, an analysis was conducted for each week of the monthlong rotation, in the aggregate. To evaluate for changes over the course of the academic year, data were analyzed in sequential 3-month blocks over the course of the academic year.
Anonymous nurse surveys were distributed and collected, 5 times from September 2017 to the end of May 2018, which assessed their perception of the quality of care provided by the interns, intern responsiveness to pages, and the overall team dynamic compared with other unit. These were spaced throughout the study periods to maximize participation and identify whether nursing perceptions changed over the 9-month duration of the study.
Objective Patient Outcome DataFor all consented patients, charts were reviewed to determine length of stay, 30-day readmission rate, 30-day emergency department visits, ICU transfers, complications, and mortality. Complications were determined by electronic chart review of progress notes and problem lists, with 2 physician reviewers who were blinded to the unit and were done dependently. Disagreements were resolved with discussion and further chart review. Each chart review took approximately 7 to 10 minutes to complete.
After discharge, the charts of consented patients were also reviewed by hospital pharmacists and evaluated for flagged pharmacy-level interventions (IVENTs, an Epic tool used to communicate and record ASP recommendations and interventions) during the patient stay, including dose/schedule changes, product changes, inappropriate therapies, and necessary therapeutic substitutions. Each patient chart was independently reviewed by 2 pharmacists, with disagreements resolved with subsequent discussion. Pharmacy flags for antimicrobial stewardship improvements or optimization of therapy were not counted as errors. Subsequently, these interventions were reviewed dependently by 2 physician reviewers in a blinded fashion to stratify the flags based on potential clinical significance. All medication errors involving opiates, benzodiazepines, therapeutic anticoagulation, dual antiplatelet therapy, antiepileptics, and nonprophylactic antimicrobials were classified as clinically significant. The classification of other medication errors was based on further chart review and discussion between physician reviewers.
Statistical MethodsPerceptions and attitudes were measured with survey questions that asked for responses on a 5-point Likert scale. For the purpose of data analysis, survey responses were collapsed into positive (beneficial) and negative (unfavorable) categories and analyzed using χ2 tests for independence. We have also included calculations and confidence intervals in Tables 1–4.
TABLE 2 - Physician Demographics and Survey Responses Extended Duty Limited Duty P 95% CI Intern demographics and responses Total responses (% of total) 57 (41.0) 82 (59.0) Women, % 47 76 <0.001 28.8 to 29.2 Interns who reported a beneficial effect, n (%) Knowing their assigned patients 14 (24) 60 (73) <0.001 48.7 to 49.3 Presenting patients they know 10 (17) 42 (51) <0.001 33.7 to 34.3 Conducting a physical exam on new patients 15 (26) 61 (74) <0.001 46.71 to 47.3 Quality of teaching 23 (40) 67 (82) <0.001 40.8 to 41.8 Level of tiredness 4 (7) 44 (54) <0.001 46.7 to 47.3 Overall satisfaction 7 (12) 64 (78) <0.001 62.7 to 65.3 Resident demographics and responses Total responses (% of total) 34 (57.6) 25 (42.4) Women, % 66 48 0.201 18.7 to 19.2 Residents who reported a beneficial effect, n (%) Quality of intern presentations of new patients 18 (53) 11 (44) 0.248 8.59 to 9.414 Quality of intern presentations of patients known to the service 8 (24) 10 (40) 0.093 15.6 to 16.4 Overall quality of care provided by the interns 18 (53) 20 (80) 0.016 26.5 to 27.4 Perception of intern tiredness 1 (3) 15 (60) <0.001 56.5 to 57.5 Incorrect orders placed by intern 4 (12) 10 (40) 0.006 27.6 to 28.4 Overall teaching on the service 15 (44) 18 (72) 0.016 27.5 to 28.5 Attending demographics and responses Total responses (% of total) 32 (58.1) 23 (41.8) Women, % 13 26 0.197 12.8 to 13.2 Attendings who reported a beneficial effect, n (%) Quality of intern presentations of new patients 28 (88) 8 (35) <0.001 52.7 to 53.3 Quality of intern presentations of patients known to the service 16 (50) 10 (43) 0.305 6.64 to 7.36 Overall quality of care provided by the interns 14 (43) 10 (43) 0.500 −0.32 to 0.32 Overall teaching on the service 17 (53) 14 (65) 0.187 8.57 to 9.43For each survey item, the response choice was dichotomized into a binary response of positive effect (“beneficial”) versus no effect or negative effect. Of intern surveys, 136 of 139 (97.8%) answered every analyzed survey question; 2 (1.4%) of the intern surveys had one question unanswered, and 1 (0.72%) had 3 analyzed questions unanswered. Of resident surveys, 136 of 139 (97.8%) answered every analyzed survey question; 1 (1.6%) of the resident surveys had 1 analyzed question unanswered, and 1 (1.6%) had 2 analyzed questions unanswered. Of attending surveys, 54 of 55 (98.2%) answered every analyzed survey question; 1 (1.8%) of the attending surveys had 1 question analyzed unanswered. P < 0.05 was used to identify significance.
CI, confidence interval.
Intern responses over initial 3 months (trimester 1, September–November), subsequent 3 months (trimester 2, December–February), and final 3 months (trimester 3, March–May) of study period. For each survey item, the response choice was dichotomized into a binary response of positive effect (“beneficial”) versus no effect or negative effect. P < 0.05 was used to identify significance.
CI, confidence interval.
For each survey item, the response choice was dichotomized into a binary response of positive effect (“beneficial”) versus no effect or negative effect. Of nurses’ responses, 47 (92.2%) answered all analyzed survey questions. Nurses were asked to compare “overall team effectiveness” and “intern responsiveness to pages” only if they had rotated on both services. Four nurses (7.8%) did not answer this question. P < 0.05 was used to identify significance.
