
記住我








This study will be a prospective equivalence randomized, double-blind controlled trial conducted in the department of surgery at Kampala International University Teaching Hospital (KIU-TH), western Uganda.
Study areaThe study will be conducted in KIU-TH in the operating theater and general surgery ward.
KIU-TH is a private nonprofit teaching hospital of Kampala International University located in Bushenyi district, south-western Uganda about 370 km from Kampala, the capital city of Uganda. The hospital has a bed capacity of 700. The hospital consists of outpatient departments (general and special), inpatient departments for surgery (general surgery and orthopedic), gynecology and obstetrics, internal medicine, and pediatrics. The department has five theater rooms with an average of 800 elective surgeries per year. The Department of General Surgery has 13 surgeons and 42 residents. There are 3 days per week for elective surgery. There are three anesthesiologists and six anesthetists. KIU-TH has a 4-bed intensive care unit (ICU) being managed by anesthesiologists.
Study populationAll patients were admitted to the surgical ward for elective hemorrhoidectomy during the study period.
Inclusion criteriaAll patients:
Aged between 18 and 65 years
Uncomplicated 3rd- and 4th-degree hemorrhoids
Classified by the American Society of Anesthesiologists (ASA) as I and II
Mixed hemorrhoids with a bulging external component
Exclusion criteriaAll patients with:
Contraindication of spinal anesthesia (chronic backache and spinal deformities)
Previous perianal surgery
A known history of allergy to local anesthetics
Bleeding disorders
Third- and 4th-degree thrombosed hemorrhoids
Active inflammatory bowel disease
Pregnant women
Documented neoplasm situated distal aspect of the large bowel or rectum
Liver diseases with portal hypertension
Failed anesthetic technique
Sample size determinationThe randomized control trial assumes a null hypothesis that the mean postoperative pain scores after hemorrhoidectomy using local anesthesia are not different from that done under saddle block by a clinically relevant amount. Since the primary outcome measure was a continuous variable (i.e., pain level measured using a visual analog scale), the formula for an equivalence design in randomized control trials by Zhong et al. [15] was used.
$$\boldsymbol=\mathbf\times }_-\propto}+}_-\boldsymbol}}}\right\}}^}\times }^}$$
where
Nsample size per group
Z1−αstandard normal deviate for a two-sided test used in equivalence trials (1.96 for 95% confidence interval)
δclinically admissible margin of equivalence design as a difference
αtype I error associated with rejecting the null hypothesis when it is true; (0.05) for 95% confidence interval
βtype II error associated with the alternative hypothesis, assumed to be 0.20 for a statistical power of 80%
(1−β)the probability of rejecting the null hypothesis when it is false, i.e., Z1−β = 0.845 for statistical power of 80%
S2pooled standard deviation of both comparison groups
According to a similar randomized control trial that compared open hemorrhoidectomy under local anesthesia versus supine anesthesia at the Korle Bu Teaching Hospital in Ghana [16], the difference in the mean pain scores between the 2 groups was δ = 0.73; pooled standard deviation in the mean pain scores S = 1.9 (average of 2.356 for local anesthesia and 1.479 for supine anesthesia), an estimated sample size of 104 participants per group, was obtained. Since at the time of the proposed study, nothing was known about the mean pain score following OH under local anesthesia and the real difference in clinical outcome between the two techniques in Uganda, the sample size was adjusted using Slovin’s formula as detailed by Ellen [17] based on the hospital records, Kampala International University Teaching Hospital which registered an average of 33 cases of grade 3 or 4 hemorrhoids in a period of 6 months that corresponded to the intended data collection period; thus, a sample size of 26 participants per group was obtained which was increased to 29 participants in each arm, based on a rate of 10% in each arm to compensate for the loss to follow-up and non-responsiveness found.
Study variablesPrimary outcome variableThe occurrence of pain following open hemorrhoidectomy will be determined in both groups using the area under the curve (AUC) for visual analog scale (VAS). The VAS will be used in an interval of 2, 4, and 6 h and 7 days postoperatively (the lower end of the scale labeled “0” means no pain while the upper end of the scale “10” signifies the worst imaginable pain).
Secondary outcome variableThe mean operative time from anesthesia induction to the end of open hemorrhoidectomy will be recorded in both groups.
Tertiary outcome variableThe tertiary outcome is the cost-effectiveness of the 2 surgical approaches in relation to the amount of materials used in the 2 arms.
Independent variablesData will be captured on preoperative independent variables such as gender, age, ASA level, and degrees of the hemorrhoids.
