
記住我










Objective To identify factors associated with unplanned return visits to the emergency department (ED) among the population aged 75 years and older. Moreover, it aims to determine the association between patients’ access to primary care and unplanned return visits.
Design Data were collected from structured interviews, administrative databases, and medical charts at the index visits, and follow-up telephone calls were made at 3 months.
Setting Emergency departments of the 3 tertiary care hospitals in Montréal, Que.
Participants Community-dwelling patients aged 75 years and older.
Main outcome measures Zero-inflated negative binomial regression analysis was conducted of unplanned return visits within 3 months. Rate ratios (RRs) and odds ratios (ORs) with 95% CIs are presented.
Results During the study period, 4577 patients were identified, 2303 were recruited, and 1998 were retained for the analysis. Among the analysis sample, 33% were 85 and older, 34% lived alone, and 91% had a family physician. Before their ED visits, 16% of patients attempted to contact their family physicians. More than half of the patients reported having difficulty seeing their physicians for urgent problems, more than 40% had difficulty speaking with their family physicians by telephone, and more than one-third had difficulty booking appointments for new health problems. Within 3 months, 562 patients (28%) had made 894 return visits. Factors associated with a lower return visit rate included age 85 years and older (RR=0.80; 95% CI 0.67 to 0.96), less severe triage score (RR=0.83; 95% CI 0.74 to 0.92), and hospitalization at the index visit (RR=0.76; 95% CI 0.64 to 0.90). Factors that resulted in a higher return visit rate were difficulty booking appointments for new problems with their family physicians (RR=1.19; 95% CI 1.01 to 1.41), having had ED visits within the previous 6 months (RR=1.47; 95% CI 1.28 to 1.68), and higher Charlson comorbidity index scores (RR=1.06; 95% CI 1.01 to 1.11). Having had ED visits within the previous 6 months (OR=2.11; 95% CI 1.27 to 3.49), having a higher Charlson comorbidity index score (OR=1.41; 95% CI 1.19 to 1.68), and having received community care services (OR=3.00; 95% CI 0.95 to 9.53) also increased the odds of return visits.
Conclusion Although most people 75 years and older have a family physician, problems still exist in terms of timely access. Unplanned return visits to the ED are associated with having more comorbidities, having had previous ED visits, having already received community services, and having difficulty booking appointments with family physicians for new problems.
Worldwide it is reported that older persons are substantial users of emergency department (ED) medical services.1-5 In Canada, it is estimated that approximately 50% of those 75 years of age and older use emergency services.3 Moreover, compared with younger patients, older patients stay longer and have higher rates of ED visits, return visits, and hospital admissions.3,6
The number of unplanned ED return visits is an outcome often used as a measure of quality of care and is shown to be associated with increased functional decline or mortality.7 Research related to the magnitude of the problem, risk identification, and interventions to decrease recidivism is prevalent in the literature.8 However, a concern that has not received a lot of attention is how patient access to primary care resources may affect unplanned ED return visits.
Although it has been reported that 98% of older persons in Canada have a regular family doctor, their ability to get timely access in the form of a same-day or next-day appointment was among the lowest of 11 countries in the 2014 Commonwealth Fund International Health Policy Survey.9 Difficulty accessing primary care has been associated with higher or inappropriate ED use,10 while easy access has been associated with fewer ED visits, improvements in continuity of care, and greater patient satisfaction.11,12
This study primarily aims to determine the factors associated with unplanned return visits within 3 months of an index ED visit and, in particular, examine the association between patients’ access to primary care and unplanned return visits. Many research studies have focused on patients older than 65 years; however, as shown by the Canadian Institute for Health Information, the number of patients aged 75 and older is increasing at a faster rate; this population is expected to double between 2017 and 2037.13 Therefore, we chose to conduct this study among patients aged 75 years and older living in autonomous residences.
METHODSStudy design and settingThis is a multicentre prospective observational study conducted at 3 tertiary adult teaching hospitals in Montréal, Que. One hospital is affiliated with McGill University and has 73,985 annual ED visits, of which 16% were from patients 75 years and older. The other 2 French hospitals are affiliated with the University of Montréal and have annual ED visits of 29,711 and 43,119. Of these visits, 16% and 11% were from patients in this age range, respectively. Patient recruitment occurred from 2012 to 2014. Research committees from the participating hospitals approved this study.
