
記住我

This study is based on the Colorectal Cancer Database (CRCBaSe), a mega-linkage originating from the SCRCR, which was further linked to national registers at the National Board of Welfare and Statistics Sweden. The SCRCR was used to identify patients, to get information on the registering hospital and on surgery of metastases and primary tumour, and to retrieve data on potential confounders and descriptive variables. When a patient is diagnosed with CRC, the hospital is responsible for registering the patient in the SCRCR and the managing hospital is automatically recorded when starting a registration in the SCRCR.
The Swedish Cancer Register (SCR), which dates back to 1958, was used to retrieve data on other cancer diagnoses and include data on previous CRC diagnoses not captured by the SCRCR, to ensure that only the first CRC diagnosis was included. Information from the Cause of Death Register was used to retrieve information on cause and date of death. The In- and Out-Patient Register was used to obtain information on comorbidities and to define presence of metastatic disease, receival of primary tumour resection and surgery of lung, liver and peritoneal metastases (Supplementary Table 1). From the Register of the Total Population, data on civil status and migration was extracted. From the Longitudinal Integrated Database for Health Insurance and Labour Market Studies data on disposable income per family unit and educational level were extracted. Civil status and highest achieved level of education were defined at the time of CRC diagnosis, while for income, information on the year prior to CRC diagnosis was used. If data was unavailable for the mentioned year, data from 0–3 years before year of diagnosis was used instead.
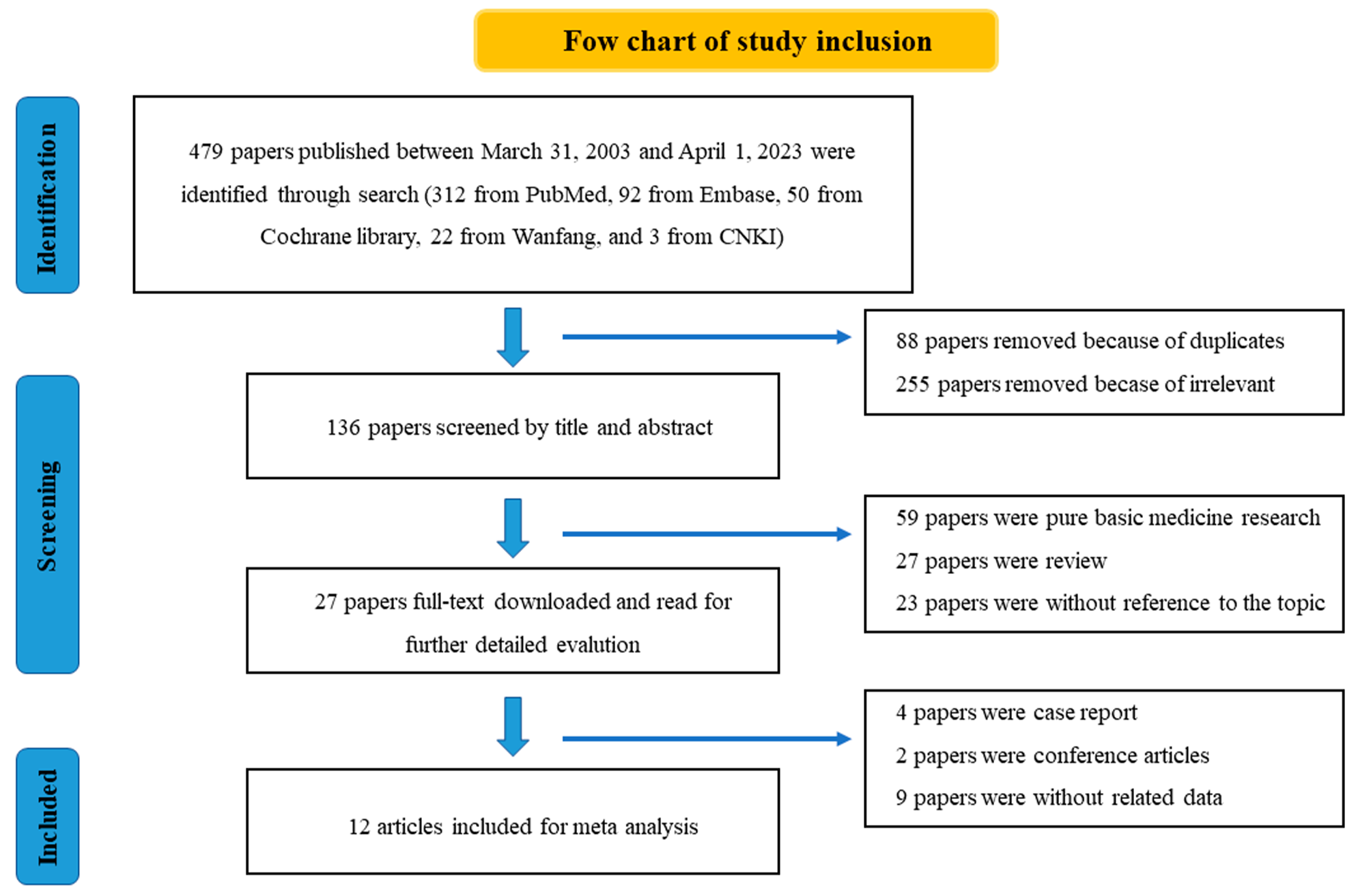
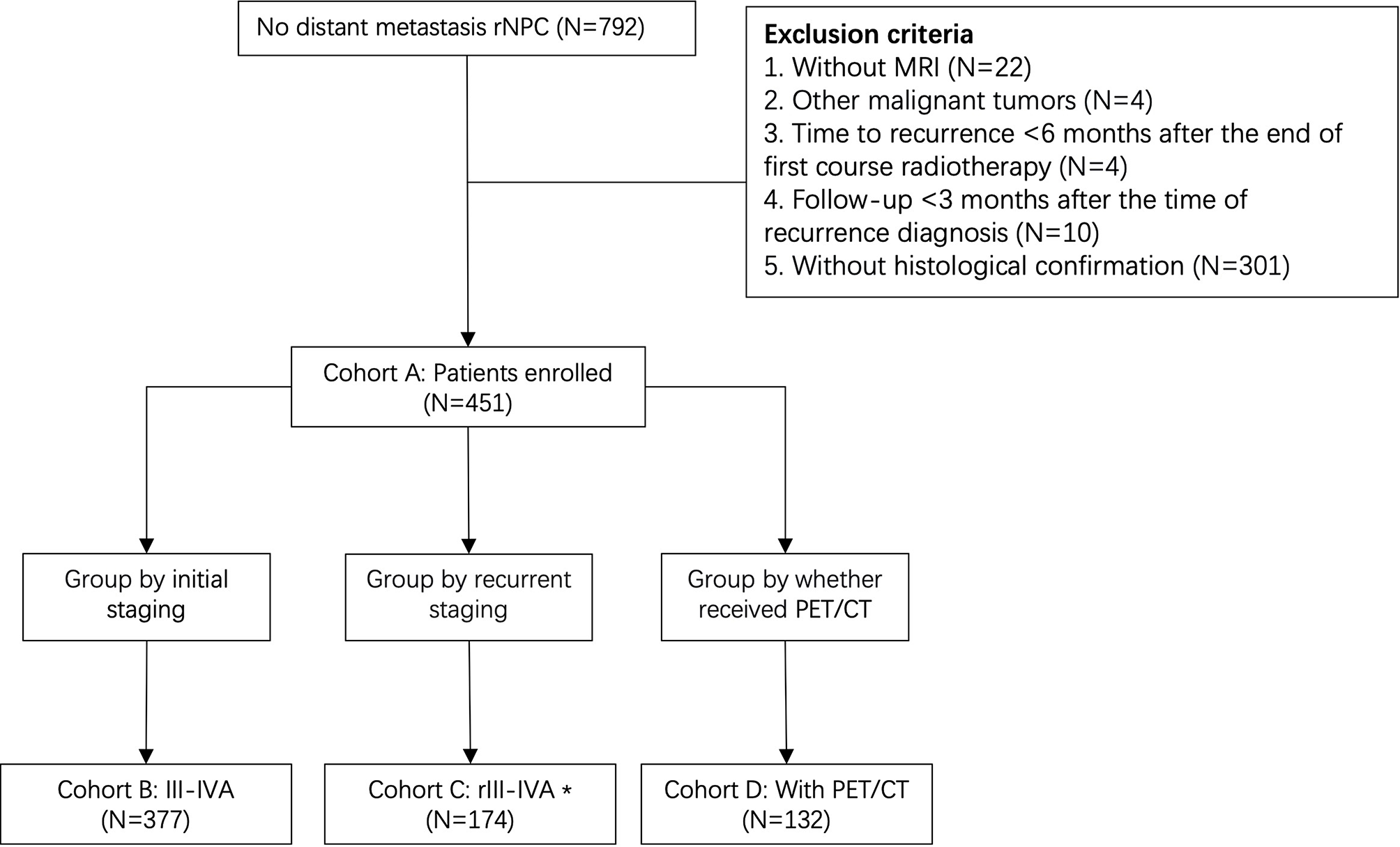
Inclusion and exclusion criteriaAll Swedish adult patients (≥ 18 years old) with a first-time CRC diagnosis in the SCRCR during 2009–2016, with no previous diagnosis of CRC in SCR, were included (n = 46,160). The following exclusions criteria were applied: no presence of synchronous metastatic disease according to a clinical or pathological assessment (n = 35,737), no specified metastatic location (n = 451), and missing data on registering hospital (n = 4). The final study population consisted of 9,968 patients (Fig. 1).