ConsentAny patient with third- and/or fourth-degree hemorrhoids aged above 18 years is eligible for this study and will be given an equal chance to participate and will be consented to by the principal investigator at the time of screening for eligibility.
Randomization and blindingAfter fulfilling the enrollment criteria and obtaining the informed consent, the participants will be allocated randomly by assistant researchers well trained to either the local anesthesia group (group A) or the saddle block group (group B) by using envelope allocation concealment whereby half of the envelopes will contain a chit with letter A while the other half will have a chit with letter B signifying local anesthesia and saddle block, respectively. The content of the envelope will be opened once the patient is in the theater, and the patients and outcome assessors will be blinded about the anesthesia.
Participant recruitment and study procedureParticipants will be recruited from surgical outpatient by trained research assistants. Patients with uncomplicated 3rd- or 4th-degree hemorrhoids will be assessed for study eligibility using a screening log. Written informed consent will be obtained from the eligible participants.
The patients admitted for elective hemorrhoidectomy will undergo pre-anesthetic evaluation the day before surgery and will be given fasting guidelines including 6 h for solid foods and 2 h to anesthesia for clear fluids like water. All patients will receive prophylactic antibiotics (intravenous 500 mg of metronidazole) within 60 min prior to incision [18]. Two hours before surgery, the patient will be receiving an enema intrarectal. All patients scheduled for surgery will be informed and admitted a day prior to surgery, prepared, and included in the theater program in order to maintain continuity of care.
Once in the operating room, vital signs will be taken (blood pressure, pulse rate, oxygen saturation, and monitoring of the ECG). Co-loading of intravenous crystalloids, namely normal saline and or ringers’ lactate, will be done using a restrictive approach of fluid administration and undergo open hemorrhoidectomy under saddle block [19].
Aseptic protocols will be observed for all groups. Group A patients, in lithotomy or prone jack-knife positions, will be infiltrated with bupivacaine 0.5% at a maximum safe dose of 2 mg/kg with adrenaline (1:200,000) following the technique of Jinjil et al. [20]. The local anesthetic mixture will be administered by the principal investigator as follows: The first two injections will be applied bilaterally (1 and 4), 5 mm from the border of the perianal skin, and the mixture will be injected at 12 and 6 o’clock (3 ml each side). Thereafter, further 4 injections will be administered into 4 quadrants performing a diamond shape (2, 3, 5, and 6), 5 mm from the anal opening; every 1 ml will be injected at a 4-cm, 3-cm, and 2-cm depth from the skin, respectively, as shown in Fig. 1.
Fig. 1
Local anesthesia infiltration [20]
With this technique, the mixture will fill the inter-sphincteric space and block the inferior rectal branch of the pudendal nerve (S2, S3) and the perineal branch of the 4th sacral nerve, causing paralysis of the external sphincter.
For group B patients, the back will be cleaned with 70% alcohol and draped while in a sitting position. The anesthetist or the anesthesiologist will identify the L4/L5 interspace by anatomical landmarks. Lidocaine will be infiltrated in the skin and subcutaneous tissue to form a wheel in the skin. A 25-G quincke spinal needle will be introduced into the sub-arachnoid space using either the midline or paramedian approach as deemed necessary by the anesthetist. Once the free flow of cerebrospinal fluid is observed in the hub of the needle, 1.5 ml of 0.5% bupivacaine will be administered. The patient will be kept in the sitting position for 10 min and thereafter placed in supine. Time 0 will be reordered once the cleaning of the back starts.
After the proof of the effect of anesthesia is administrated, participants in both groups will be put in lithotomy position, and the perianal region will be cleaned and draped before the beginning of open hemorrhoidectomy which will be done by the principal investigator. The technique for open hemorrhoidectomy will be as described by Milligan Morgan Clinic [21] after which dressing will be done, and this will be documented as a time finale.
Analgesia will be given according to the visual analog scale (VAS) once it is rated more than 4 by the patient at 2, 4, and 6 h for all patients irrespective of the type of anesthesia, and all participants will be discharged based on the post-anesthesia discharge scoring system (PADS) for determining home-readiness whereby the patient is judged fit for discharge when his score is ≥ 9 [22] and the 7th day assessment will be done after the patient is called back by the research assistants. Participants will be reassessed using the VAS on the 7th day postoperative. Diclofenac sodium 100 mg oral 8 hourly for 5 days will be considered as rescue analgesia postoperatively. All patients will be receiving a tablet of metronidazole 400 mg 8 hourly for the following five postoperative days.
