
記住我

In the last three decades, a number of individual studies and meta-analyses have claimed that most antihypertensive drugs can be associated with an increased risk of a variety of neoplastic diseases [1–5]. This has not been confirmed by meta-analyses of randomized clinical trials or observational studies of longer duration, which have not seen any substantial antihypertensive drugs–cancer association or produced mechanistic evidence of its plausibility [6–8]. An exception, however, could be hydrochlorothiazide (HCTZ) as the reports that in the Danish population, the use of this drug was associated with an increased risk of non-melanoma skin cancers (NMSCs) [9,10], have been replicated in other populations and settings around the world [11–15], with few exceptions [16,17]. Furthermore, it has been observed that the association has a clear dose–response relationship, which supports a causal role of the drug, a conclusion that is further strengthened by the evidence, available already years ago, that HCTZ has photosensitizing effects [18–22]. This led the International Agency for research on Cancer to classify HCTZ as potentially carcinogenic in humans [23]. It has more recently led the European Medicines Agency and the US Food and Drug Administration to recommend updating the summary of product characteristics with safety warnings and advice on adequate ultraviolet (UV) protection in patients under HCTZ treatment [24,25].
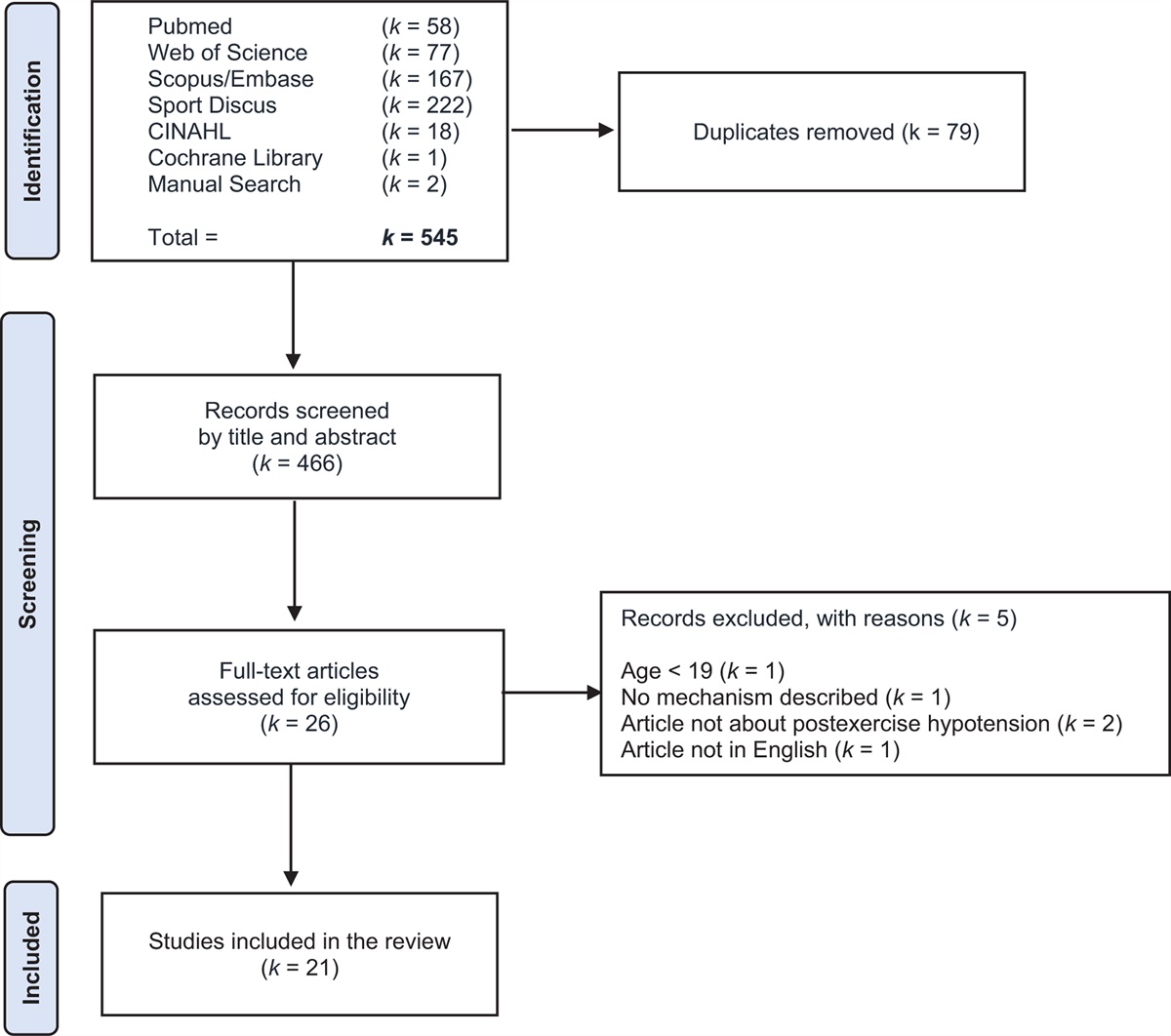
Thiazide/thiazide-like diuretics are commonly prescribed for lowering an elevated blood pressure and reduce hypertension-related cardiovascular events and death [26,27]. Their use markedly enhances the blood-lowering effect of all other drugs [28], for which reason, combinations that include diuretics are recommended by all hypertension guidelines to achieve blood pressure control in most hypertensive patients either after initial monotherapy or by some guidelines, as the initial treatment step [29–31]. The single pill combination of a thiazide diuretic, such as HCTZ at lower daily doses (12.5 or 25.0 mg) and a blocker of the renin–angiotensin system exceeds by far that of any other diuretic almost all over the world. After the reports from the Danish population, use of HCTZ dropped by 44% in Denmark, with even greater rates of discontinuation in younger patients [32]. Although numerical data are not available, a drop has probably occurred in other countries as well. This may seriously undermine the available therapeutic means to fight a condition, which is ranked as the first cause of death and burden of diseases worldwide [33], emphasizing the need for further studies not only on the carcinogenic risk of this drug but also on the mechanisms of