
記住我







Background: There is no consensus on the most effective treatments of pulmonary arterial hypertension (PAH). Our objective was to compare effects of medications for PAH.
Methods: We searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials and Clinicaltrials.gov from inception to December 2021. We performed a frequentist random-effects network meta-analysis on all included trials. We rated the certainty of the evidence using the Grades of Recommendation, Assessment, Development, and Evaluation approach.
Results: We included 53 randomised controlled trials with 10 670 patients. Combination therapy with endothelin receptor antagonist (ERA) plus phosphodiesterase-5 inhibitors (PDE5i) reduced clinical worsening (120.7 fewer events per 1000, 95% CI 136.8–93.4 fewer; high certainty) and was superior to either ERA or PDE5i alone, both of which reduced clinical worsening, as did riociguat monotherapy (all high certainty). PDE5i (24.9 fewer deaths per 1000, 95% CI 35.2 fewer to 2.1 more); intravenous/subcutaneous prostanoids (18.3 fewer deaths per 1000, 95% CI 28.6 fewer deaths to 0) and riociguat (29.1 fewer deaths per 1000, 95% CI 38.6 fewer to 8.7 more) probably reduce mortality as compared to placebo (all moderate certainty). Combination therapy with ERA+PDE5i (49.9 m, 95% CI 25.9–73.8 m) and riociguat (49.5 m, 95% CI 17.3–81.7 m) probably increase 6-min walk distance as compared to placebo (moderate certainty).
Conclusion: Current PAH treatments improve clinically important outcomes, although the degree and certainty of benefit vary between treatments.
IntroductionPulmonary arterial hypertension (PAH) is a serious, progressive lung disease characterised by pulmonary vascular angiopathy, resulting in progressive dyspnoea, exercise limitation and right ventricular (RV) failure leading to premature mortality [1]. Although PAH remains incurable and still carries an overall poor prognosis, the median survival has significantly increased from 2–3 years in untreated patients to more than 6–10 years, largely based on open-label, real-world evidence [1–3]. This is thought to be the result of the development and routine clinical use of multiple medications, as well as care organised through pulmonary hypertension centres with specific expertise.
The treatment landscape for PAH has changed dramatically over 20 years, with development of medications targeting three classical therapeutic pathways: endothelin receptor antagonists (ERAs), nitric oxide (NO)-cyclic GMP-phosphodiesterase-5 pathway-active medications, including phosphodiesterase-5 inhibitors (PDE5i) and soluble guanylate cyclase stimulators, as well as prostanoid analogues and prostacyclin receptor agonists (PRA). Moreover, other therapies have also been studied, including imatinib, selonsertib and sotatercept, targeted at novel biologic pathways of vascular and endothelial dysfunction. Randomised controlled trials (RCTs) of all these agents have reported clinical benefits, largely compared to placebo treatment, including improved symptoms, functional class and exercise capacity, and reduced clinical worsening. Clinical practice guidelines typically recommend the use of two or three medications in most patients, each targeting one of the three classical pathways in a combination therapy approach, depending on individual patient pulmonary hypertension and severity of RV failure and individual risk stratification [2, 4, 5]. However, guidelines do not provide specific recommendations regarding most effective and safest first- and second-line classes of medications, due in part to a paucity of head-to-head trials directly comparing these therapies.
Unlike conventional pairwise meta-analysis, network meta-analysis (NMA) is more appropriate for PAH treatment effects, as it allows for multiple comparisons across multiple treatments, including placebo, as it allows for head-to-head comparisons despite the lack of direct head-to-head trials. These analyses remain an important part of clinical practice guideline development in order to inform best clinical practice.
However, there have been significant disparities in the quality of evidence synthesis in past NMAs and conventional meta-analysis [6], as well as older methodology with lack of assessment of clinically significant benefits. We investigated the comparative effectiveness of both approved and investigational drug treatment for PAH using NMA, applying current Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) methods [7].
MethodsWe report this NMA in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis extension statement for reporting of systematic reviews incorporating NMAs [8]. We pre-registered a protocol on open science framework on 2 August 2021: https://osf.io/ver7a.
Search strategyWe searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials and Clinicaltrials.gov from inception to June 2021 and updated the search in December 2021. We did not include unpublished trials or data, including abstracts. Our search strategy is presented in supplementary material S1.