The follow-up research assistants different from the recruiting team will collect the outcome data from patients at a stipulated time and enter it into a Microsoft Excel sheet up to the 7th day postoperative.
On the 7th day postoperative, the patients will be called back for review and follow-up assessment. Those who will not be able to come back to the hospital after discharge will be interviewed on a telephone call.
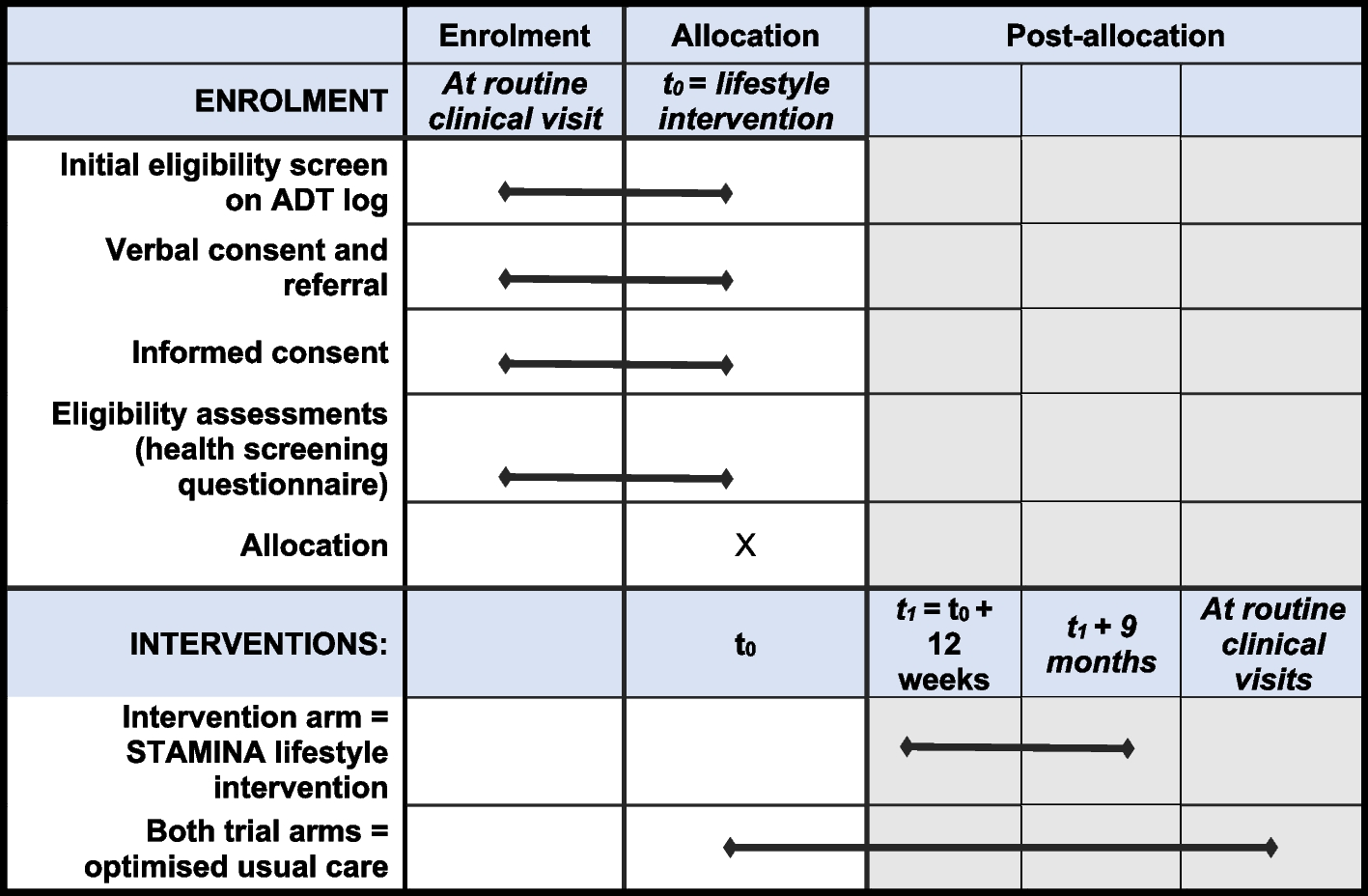
During both visits, detailed information will be obtained by the study doctor. The entire process from patient allocation to follow-up is displayed in Fig. 2 and well described in a Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) figure in Fig. 3.