this effect, its predictability in different patients, and the safety boundaries within which the drug can be used. We have recently added information on this issue, by setting up an experimental model that did not limit the observation to acute effects but mimicked the actual human exposure consisting of long-lasting HCTZ exposures and multiple UV irradiations. Human keratinocytes (HaCaT) were irradiated twice a week for 9 weeks with UVA (10 J/cm2) in the presence or absence of HCTZ (70 ng/ml) and compared with untreated cells or to cells exposed only to HCTZ. To establish a model with translational relevance for human exposure, the UVA dose applied approximated a human exposure of approximatively 1 h of midsummer sun [34], and in the absence of data on skin levels, the concentration was selected on the basis of the average human plasma levels after oral administration of 12.5 mg of HCTZ [35,36]. We demonstrated that the chronic combined exposure to UVA and HCTZ induced dysplastic changes in human keratinocytes, increased genotoxic damage, apoptosis resistance and inflammation, and activated the oncogenic pathway Wnt, thus reproducing some of the molecular alterations observed in human NMSCs [37] (Fig. 1). It was also clear that in absence of UVA, HCTZ did not exert any pro-carcinogenic effect. This adds to current knowledge of the steps through which HCTZ increases at cellular level the risk of NMSCs and further shows that in absence of UVA, the drug is well tolerated and that this is most likely the case if exposure to UVA is avoided by appropriate photoprotective measures, a principle that applies, however, not only to HCTZ users but also to the general population. Finally, this work emphasizes that a bidirectional research approach that integrates clinical data with experimental evaluations might be valuable to understand the biological plausibility of epidemiological observations, including those related to drug safety. This was also well exemplified by the studies exploring the link of thiopurines and voriconazole with skin cancer [38,39].
 FIGURE 1: Schematic representation of the pro-photo-carcinogenic effects of hydrochlorothiazide proposed. Data from [37]. The chronic, combined treatment with UVA and HCTZ, but not with HCTZ alone, induces dysplastic changes in human keratinocytes characterized by increased DNA damage and inflammation, defective DNA repair, the activation of the oncogenic pathway Wnt, apoptosis resistance and clonogenic potential [37]. Inserted photomicrographs show hematoxylin–eosin-stained keratinocytes with a round-shaped morphology before treatment; after chronic treatment with UVA and HCTZ, a pseudoepithelial morphology and dysplastic features are observed (scale bar 50 μmol/l).