Selection of participantsEligible patients were those 75 years and older visiting the EDs during the recruitment period, who lived in their own homes or in an autonomous residence (ie, for older persons who are physically and psychologically independent). Patients were excluded if they were unable to provide informed consent, they had a language barrier (ie, spoke neither English nor French), they were cognitively impaired, they failed the Short Portable Mental Status Questionnaire14 (defined as ≥5 errors out of 10), their visit was planned (eg, for imaging), or their visit led to prolonged hospitalization. Two research assistants worked on a predetermined schedule in the 3 hospitals to cover both weekday and weekend enrolment. The number of enrolment days at each site was proportional to the volume of patients 75 years and older at the specific site.
Date collection and outcomesOn the index ED visit, patients were asked to complete an index interview questionnaire. Three months later, patients were telephoned to respond to a follow-up questionnaire. All patient encounters were conducted in English or French. All unplanned return visits during the follow-up period were recorded; planned visits such as imaging, cast checks, dressing changes, direct referrals, and abnormal laboratory result follow-up were excluded.
Data were collected through patient interviews, medical chart reviews, and administrative databases (details in supplementary material, available from CFPlus*). The patients’ interview questionnaire included questions on access to health services, use of primary care services, perceived health status and living arrangements, the Barthel index of activities of daily living, and past medical history and health care resource utilization (to calculate the Identification of Seniors at Risk index and Charlson comorbidity index).15,16 We chose theIdentification of Seniors at Risk index out of many other screening risk tools because it is one of the most commonly used and it was developed in Canada. Patient demographic characteristics (eg, age, sex), clinical characteristics (eg, triage, arrival method), and discharge information (follow-up instructions) were obtained through medical charts or databases. At 3-month follow-up, patients were asked about their use of health care resources and any changes in living arrangement.
Return visit was the main outcome and it was measured in 2 ways: as a binary outcome (yes or no) and as a count outcome (the number of ED return visits within the 3 months before follow-up). This outcome was obtained from medical charts and from the follow-up questionnaire.
Sample sizeSample size was calculated with the aim of comparing return visits between patients who had difficulty accessing primary care versus those without difficulty. Based on literature and data from the participating hospitals, a 3-month return visit rate of 25% was expected. To detect a relative change of 25% (ie, an absolute change of 6.25% in return visit rate), at a significance level of .05 and with 80% power, 1622 patients would be required. Considering the correlation between primary care access variables versus other independent variables also associated with the outcome, we added a variance inflator of 1.15, resulting in a sample size of 1866 patients.
Data analysisDescriptive statistics (proportions; means with SDs) were used for the general characteristics of the patient population. Univariate analyses such as  2 tests, Student t tests, or Poisson regression with a single independent variable were used to select factors associated with the outcome variables (binary and count) at a significance level of P<.1. Then, selected factors were retained for multivariable analyses. Since distribution of the number of return visits showed both excess zeros and overdispersion, we therefore considered the zero-inflated Poisson model and zero-inflated negative binomial model as the multivariable analyses of choice.17 Different models were compared using the Lagrange multiplier statistic, the Akaike information criterion, or the Vuong test, as appropriate.18,19 Zero-inflated negative binomial regression was chosen as the best model, where the logit model part (by logistic regression analysis) estimates the probability of return to the ED (ie, no excess zeros), while the count model part (by negative binomial regression analysis) estimates the rate of return visits to the ED. Results are presented as odds ratios (ORs) and rate ratios (RRs) and their associated 95% CIs.
2 tests, Student t tests, or Poisson regression with a single independent variable were used to select factors associated with the outcome variables (binary and count) at a significance level of P<.1. Then, selected factors were retained for multivariable analyses. Since distribution of the number of return visits showed both excess zeros and overdispersion, we therefore considered the zero-inflated Poisson model and zero-inflated negative binomial model as the multivariable analyses of choice.17 Different models were compared using the Lagrange multiplier statistic, the Akaike information criterion, or the Vuong test, as appropriate.18,19 Zero-inflated negative binomial regression was chosen as the best model, where the logit model part (by logistic regression analysis) estimates the probability of return to the ED (ie, no excess zeros), while the count model part (by negative binomial regression analysis) estimates the rate of return visits to the ED. Results are presented as odds ratios (ORs) and rate ratios (RRs) and their associated 95% CIs.