Fig. 2
Flow chart of the trial process from allocation to follow-up at Kampala International University Teaching Hospital
Fig. 3
Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) figure of the trial schedule for enrollment, interventions, and follow-up/assessments at Kampala International Teaching Hospital
Interim analysisBiostatisticians will perform an interim analysis once we register a total of 36 patients for open hemorrhoidectomy using the two different anesthetic techniques, which is 62.1% of the planned number of patients. The primary, secondary, and tertiary outcomes will be evaluated to compare open hemorrhoidectomy using local anesthesia versus saddle block among patients with primary uncomplicated 3rd- and 4th-degree hemorrhoids.
The Data Monitoring Committee would recommend continuing, discontinuing, or modifying the trial, if concerns regarding the effect and safety of the participants will arise.
The recommendation to withdraw a patient from the trial will be decided by the principal investigator in case of failure of the anesthetic technique and loss of follow-up.
A recommendation of trial termination would be considered by the principal investigator, clinical trial institution, and ethics committee if achieving the difference in treatment effects is unlikely or if intolerable adverse effects occurred. The detailed results remain confidential to the investigator. The interim analysis was done on 10 March 2022, and continued recruitment was recommended.
Data processing and analysis planData will be statistically analyzed using IBM Statistics SPSS for Windows 23.0. The primary outcome will analyze all randomized patients (on an intent-to-treat (ITT) basis) and per-protocol (PP) population. The mean pain scores at rest and their standard deviations will be computed and compared using one-way ANOVA tests. VAS will be stratified as ordinal (0 as no pain, 1–3 as mild, 4–6 as moderate, and 7–10 as severe); the significance of the difference in the mean scores between local and saddle groups will be determined by the Kruskall-Wallis (H) test at 95% confidence interval, regarding p < 0.05 as statistically significant; furthermore, the mean pain scores will be analyzed for significant differences in the area under the curve (AUC) for VAS (2-sample t-test). The mean operative time and standard deviation will be computed for each technique of open hemorrhoidectomy. Cross tabulation will be performed between the two open hemorrhoidectomy techniques for categorical cost-effective analysis. The difference in the means will be compared using the t-test and their corresponding two-tailed p-value, regarding p < 0.05 as statistically significant.
Study durationThe study duration is a 6-month study period from 1 December 2021 to 31 May 2022. During this period, all participants will be followed up for a period of 7 days post-surgery. At the end of this trial, the result will be published in a peer-reviewed journal, and deidentified data set will be publically available to other researchers on a permanent web link that will be provided by a peer-reviewed journal.
Trial statusThe first case was recruited on 2 December 2021, and as of 7 April 2022, 45 patients were registered out of the required sample size of 58 for this protocol version 3 as of 21 May 2022.
Ethical considerationsThis clinical trial has been approved by the Kampala International University Research Ethics Committee (KIU-REC) under the number KIU-REC-2021-24. The standard official consent form for the Kampala International University Research and ethical review committee will be adopted. Respective hospital surgical consent forms conforming to WHO consenting information standards will be used, and oral translation to the local language will be done by the researcher or his delegated assistant. Participant recruitment will be done non-discriminatively regardless of race, color, or tribe. All those who meet the selection criteria will have equal chances of participating. The inclusion and exclusion criteria will be followed strictly. The trial will be overseen by the Institutional Research Ethics Committee (IREC) of Kampala International University.
Adverse eventsThere are minor discomforts anticipated in this study: pain associated with venipuncture during the process of blood collection for investigations which will be necessary as routine patient preparation for surgery. Patients are then expected to undergo pain and stress of hemorrhoids operation and bleeding after the operation. These discomforts are not imposed by the study but rather expected routine from patients who undergo such operations.
Ancillary and post-trial careThe outcome of the study may indirectly help participants to obtain care during study time and will be recognized during publications. Diverse outcomes, e.g., too much pain, will result in converting from local to SA (crossover) and getting other analgesics other than those prescribed in the trial.
Trial discontinuationThe trial will be discontinued for individual patients due to non-adherence, e.g., not completing the specified duration of follow-up, diverse outcomes, e.g., too much pain resulting in converting from local to GA (cross over) and getting other analgesics other than those prescribed in the trial.
UnblindingThe recommendation to withdraw a patient from the trial will be decided by the principal investigator in case of failure of the anesthetic technique and loss of follow-up. In addition to that, outcome assessors will be blinded, and the criterion for unblinding is if they observe adverse effects related to intervention that needs to be disclosed to the attending clinician.
Missing dataMissing data will be reported as missing during the analysis. Clinical characteristics of those lost to follow-up and crossovers will be compared to those retained in both groups.
留言 (0)