CI, confidence interval.
In those instances where survey data could not be analyzed in this way, for instance, patient length of stay in the hospital, data were treated as continuous and analyzed using independent-samples t tests. We use an α of 0.05 throughout this study to denote statistical significance, although we report specific P values throughout. Data analysis was conducted using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, New York).
RESULTS Survey Results PatientsThere were 228 patients on the extended duty-hour unit and 221 on the limited duty-hour unit who consented to be part of the study and completed the survey (Table 1). There was no significant difference in the average age and sex of the patients recruited, the number who declined to participate, or the number who had the surveys conducted verbally. Patient survey data indicated no significant differences in the patients’ perception of the number of times they saw their doctors or the medical team, how well the doctors knew their medical problems, how well the doctors listened, or overall satisfaction.
Nineteen patients (4.3% of total patients), on subsequent chart review, were discovered to not have been under the care of either medicine service. They were patients cared for by either oncology or neurology services who had been placed on these units because of bed availability. Their data were included in the survey responses because of the anonymous nature of the surveys and inability to identity these surveys in retrospect. However, these patients were excluded from the objective outcome analyses. One patient was misidentified as being on limited duty-hour unit when they were under the care of the extended duty-hour team. This patient’s data were included in the survey responses because of the lack of identifying markers but were assigned to the appropriate service for the objective outcome data analyses.
PhysiciansSixty-two unique interns (40 women; ages, 25–34 years), 27 unique residents (16 women), and 28 unique attendings (5 women) participated. The total number of surveys (including subsequent weekly survey administrations over the course of the rotation) resulted in 139 completed intern surveys, 59 completed resident surveys, and 55 completed attending surveys (Table 2). Over 36 separate survey administrations during the 9-month survey period, the overall survey response rates were 64.4% for interns, 81.9% for residents, and 39% for attendings. The rates that each intern, resident, and attending filled out the survey at least once were 83.7%, 73.0%, and 58.8%, respectively.
Interns assigned to the extended schedule reported less familiarity with their assigned patients (24% versus 73% reporting a beneficial effect, P < 0.001), a decreased ability to conduct physical exams on new patients (27% versus 74%, P < 0.05), increased perceptions of tiredness (7% versus 54%, P < 0.001), decreased quality of teaching (41% versus 82%, P < 0.001), and decreased overall satisfaction (12% versus 78%, P < 0.001; see Table 2 and Fig. 1 for full responses).
 FIGURE 1:
FIGURE 1: Graphical representation of anonymous intern, resident, and attending survey responses over a 9-month survey period. *P < 0.01. **P < 0.05.
Residents overseeing interns on the extended schedule reported lower quality of care provided by the interns (53% versus 80% reporting a beneficial effect, P = 0.016), increased perceptions of intern tiredness (3% versus 60%, P < 0.001), increased incorrect orders (12% versus 40% P = 0.006), and lower overall quality of teaching on the service (44% versus 72%, P = 0.016; Table 2).
There were no significant differences in resident perceptions of intern performance during new patient presentations or presentations of previously admitted patients. In a separate question posed only to residents in the extended duty-hour schedule, 47.1% of the residents reported that extended duty-hour interns performed at an “inferior” or “far inferior” level, whereas 16.7% of resident surveys reported that the extended duty-hour interns performed at a “superior” or “far superior” level compared with their prior experiences supervising limited duty-hour interns on other general medicine services. There was no difference in responses between PGY-2 and PGY-3 residents.
Attending physicians were significantly more likely to report higher-quality new patient presentations by interns working on the extended duty-hour schedule as superior to interns that they had supervised on other services with limited duty-hour schedules 88% (extended duty hours) versus 35% (limited duty hours; P < 0.001), without significant differences in perceptions of the quality of presentations of patients known to the service, overall quality of care, or overall quality teaching (Table 2).
Throughout the academic year, extended duty-hour interns reported a significantly increased perception of their ability to perform physical exams and a decreased perception of presenting patients unfamiliar to them, whereas limited duty-hour interns reported increased perceptions in overall knowledge of their patients and the quality of teaching (Table 3). Intern perceptions of tiredness and overall intern satisfaction did not significantly change in either unit as the academic year progressed. Resident and attending survey response scores did not change significantly in either unit as the academic year progressed.
NursesForty-eight surveys were completed by 31 nurses over the duration of the study. There was no significant difference in nursing perceptions of the quality of intern care, team dynamics, or responsiveness to pages (Table 4). There were no significant differences in nursing responses across the 5 separate survey administrations.
Objective Patient Outcome Data Patient Chart ReviewThere were no significant differences between length of stay, ICU transfers, 30-day readmission rates, 30-day emergency department visits, complications (see Table 5 for the full list of complications), or mortality.
TABLE 5 - Total Complications on Extended Duty-Hour and Limited Duty-Hour Services Complication Extended-Duty Service Limited-Duty Service Neurologic/behavioral/psychiatric Hospital delirium without agitation/violence 1 4 Psychosis or hospital delirium with agitation/violence episodes 1 2 Vertigo or lightheadedness 1 1 Altered mental status 1 2 Focal neurologic deficit 1 1 Seizure 1 1 Suicidal ideation 1 0 Cardiovascular Hemodynamic compromise (hypotension, shock) 6 9 Atrial arrhythmia or nonsustained ventricular tachycardia without hemodynamic compromise 4 7 Hyper/hypokalemia with ECG changes 2 4 Hyper/hypokalemia without ECG changes 0 4 Myocardial infarction 0 3 Cardiac arrest 0 2 Complete heart block 1 0 Hypertensive emergency 0 1 Angina 1 0 Volume overload without sequelae 0 1
留言 (0)