
記住我

To prioritize patient safety issues and determine the effects of various patient safety interventions, it is essential to examine the status of patient safety and follow up on patient safety trends.1,2 Various methods, each with unique strengths and weaknesses, are used to examine the status of patient safety.3,4 One representative example is the patient safety reporting and learning system that prepares and disseminates the strategy for improvement based on the details of reports on patient safety incidents from medical professionals. However, there may be issues in assessing patient safety solely based on this system because it relies on self-reports, and the incidence of reports varies depending on the medical institution’s level of awareness of patient safety.5
As such, studies have aimed to review medical records to comprehensively identify the status of patient safety.6 Because the Harvard Medical Practice Study was conducted in the United States to examine the incidence and characteristics of adverse events through a retrospective review of medical records of patients,7,8 the method used in that study has been used worldwide, including in Australia, Canada, the Netherlands, and Sweden, to conduct a medical record review at the national level.9–17 Although medical record reviews are regarded as the criterion standard for identifying adverse events, studies have indicated the importance of improving reliability among reviewers, including physicians and nurses.6,18,19 In addition, improving the feasibility of medical record review for the identification of adverse events requires resolving issues of high cost, its time-consuming nature, and the importance of the quality of medical records.3,4
In the case of the Republic of Korea (hereinafter Korea), the Korea National Patient Safety Incidents Inquiry (KNPSII) survey was conducted to identify the incidence and characteristics of adverse events after the establishment of the first Comprehensive Plans for Patient Safety as a part of the 5-year plan to improve patient safety and quality of medicine. Specifically, a 3-stage retrospective medical record review was conducted in 15 regional public hospitals in Korea to determine the efficacy of using medical record review to identify adverse events.18,20–22 The detailed characteristics of the adverse events identified in this particular survey have been discussed in a previous article.23
This study focused on the feasibility of the KNPSII survey. Specifically, the study aimed to examine the validity of the screening criteria, interreviewer reliability, the quality of medical records, and the amount of time needed to review medical records. Previous research has focused on the reliability of medical records6,19 and rarely reported the aspects to be considered in terms of feasibility. We expect the results of this study to contribute to the improvement of the methodology of medical record review for the identification of adverse events to enhance feasibility.
METHODS Study DesignThis study conducted a 3-stage retrospective medical record review in 15 regional public hospitals in Korea based on the methodology of previous studies.7,16,20 It was conducted in accordance with the first Comprehensive Plans for Patient Safety and was exempted from ethical approval in accordance with Article 2 Paragraph 2 Subparagraph 1 of the Enforcement Rule of the Bioethics and Safety Act.24
Medical Record ReviewIn stage 1 of the medical record review, 2 nurses independently verified the presence of 41 screening criteria in the electronic medical records of the patients. In stage 2 of the review, 2 physicians independently assessed the incidence of adverse events for the patients identified in stage 1 of the review to complete a detailed adverse event report. In stage 3, in accordance with suggestions from a previous study,20 the results of stage 2 were reviewed further by a review committee, which consisted of individuals with experience in a previous related study or experts in the field of patient safety. The results for each institution were summarized based on details of the adverse events determined in stage 3, including the number of events, degree of harm, causality, and preventability, to determine the final adverse events by pooling the outcomes from each institution. An interim audit was conducted by the institution during the review to share review experience among the reviewers and discuss any differences in opinion so that consistent criteria can be used in the review. In case queries arose during the review, consistent answers were provided through an expert review through the management of the corresponding institution, which was also shared with other reviewers.
MeasuresIn the stage 1 review, data including reviewer information (duration of review, etc.), patient information (sex, duration of hospitalization, department of admission, route of admission, etc.), presence of screening criteria, and medical records quality assessment were collected. The screening criteria included the following 41 items in 7 areas in total: “general: admission, discharge, and transfer”; “events”; “drug, fluid, blood”; “test results”; “related surgery”; “obstetrics and neonates”; and “others.” Any patient with at least one screening criterion identified by at least one reviewer in the stage 1 review progressed to stage 2 for further review.
In stage 2 of the review, reviewer information (duration of review, etc.), incidence of adverse events, detailed adverse event report (type of adverse event, degree of harm, causality, preventability, etc.), and medical record quality assessment were collected. The quality of medical records in stage 1 and stage 2 review was evaluated as a single comprehensive question on a 4-point scale as follows: 1 (very poor), 2 (poor), 3 (good), and 4 (very good).