Fig. 1
Flowchart showing study criteria for patients diagnosed with first-time synchronous metastatic colorectal cancer in 2009–2016. *Within predefined time window: 90 days before diagnosis to 270 days after diagnosis. Abbreviations: CRC=colorectal cancer, IPR=In-Patient Register,OPR=Out-Patient Register, SCR=Swedish Cancer Register, SCRCR=Swedish Colorectal Cancer Register
Fig 2 A-D
Metastatic surgery by A) year B) hospital volume, C) hospital level and D) healthcare region. Including 9,968 patients with synchronous metastatic colorectal cancer (mCRC). The figures show the proportion receiving metastatic surgery between 90 days before mCRC diagnosis and 270 days after. P-value from trend test was < 0.001 for A-B and P-value from chi square test was < 0.001 for C-D.
Exposures and outcomesOur primary exposure was annual hospital volume of incident mCRC patients, i.e., the total number of patients diagnosed with mCRC at a specific hospital during a given year. The annual hospital volume was divided into quartiles (≤ 25th, > 25th to ≤ 50th, > 50th to ≤ 75th, and > 75th). As such, the same hospital could be exposed as a 1st quartile hospital one year and then fall into another quartile of hospital volume another year. Additionally, level of hospital (university or non-university) and its association with odds of metastatic surgery was investigated. Our primary outcome was receiving metastatic surgery (yes/no), which was defined as receiving surgical resection including a non-surgical locally ablative procedure of liver, and/or peritoneal, and/or lung metastases within 90 days prior to and 270 days after the date of primary CRC diagnosis date (Supplementary Table 2). This time window was chosen to encompass the majority of treatments for synchronous metastases, but not include treatment for metachronous metastases. Furthermore, it was required that the patient underwent primary tumour resection, either before, simultaneously or after the surgery of the metastases, to be defined as having received the primary outcome. Our secondary outcome was OS from date of diagnosis.
Statistical methodsFrequencies and proportions of patient and tumour characteristics were calculated separately within hospital volume quartiles. The proportion of patients receiving metastatic surgery by year of diagnosis, hospital volume quartiles, hospital level, and healthcare region, were visualised using bar charts. Chi-squared tests were used for formal testing of differences in distributions, and logistic regression was applied to evaluate trends.
Crude and adjusted logistic regression models were fitted to estimate odds ratios (ORs) with 95% confidence intervals (CIs) of receiving metastatic surgery. The first multivariable model included one exposure (hospital volume or level) and adjusted for sex (female, male), age (18–64 years, 65–79 years and ≥ 80 years old), Charlson comorbidity index (CCI) [28] (0, 1 and ≥ 2), year of diagnosis (continuous 2009–2016), location of the primary tumour (right colon, transverse colon, left colon, and unknown location in colon or rectum), clinical tumour (cT) stage (1–3, 4, X), clinical nodal (cN) stage (0, 1–2, X), extent of metastatic disease (single location/ multiple locations), civil status (married/registered partner, or not married), highest commenced educational level (primary school, secondary school, or higher education) and disposable income per family unit (divided into four quartiles per year of diagnosis). A second multivariable model was constructed including both exposures (hospital volume and level) and adjusted for the variables mentioned above. An additional multivariable model also included the potential mediator MDT (yes/no). Tests for interactions between hospital volume and hospital level, and hospital level and MDT conference, were performed using a Wald test. Missing data were included in the adjusted models by use of the missing-indicator method [29].
For the survival analyses, the patients were followed from date of diagnosis until date of death, migration, or 31st December 2017, whichever occurred first. The underlying time scale was time since diagnosis. The Kaplan–Meier method was used to calculate OS proportions, and the log rank test to test for survival differences, by hospital volume and hospital level. Cox regression models were used to estimate hazard ratios (HRs) with 95% CIs of the all-cause mortality rate for the four hospital volume quartiles and hospital level. Both univariable and multivariable models were fitted, where the latter adjusted for the same variables as described in the multivariable logistic regression models above. The proportional hazard assumption was formally tested using the Schoenfeld residuals.
A sensitivity analysis was performed using a delayed entry model, in which follow-up started at 270 days after diagnosis. Patients who died (n = 3,964) or were administratively censored (n = 11) during these 270 days were not included in this analysis (n,included = 5,993). The Kaplan–Meier method was used to calculate OS proportions, and the log rank test to test for survival differences, by whether the patients received metastatic surgery or not.
The significance level was set to 5%. Statistical analyses were done using Stata (StataCorp. 2017. Stata Statistical Software: Release 16. College Station, TX: StataCorp, LLC).
Ethical approvalEthical approval was given by the Regional Board of the Ethical Committee in Stockholm, Sweden (DNR: 2014/71–31, 2018/328–32, 2021–00,342) and the study was conducted in accordance with the ethical standards described.
留言 (0)