During the study period 4577 patients aged 75 years and older who lived in autonomous residences were identified, of whom 41% were excluded and 9% declined to participate. Therefore, 2303 patients (50%) were recruited. At 3 months, 179 were deceased, 30 declined to continue participating, and 96 were withdrawn owing to loss to follow-up, transfer to other hospitals, admission to long-term care, or hospitalization in an acute care ward for more than 2 months following the index visit. Thus, 1998 patients (87%) were included in the data analysis (Figure 1). Within 3 months, 562 patients (28%) had revisited the ED for a total of 894 return visits (Figure 2).
 Figure 1.
Figure 1. Flowchart of study patient recruitment and sample derivation
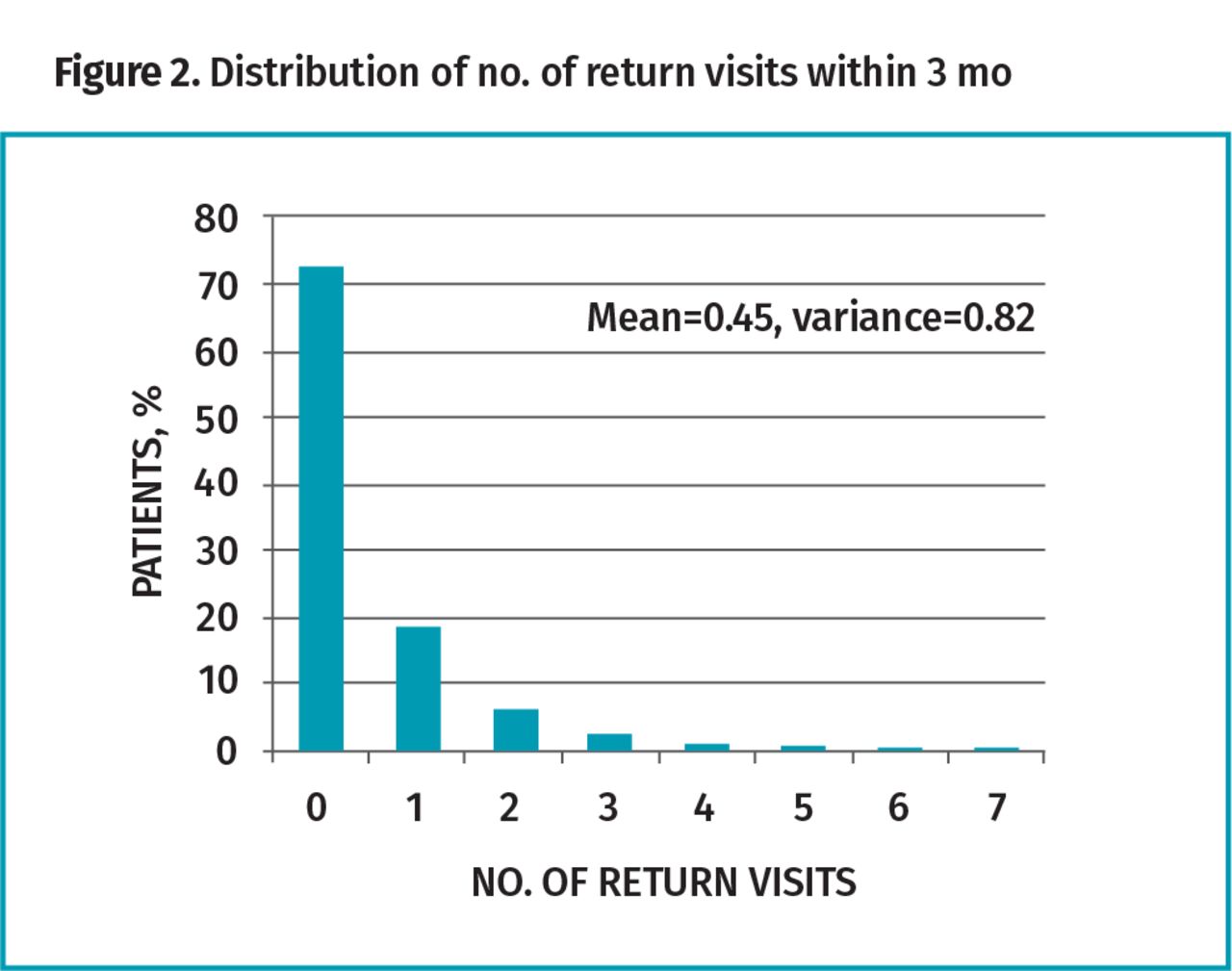 Figure 2.