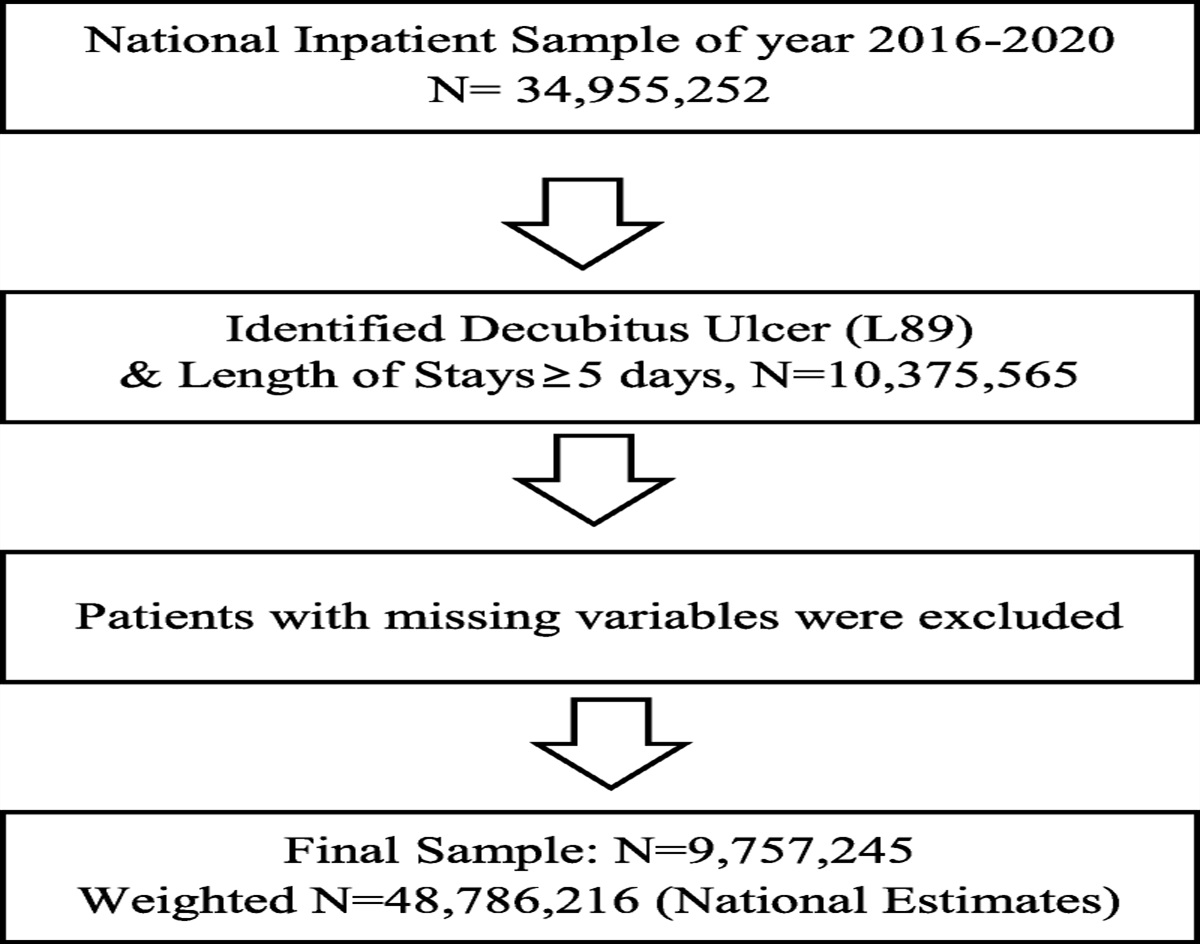
Patient SelectionThis survey was conducted at 15 general hospital-level medical institutions with at least 200 beds among 33 regional public hospitals in Korea. We used data from patients who were discharged in 2016. Using the random number table, data from 500 patients who were discharged on a randomly extracted date between January 1, 2016, and December 31, 2016, were reviewed for each institution, and a total of 7500 discharged patients were surveyed (500 per institution). The number of samples was calculated by institution based on similar studies.21,25
Data were included if the patient records were complete with all discharge summaries and coding, if the patient was in the hospital for at least 24 hours, and if the patient was 19 years or older. Data were excluded if the patient was admitted for the first time at the Department of Traditional Korean Medicine, Dental Care, Psychiatry, or Rehabilitation Care. The scope of review for medical records was 1 year before and after the discharge date of the index admission. For example, if September 1, 2016, was selected as the discharge date, the scope of review for medical records was between September 1, 2015, and September 1, 2017.