FIGURE 1: Schematic representation of the pro-photo-carcinogenic effects of hydrochlorothiazide proposed. Data from [37]. The chronic, combined treatment with UVA and HCTZ, but not with HCTZ alone, induces dysplastic changes in human keratinocytes characterized by increased DNA damage and inflammation, defective DNA repair, the activation of the oncogenic pathway Wnt, apoptosis resistance and clonogenic potential [37]. Inserted photomicrographs show hematoxylin–eosin-stained keratinocytes with a round-shaped morphology before treatment; after chronic treatment with UVA and HCTZ, a pseudoepithelial morphology and dysplastic features are observed (scale bar 50 μmol/l).An important but unfortunately unanswered question is whether HCTZ can be replaced by other drugs [40] with similar blood pressure-lowering mechanisms to preserve the multimechanistic approach that makes combination treatment particularly effective [41]. As photosensitivity is not a unique feature of HCTZ, carcinogenic influences may in principle not be excluded also for other thiazides or thiazide-like antihypertensive drugs [42]. However, human and experimental studies in the field are scarce. The thiazide bendroflumethiazide was phototoxic in a cell culture model whereas chlortalidone and indapamide did not induce phototoxicity in this assay [43]. Case–control studies in Denmark and UK showed that the thiazide-like indapamide was not associated with NMSCs but with an increased risk of malignant melanoma [9,44,45] whereas bendroflumethiazide was not associated with the risk of any type of skin cancer [8,9,46]. To our knowledge, whether the thiazide-like diuretic chlorthalidone increases the risk of skin cancer is still to be determined. Additional pharmaco-epidemiological studies as well as experimental pharmacological evidence for or against the photocarcinogenic effects of other thiazide or thiazide-like antihypertensive drugs would be valuable.
To date, health authorities do not recommend stopping HCTZ as the risk–benefit is in favor of the cardiovascular benefits but recommend patients taking HCTZ to be informed of the risk of NMSC and to regularly check their skin, limit UV exposure and use adequate protections [24,25]. Health authorities also recommend that in patients with history of skin cancer, the use of HCTZ may be reconsidered [24].
In conclusion, in line with the recommendation of health authorities, for patients under appropriate blood pressure control with HCTZ, the switch to other treatments, whose pro-photocarcinogenic effects are not yet well established, should be carefully evaluated on the basis of the risk–benefit ratio.
ACKNOWLEDGEMENTS Conflicts of interestThere are no conflicts of interest.
REFERENCES 1. Pahor M, Guralnik JM, Salive ME, Corti MC, Carbonin P, Havlik RJ. Do calcium channel blockers increase the risk of cancer? Am J Hypertens 1996; 9:695–699. 2. Lin SY, Lin CL, Lin CC, Hsu WH, Lin CD, Wang IK, et al. Association between Angiotensin-Converting Enzyme Inhibitors and Lung Cancer-A Nationwide, Population-Based, Propensity Score-Matched Cohort Study. Cancers (Basel) 2020; 12:747. 3. Largent JA, McEligot AJ, Ziogas A, Reid C, Hess J, Leighton N, et al. Hypertension, diuretics and breast cancer risk. J Hum Hypertens 2006; 20:727–732. 4. Sipahi I, Debanne SM, Rowland DY, Simon DI, Fang JC. Angiotensin-receptor blockade and risk of cancer: meta-analysis of andomized controlled trials. Lancet Oncol 2010; 11:627–636. 5. Xie Y, Xu P, Wang M, Zheng Y, Tian T, Yang S, et al. Antihypertensive medications are associated with the risk of kidney and bladder cancer: a systematic review and meta-analysis. Aging (Albany, NY) 2020; 12:1545–1562. 