Figure 2. Distribution of no. of return visits within 3 mo
Table 1 shows the independent variables separated into subgroups. These subgroups included factors related to patient characteristics, factors related to access to primary care services, and factors pertaining to the index ED visit. Variables with asterisks indicate statistically significantly differences related to return visits either by logistic regression (with the binary outcome of having had a return visit or no return visit) or Poisson regression analyses (with the count outcome of number of return visits). Although most patients had a family physician (91%), only 16% contacted their family physicians before going to the ED. In addition, more than 50% reported having had difficulty seeing their physicians for urgent problems, more than 40% had difficulty reaching their family physicians by telephone, and more than one-third had difficulty booking appointments for new health problems.
Table 1.Comparison of patients who returned to the ED vs those who did not return within 3 mo of the first ED visit: Percentages may not add to 100% owing to rounding.
For multivariable analysis, results from the zero-inflated negative binomial model are shown in Table 2. Table 2A shows factors that were associated with the number of return visits, while Table 2B shows factors that were associated with the binary outcome: having had a return visit or no return visit. Those who were 85 years or older (RR=0.80; 95% CI 0.67 to 0.96), had a lower-severity triage level (RR=0.83; 95% CI 0.74 to 0.92), or were admitted during the index visit (RR=0.76; 95% CI 0.64 to 0.90) had lower return visit rates. On the other hand, those who had difficulty booking appointments for new problems with their family doctors (RR=1.19; 95% CI 1.01 to 1.41), had ED visits within the previous 6 months (RR=1.47; 95% CI 1.28 to 1.68), or had a higher Charlson comorbidity index score (RR=1.06; 95% CI 1.01 to 1.11 for every 1-unit increase) had higher return visit rates. Factors that were associated with a higher likelihood of return visit were visits to the ED in the past 6 months (OR=2.11; 95% CI 1.27 to 3.49), increased Charlson comorbidity index score (OR=1.41; 95% CI 1.19 to 1.68 for every 1-unit increase), and having received help from local community services (OR=3.00; 95% CI 0.95 to 9.53).
Table 2.Multiple variable analysis (zero-inflated negative binomial model): A) Negative binomial regression to model return visit rate and B) logistic regression to model odds of return to the ED (excess zeros).
A comparison between patients in the analysis and patients withdrawn after enrolment (excluding death) showed that the 2 groups are similar (supplementary table available from CFPlus*) except that more patients in the withdrawn group lived in autonomous residences and arrived at the ED by ambulance. The reason could be a lack of family help for these patients.
DISCUSSIONOur study found the unplanned return visit rate is 28% among patients 75 years and older living autonomously. Other research looking at return visits within 90 days found that, for patients aged 65 years and older, the return visit rate is around 30%,20-25 while for patients 75 years and older, the return visit rate varies. For example, a Swiss study25 found a 38% return visit rate, while a French study observed a 10% return visit rate.26 This disparity may be due to differences in health care systems or hospital settings.
An important objective of this study was to understand how patient access to primary care might influence unplanned return ED visits. We measured a host of different factors to evaluate patients’ access to primary care services and found the following statistically significant associations. First, we found that for patients receiving community health services (eg, wound care by nurses), the odds of unplanned return visits increased 3-fold. This may be owing to patients’ poor baseline health status that required more health resources.27 Also contributing to an increased return visit rate was difficulty in accessing a family doctor for new problems (19% increased risk). This result agrees with a survey in the general population that difficulty with access to family doctors increases the use of emergency medical services.10,12
It is also worth noting that although most patients reported having a family physician, very few patients had contacted their family physicians before presenting to the ED. Apart from the fact that it is not easy to access primary care (more than half reported having difficulty seeing their physicians for urgent problems within 2 days and more than one-third had difficulty calling or booking appointments for new health problems), another potential reason could be that patients assumed that they would not be able to reach their family physicians at the time of their ED visits. In fact, 45% of patients arrived at the ED outside of regular office hours, ie, outside weekdays between 8:00 AM and 6:00 PM.
In addition, our study found that previous ED visits, higher comorbidity scores, and high severity of triage increased the risk of return visits. These findings are largely supported by the literature, mainly for those aged 65 and older.19,21,22,24 Within the same body of literature, only 1 study (targeting patients aged ≥65 years) stated that age is related to return visits, but in its analysis, age was determined a priori to be retained in the final model.20 In our analysis, we categorized patients into 2 groups: those aged 75 to 84 and those aged 85 and older; we found that patients aged 85 and older had a lower risk of revisiting the ED. Similar findings suggested that those 85 years and older are least likely to have short-term return ED visits (within 30 days) among patients aged 65 and older.5,7,28
Studies have shown there is an increasing trend in ambulatory care–sensitive conditions (ACSCs) among older patients visiting the ED,29 despite the definition of ACSCs not being suitable for use in the ED setting.30 Further research that investigates whether the patients at index ED visits and return visits can be classified as having ACSCs would be helpful in understanding the resources required in primary care and the importance of access to primary care.