Education of ReviewersFor stages 1 and 2, two reviewers who were trained in the method of reviewing medical records were recruited internally from each institution. Reviewers were recruited from an externally affiliated institution if it was difficult to recruit internally. A total of 30 reviewers were selected for stages 1 and 2, and attended a class about patient safety–related terminology and the identification of adverse events through medical record review. Two experts with previous experiences in conducting medical record review studies to detect adverse events educated reviewers. The class took about 1.5 hours. Subsequently, reviewers took part in an approximately 1.5-hour practice review using 2 sample medical records and case studies on the score for causality and preventability by each adverse event. The case studies were discussed to ensure that consistent review criteria could be established; they mostly included cases in which there was confusion in the decision.
Statistical AnalysisReview results were summarized using Microsoft Office Excel 2013 (Microsoft Corporation, Redmond, Washington), and descriptive analyses were conducted using IBM SPSS 20 (IBM, Armonk, New York). The sensitivity and positive predictive values were calculated for the adverse events, and interreviewer reliability was verified using the overall agreement rate and the κ value. The reliability of the stage 1 results was based on whether there was a need for a second review by reviewing at least one screening criterion for a particular patient. Reliability of the stage 2 results was based on the agreement in the reviewers’ opinions about the occurrence of an adverse event, the degree of harm, the causality, and the preventability. “Perfect match” was defined as agreement in all of the opinions for the occurrence of an adverse event, the degree of harm, the causality, and the preventability; “partial match” was defined as agreement on the decision for adverse event but disagreement in the degree of harm, causality, or preventability. In addition, the quality assessment and duration of review of medical records were compared and examined among the institutions and the stage 1 and 2 reviewers.
RESULTSThere were a total of 4159 patients with at least 1 of the 41 screening criteria, accounting for 55.5% of all patients. The highest incidence was found for “specialty consult,” followed by “length of index was over 30 days,” “transfusion or use of blood products,” “in-unit procedure,” and “decrease in hemoglobin or hematocrit of 25% or greater” (Table 1). The positive predictive value in stage 1 was 17.9%. The screening criterion with the highest positive predictive value was “mechanical ventilation greater than 24 hours post-op.” The highest sensitivity was observed for “specialty consult,” followed by “length of index was over 30 days” and “in-unit procedure.”
TABLE 1 - Frequency and Sensitivity of Screening Criteria Screening Criteria Patients of Second Stage Review, n (%) Sensitivity, % Positive Predictive Value, % [General: admission, discharge, and transfer] 1. The index admission was an unplanned admission related to previous healthcare management 765 (5.1) 10.2 13.1 2. Length of index was more than 30 d 1667 (11.2) 34.9 28.6 3. Unplanned readmission after discharge from index admission 798 (5.4) 14.5 17.1 4. Revisiting emergency department within 72 h after discharge from index admission 180 (1.2) 3.9 18.7 5. Unplanned transfer to another acute care hospital 320 (2.2) 5.2 18.3 6. Temperature higher than 38.3°C at the point of discharge 44 (0.3) 1.1 24.2 7. Unplanned transfer from general care to intensive care 181 (1.2) 7.4 41.0 8. Specialty consult 2262 (15.2) 42.0 19.4 [Events] 9. Cardiac or respiratory arrest, rapid response team activation 152 (1.0) 5.2 34.2 10. Death in hospital 661 (4.4) 10.1 22.3 11. Hospital incurred patient injury 442 (3.0) 29.3 69.4 12. Oversedation/hypotension 268 (1.8) 9.4 33.5 13. Restraint use 439 (3.0) 11.1 28.8 14. Acute dialysis 11 (0.1) 0.3 25.0 15. In-unit procedure 1329 (8.9) 30.6 26.1 16. Treatment of organ damage after an invasive procedure 19 (0.1) 1.3 71.4 17. Acute myocardial infarction, cerebrovascular accident, or pulmonary embolus during or after