6. Copland E, Canoy D, Nazarzadeh M, Bidel Z, Ramakrishnan R, Woodward M, et al. Antihypertensive treatment and risk of cancer: an individual participant data meta-analysis. Lancet Oncol 2021; 22:558–570. 7. Bangalore S, Kumar S, Kjeldsen SE, Makani H, Grossman E, Wetterslev J, et al. Antihypertensive drugs and risk of cancer: network meta-analyses and trial sequential analyses of 324,168 participants from randomised trials. Lancet Oncol 2011; 12:65–82. 8. Cho IJ, Shin JH, Jung MH, Kang CY, Hwang J, Kwon CH, et al. Antihypertensive drugs and the risk of cancer: a nationwide cohort study. J Clin Med 2021; 10:771. 9. Pedersen SA, Gaist D, Schmidt SAJ, Hölmich LR, Friis S, Pottegård A. Hydrochlorothiazide use and risk of nonmelanoma skin cancer: a nationwide case-control study from Denmark. J Am Acad Dermatol 2018; 78:673–681. 10. Pottegård A, Hallas J, Olesen M, Svendsen MT, Habel LA, Friedman GD, et al. Hydrochlorothiazide use is strongly associated with risk of lip cancer. J Intern Med 2017; 282:322–331. 11. Morales DR, Pacurariu A, Slattery J, Kurz X. Association between hydrochlorothiazide exposure and different incident skin, lip and oral cavity cancers: a series of population-based nested case-control studies. Br J Clin Pharmacol 2020; 86:1336–1345. 12. Daniels B, Pearson S-A, Vajdic CM, Pottegård A, Buckley NA, Zoega H. Risk of squamous cell carcinoma of the lip and cutaneous melanoma in older Australians using hydrochlorothiazide: a population-based case-control study. Basic Clin Pharmacol Toxicol 2020; 127:320–328. 13. León-Muñoz LM, Duarte-Salles T, Llorente A, Díaz Y, Puente D, Pottegård A, et al. Use of hydrochlorothiazide and risk of skin cancer in a large nested case-control study in Spain. Pharmacoepidemiol Drug Saf 2021; 30:1269–1278. 14. Eworuke E, Haug N, Bradley M, Cosgrove A, Zhang T, Dee EC, et al. Risk of nonmelanoma skin cancer in association with use of hydrochlorothiazide-containing products in the United States. JNCI Cancer Spectr 2021; 5:kab009. 15. Adalsteinsson JA, Muzumdar S, Waldman R, Hu C, Wu R, Ratner D, et al. Association between hydrochlorothiazide and the risk of in situ and invasive squamous cell skin carcinoma and basal cell carcinoma: a population-based case-control study. J Am Acad Dermatol 2021; 84:669–675. 16. Gallelli L, Cione E, Siniscalchi A, Vasta G, Guerra A, Scaramuzzino A, et al. Is there a link between nonmelanoma skin cancer and hydrochlorothiazide? Curr Drug Saf 2021; [Epub ahead of print]. 17. Pottegård A, Pedersen SA, Schmidt SAJ, Lee CN, Hsu CK, Liao TC, et al. Use of hydrochlorothiazide and risk of skin cancer: a nationwide Taiwanese case-control study. Br J Cancer 2019; 121:973–978. 18. Gómez-Bernal S, Alvarez-Pérez A, Rodríguez-Pazos L, Gutiérrez-González E, Rodríguez-Granados MT, Toribio J. Photosensitivity due to thiazides. Actas Dermosifiliogr 2014; 105:359–366. 19. Selvaag E, Petersen AB, Gniadecki R, Thorn T, Wulf HC. Phototoxicity to diuretics and antidiabetics in the cultured keratinocyte cell line HaCaT: evaluation by clonogenic assay and single cell gel electrophoresis Comet assay. Photodermatol Photoimmunol Photomed 2002; 18:90–95. 20. Selvaag E, Anholt H, Moan J, Thune P. Inhibiting effects of antioxidants on drug-induced phototoxicity in cell cultures. Investigations with sulphonamide-derived oral antidiabetics and diuretics. J Photochem Photobiol B 1997; 38:88–93. 21. Selvaag E, Thune P. Phototoxicity to sulphonamide-derived oral antidiabetics and diuretics: investigations in hairless mice. Photodermatol Photoimmunol Photomed 1997; 13:4–8. 22. Kunisada M, Masaki T, Ono R, Morinaga H, Nakano E, Yogianti F, et al. Hydrochlorothiazide enhances UVA-induced DNA damage. Photochem Photobiol 2013; 89:649–654. 23. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Some Drugs and Herbal Products. Lyon (FR): International Agency for Research on Cancer; 2016. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 108.) Available at https://www.ncbi.nlm.nih.gov/books/NBK350406/ 25. Food and Drug Administration. FDA Advisory No. 2019–328. Safety information: risk of nonmelanoma skin cancer with prolonged use of hydrochlorothiazide. Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-label-changes-hydrochlorothiazide-describe-small-risk-nonmelanoma-skin-cancer. 26. Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension: 4. Effects of various classes of antihypertensive drugs--overview and meta-analyses. J Hypertens 2015; 33:195–211. 27. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016; 387:957–967. 28. Mancia G, Rea F, Corrao G, Grassi G. Two-drug combinations as first-step antihypertensive treatment. Circ Res 2019; 124:1113–1123. 29. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018; 71:e127–e248. 30. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens 2018; 36:1953–2041. 31. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of hypertension global hypertension practice guidelines. Hypertension 2020; 75:1334–1357. 32. Pottegård A, Bech BH, Pedersen SA, Christensen B. Use of hydrochlorothiazide in Denmark following publication of skin cancer risk findings. Pharmacoepidemiol Drug Saf 2021; 30:1611–1616. 33. Zhou B, Perel P, Mensah GA, Ezzati M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol 2021; 18:785–802. 34. Jeanmougin M, Civatte J. Dosimétrie du rayonnement ultra-violet solaire. Variations journalières et mensuelles à Paris [Dosimetry of solar ultraviolet radiation. Daily and monthly changes in Paris]. Ann Dermatol Venereol 1987; 114:671–676. 35. Beermann B, Groschinsky-grind M. Antihypertensive effect of various doses of hydrochlorothiazide and its relation to the plasma level of the drug. Eur J Clin Pharmacol 1978; 13:195–201. 36. Beermann B, Groschinsky-Grind M. Pharmacokinetics of hydrochlorothiazide in man. Eur J Clin Pharmacol 1977; 12:297–303. 37. Bigagli E, Cinci L, D’Ambrosio M, Nardini P, Portelli F, Colucci R, et al. Hydrochlorothiazide use and risk of nonmelanoma skin cancers: a biological plausibility study. Oxid Med Cell Longev 2021; 2021:6655542. 38. Ikeya S, Sakabe JI, Yamada T, Naito T, Tokura Y. Voriconazole-induced photocarcinogenesis is promoted by aryl hydrocarbon receptor-dependent COX-2 upregulation. Sci Rep 2018; 8:5050. 39. O’Donovan P, Perrett CM, Zhang X, Montaner B, Xu YZ, Harwood CA, et al. Azathioprine and UVA light generate mutagenic oxidative DNA damage. Science 2005; 309:1871–1874. 40. Hollestein LM, Arnspang Pedersen S. Increased cutaneous squamous cell carcinoma risk with hydrochlorothiazide use: is there a safe alternative? Br J Dermatol 2021; 185 (2):244–245. 41. Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. Am J Med 2009; 122:290–300. 42. Kreutz R, Algharably EAH, Douros A. Reviewing the effects of thiazide and thiazide-like diuretics as photosensitizing drugs on the risk of skin cancer. J Hypertens 2019; 37:1950–1958. 43. Selvaag E. Cell cultures in the investigation of thiazide phototoxicity. Naunyn Schmiedebergs Arch Pharmacol 1997; 356:293–296. 44. Schneider R, Reinau D, Stoffel S, Jick SS, Meier CR, Spoendlin J. Risk of skin cancer in new users of thiazides and thiazide-like diuretics: a cohort study using an active comparator group. Br J Dermatol 2021; 185:343–352. 45. Jensen AØ, Thomsen HF, Engebjerg MC, Olesen AB, Sørensen HT, Karagas MR. Use of photosensitising diuretics and risk of skin cancer: a population-based case-control study. Br J Cancer 2008; 99:1522–1528. 46. Pottegård A, Pedersen SA, Schmidt SAJ, Hölmich LR, Friis S, Gaist D. Association of hydrochlorothiazide use and risk of malignant melanoma. JAMA Intern Med 2018; 178:1120–1122.
留言 (0)