Strengths and limitationsOur study has several important strengths. First, we recruited a large number of elderly patients from 3 different hospitals. Second, we recorded extensive amounts of reliable data from a variety of sources. For example, to ascertain patients’ comorbidities, we cross-checked this information using interview and medical charts.
One limitation of our study is that we excluded patients with language barriers. These patients may behave differently or be more likely to return to the ED owing to limited understanding of discharge instructions or difficulty communicating with their family physicians. A study funded by Health Canada suggests there is compelling evidence of the negative impact of language barriers on health care access and patient experience.31 Another limitation is that while many patients have been excluded or refused, we did not provide a comparison between enrolled and nonenrolled patients owing to the fact that there was not enough information about the nonenrolled patients.
ConclusionOur study revealed that although most elderly patients have a family physician, they do have difficulty in terms of access to care. In addition to patient characteristics and index visit–specific factors, difficulty in accessing primary care was associated with a higher rate of return visits to the ED within an elderly population. Therefore, community-based programs that target patient education and improved access to primary care are necessary not only for reducing return visits to the ED, but also for continuity of care and patient satisfaction.
NotesEditor’s key points▸ This study found the unplanned return emergency department (ED) visit rate is 28% among patients 75 years and older living autonomously.
▸ For patients receiving community health services (eg, wound care by nurses), the risk of unplanned return visits increased by 3-fold. Also contributing to an increase in return visit rate was the difficulty in accessing a family doctor for new problems (19% increased risk). Although most patients reported having a family physician, very few patients had contacted their family physicians before presenting to the ED. More than half reported having difficulty seeing their physicians for urgent problems within 2 days and more than one-third had difficulty calling or booking appointments for new health problems.
▸ Previous ED visits, higher comorbidity scores, and high severity of triage increased the risk of return visits. The analysis categorized patients into those aged 75 to 84 and those aged 85 and older; patients aged 85 and older had a lower risk of revisiting the ED.
Points de repère du rédacteur▸ Cette étude a constaté que le taux des visites de retour aux services d’urgence (à l’urgence) est de 28 % chez les patients de 75 ans et plus qui vivent de manière autonome.
▸ Chez les patients qui recevaient des services de santé communautaires (p. ex. soins d’une plaie par une infirmière), le risque d’une visite de retour non planifiée à l’urgence triplait. Les difficultés à accéder à un médecin de famille pour de nouveaux problèmes constituaient un autre facteur de l’augmentation du taux de visites de retour (augmentation du risque de 19 %). Même si la plupart des patients disaient avoir un médecin de famille, très peu d’entre eux avaient communiqué avec elle ou lui avant de se présenter à l’urgence. Plus de la moitié d’entre eux ont signalé avoir de la difficulté à voir leur médecin de famille pour des problèmes urgents dans les 2 jours suivant l’appel, et plus du tiers avaient des problèmes à parler au médecin ou à prendre rendez-vous pour de nouveaux problèmes de santé.
▸ Des visites antérieures à l’urgence, des scores de comorbidité plus élevés et une sévérité plus grande au triage augmentaient le risque d’un retour à l’urgence. L’analyse classait les patients entre les 75 à 84 ans et les 85 ans et plus; les patients de 85 ans et plus avaient le plus faible risque de retour à l’urgence.
Footnotes↵* Supplementary material on data collection is available from https://www.cfp.ca. Go to the full text of the article online and click on the CFPlus tab.
Contributors
Dr Marc Afilalo, Xiaoqing Xue, Antoinette Colacone, Dr Jean-François Boivin, Dr Roland Grad, and Dr Emmanuelle Jourdenais contributed substantially to the study conception and design, funding application, data acquisition, analysis, and result interpretation, and critically revised the manuscript for important intellectual content. Xiaoqing Xue performed the statistical analyses. Antoinette Colacone and Xiaoqing Xue drafted the manuscript; revised, edited, and prepared the manuscript for submission; and agree to act as guarantors of the work. All authors provided their approval of the final version of the manuscript.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Copyright © 2022 the College of Family Physicians of Canada
留言 (0)