an invasive procedure 7 (0.0) 0.4 42.9 [Drug, fluid, blood] 18. Transfusion or use of blood products 1,463 (9.8) 31.7 30.0 19. Peniramin injection (chlorpheniramine maleate 4 mg) or Chlorpheniramine Maleate Injection Huons (chlorpheniramine maleate 4 mg) use by intramuscular or intravenous route 170 (1.1) 7.4 43.0 20. Abrupt medication stop 853 (5.7) 25.0 28.4 21. Antidotes use 86 (0.6) 0.5 6.6 22. Adverse drug reaction 230 (1.5) 14.4 59.4 [Test result] 23. Health care–associated infection 351 (2.4) 15.0 43.8 24. Decrease in hemoglobin or hematocrit of 25% or greater 917 (6.2) 26.2 28.9 25. Hypoglycemic symptom 185 (1.2) 5.0 27.2 26. Bleeding tendency 52 (0.3) 2.0 32.6 27. Rising BUN or serum creatine >2 times baseline 441 (3.0) 9.5 19.3 28. Clostridium difficile–positive stool 70 (0.5) 4.0 63.8 [Related surgery] 29. Postoperative troponin level greater than upper normal limit 14 (0.1) 0.7 45.5 30. Mechanical ventilation >24 h postoperatively 14 (0.1) 1.1 80.0 31. Unplanned return to the operating theater 36 (0.2) 2.4 64.3 32. Unplanned removal, injury, or repair of organ during surgery 2 (0.0) 0.1 50.0 33. Intraoperative epinephrine, norepinephrine, naloxone, or romazicon 127 (0.9) 2.8 22.1 34. Unplanned change in procedure or surgery 22 (0.1) 0.7 29.4 35. Intubation, reintubation, BiPap in postanesthesia care unit 2 (0.0) 0.0 0.0 36. X-ray in postanesthesia care unit 1 (0.0) 0.0 0.0 [Obstetrics and neonates] 37. β2 Agonist use in obstetrics 0 (0.0) — — 38. Oxytocic agents in obstetrics 116 (0.8) 0.3 3.1 39. Complications of neonatal, abortion, amniocentesis or labor and delivery 0 (0.0) — — [Others] 40. Documentation or correspondence indicating litigation, dissatisfaction 49 (0.3) 1.6 28.6 41. Any other undesirable outcomes not covered above 125 (0.8) 7.9 51.3 Total 14,871 (100.0) — 17.9In stage 1, the overall percents of agreement were 81.9% when all negatives from the 2 reviewers were included and 67.3% when all negatives from the 2 reviewers were excluded (Table 2). Here, the κ value was 0.64 (95% confidence interval [CI], 0.61–0.66). By institution, the minimum and the maximum percents of agreement when all negatives were included were 62.0% and 95.0%, respectively; when all negatives were excluded, the minimum and the maximum overall percents of agreement were 48.2% and 84.1%, respectively. In stage 2, 83.7% of cases were a perfect match, and 87.4% were a partial match (Table 3). The κ values were 0.159 (95% CI, 0.12–0.20) and 0.389 (95% CI, 0.35–0.43), respectively. By institution, the percentage of perfect matches ranged from 57.8% to 97.5%, and the percentage of partial matches ranged from 73.0% to 98.7%.
TABLE 2 - Reliability of First Reviewers by Medical Institution Medical Institution Overall Percent Agreement (Including All Negative Findings) Overall Percent Agreement (Excluding All Negative Findings) κ Value 95% CI A 92.4 83.4 0.84 0.76–0.93 B 62.0 48.2 0.31 0.24–0.38 C 90.8 68.9 0.75 0.67–0.84 D 85.8 76.1 0.72 0.63–0.80 E 86.0 74.2 0.72 0.63–0.81 F 71.4 49.6 0.42 0.34–0.51 G 74.4 59.2 0.49 0.41–0.58 H 83.8 64.8 0.66 0.57–0.74 I 78.6 68.8 0.57 0.48–0.65 J 83.0 63.4 0.64 0.56–0.73 K 83.2 70.2 0.66 0.58–0.75 L 85.4 76.2 0.71 0.62–0.79 M 72.0 49.6 0.45 0.37–0.53 N 95.0 84.1 0.88 0.79–0.97 O 84.0 81.0 0.57 0.49–0.65 Total 81.9 67.3 0.64 0.61–0.66*Agreement in all of the opinions for the occurrence of an adverse event, the degree of harm, the causality, and the preventability.
†Agreement on the decision for adverse event but disagreement in the degree of harm, causality, or preventability.
The mean quality assessment scores were 3.18 of 4 points in stage 1 and 3.05 of 4 points in stage 2 (Table 4). By institution, the minimum and maximum scores in stage 1 were 2.93 and 3.52, respectively, and the scores in stage 2 were 2.72 and 3.30, respectively. The main reason for a negative assessment in stage 1 was insufficient description for identifying patient condition and inadequate medical records, incorrect entry on procedure and treatment, and differences in details between medical records. The majority of reviewers in stage 2 responded that identifying adverse events was difficult because of insufficient description of patient conditions and inadequate medical records.
TABLE 4 - Quality of Medical Record by Medical Institution Medical Institution First Stage Review, Mean ± SD Second Stage Review*, Mean ± SD A 3.12 ± 0.33 3.21 ± 0.41 B 2.93 ± 0.27 2.72 ± 0.48 C 3.06 ± 0.24 3.30 ± 0.56 D 3.51 ± 0.50 3.05 ± 0.38 E 3.10 ± 0.31 3.01 ± 0.11 F 3.37 ± 0.48 3.10 ± 0.37 G 3.06 ± 0.34 2.90 ± 0.30 H 3.52 ± 0.50 3.25 ± 0.46 I 3.00 ± 0.05 2.99 ± 0.11 J 3.00 ± 0.15 2.86 ± 0.37 K 3.39 ± 0.54 2.67 ± 0.50 L 3.02 ± 0.22 3.00 ± 0.00 M 3.48 ± 0.50 3.05 ± 0.21 N 3.24 ± 0.44 3.00 ± 0.00 O 3.00 ± 0.03 2.99 ± 0.11 Total 3.19 ± 0.42 3.05 ± 0.39*Detailed adverse event reports only.
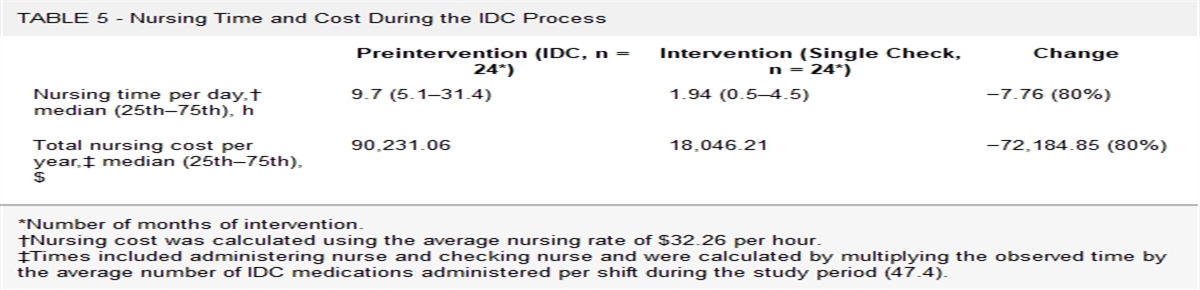
In stage 1, it took an average of 13.02 minutes to review one patient record, with a range of 6.35 to 52.50 minutes (Table 5). Regardless of the completion of a detailed adverse event report, the mean review time for in stage 2 was 5.06 minutes, with a range of 0.62 to 22.5 minutes. In addition, the time taken to complete a detailed adverse event report was 9.47 minutes on average, with a range of 3.39 to 29.04 minutes.
TABLE 5 - Review Time of First and Second Stage Review by Medical Institution Medical Institution First Stage Review, Mean ± SD Second Stage Review, Mean ± SD Detailed Adverse Event Reports, Mean ± SD A 7.98 ± 12.90 3.96 ± 45.23 9.57 ± 8.59 B 6.35 ± 8.18 4.50 ± 5.86 6.54 ± 5.48 C 8.46 ± 21.15 2.02 ± 3.73 7.18 ± 6.39 D 10.68 ± 21.83 0.68 ± 4.10 11.47 ± 10.51 E 12.57 ± 12.61 3.05 ± 5.22 7.17 ± 9.76 F 8.92 ± 17.30 0.57 ± 1.41 3.39 ± 1.66 G 9.54 ± 16.23 22.50 ± 31.56 29.04 ± 45.31 H 17.96 ± 30.82 2.87 ± 4.75 5.45 ± 5.44 I 16.75 ± 20.61 5.51 ± 18.19 20.01 ± 49.53 J 8.32 ± 6.92 5.41 ± 9.93 8.87 ± 7.58 K 6.84 ± 6.35 0.62 ± 2.42 6.44 ± 3.13 L 9.71 ± 9.98 3.65 ± 6.66 9.29 ± 5.05 M 16.43 ± 33.48 14.95 ± 41.84 18.00 N 52.50 ± 130.40 1.71 ± 3.00 6.30 ± 4.50 O 8.39 ± 11.03 2.22 ± 4.94 6.60 ± 4.36 Total 13.02 ± 37.63 5.06 ± 19.10 9.47 ± 20.12This study examined the feasibility of the KNPSII survey conducted in accordance with the Patient Safety Act of Korea. We examined the validity of the screening criteria, interreviewer reliability, medical record quality assessment, and the time taken for medical record review. For the method of reviewing medical records to identify adverse events to remain the criterion standard in examining patient safety status, it must be able to yield valid and reliable results; this study is significant in that it provides relevant comprehensive data about this.
In the first national-level KNPSII survey conducted in Korea, 41 screening criteria were used. This is greater than the 18 criteria used in Harvard Medical Practice Study–rel
留言 (0)