Study eligibilityWe included RCTs, including crossover trials, that randomised patients with any World Health Organization (WHO) group 1 PAH aetiology to one of the following treatments versus standard of care or placebo: biologics (imatinib, selonsertib, sotatercept), ERAs (ambrisentan, bosentan, macitentan), NO-cyclic GMP-phosphodiesterase-type 5 pathway-active medications, including PDE5i (sildenafil, tadalafil, vardenafil) and the soluble guanylate cyclase stimulator (riociguat), prostanoid analogues (epoprostenol, iloprost, treprostinil) and prostacyclin receptor agonists (ralinepag, selexipag). We included trials with a minimum of 8 weeks’ follow-up. We included trials that enrolled patients aged <18 years, but excluded trials that exclusively studied paediatric or neonatal populations. We did not exclude trials based on language or year of publication.
Study selectionWe worked independently and in duplicate to screen titles and abstracts of search records and subsequently the full texts of records deemed potentially eligible at the title and abstract screening stage. We resolved discrepancies by discussion, and when necessary, by third-party adjudication.
Data extraction and outcome assessmentUsing a pilot-tested data extraction form, we collected data independently and in duplicate on trial and baseline patient characteristics including age, sex, baseline functional status and the following outcomes: 1) clinical worsening (as defined by study authors); 2) all-cause mortality; 3) all-cause hospitalisations; 4) 6-min walk distance (6MWD); 5) change in New York Hospital Association (NYHA)/WHO functional class (FC) status; 6) cardiac output and/or index; and 7) severe adverse events (SAEs; as defined by study authors).
Risk of bias in individual studiesWe assessed the risk of bias independently and in duplicate using a revision of the Cochrane tool for assessing risk of bias in randomised trials (RoB 2.0; supplementary material S2) [9]. We rated outcomes of interest as 1) low risk of bias; 2) probably low risk of bias; 3) probably high risk of bias; or 4) high risk of bias, across the following domains: bias arising from the randomisation process; bias owing to departures from the intended intervention; bias from missing outcome data; bias in measurement of the outcome; and bias in selection of the reported results, including deviations from the registered protocol. We resolved discrepancies by discussion and, when not possible, through adjudication by a third party.
Data synthesisTo simplify comparison between drug classes, we grouped individual medications into nodes based on molecule and pathway targeted, except when the clinical sense was that the route of administration affected clinical efficacy (i.e. oral versus inhaled versus intravenous/subcutaneous prostanoids) (supplementary material S3).
We summarised the effect of interventions on dichotomous outcomes (e.g. mortality) using relative risks and corresponding 95% confidence intervals. For dichotomous outcomes, we also calculated the absolute risk difference per 1000 patients by multiplying the relative risk by the baseline risk. We assumed the baseline risk to be equal to the median risk in the pooled placebo arms across trials. For continuous outcomes, we calculated mean difference and 95% confidence intervals.
For all outcomes, we performed a frequentist random-effects NMA using the netmeta package in R 2.0 (https://github.com/guido-s/netmeta). An NMA is more comprehensive than a conventional pairwise (e.g. single active treatment versus placebo) meta-analysis, especially when there are multiple treatment options, in that it allows for multiple comparisons across multiple treatments, including placebo. The conclusions regarding the certainty of benefit for a particular medication “A” are based on an overall network estimate, which is a pooled estimate based on direct estimates (from direct evidence of the effects of treatment “A” in clinical trial data) and indirect estimates. The latter indirect estimates are derived from indirect evidence, based on the results of trials of other medications which all have a common comparator, such as placebo. In the collective PAH medication evidence base, many studies are available with the common comparator (e.g. out of 42 trials assessing effects of various treatments on clinical worsening, 35 were placebo-controlled). This inclusion of indirect evidence from multiple placebo-controlled RCTs of other medications improves the precision of overall network estimates for benefits of each medication relative to this summary “placebo” group that is pooled from the placebo arms of all included trials. The inclusion of head-to-head trials connecting treatment “A” with any other treatment (e.g. the REPLACE trial of riociguat versus PDE5i) provides additional indirect evidence and increases the precision of the overall network estimates for effect of treatment “A”. Most importantly in an NMA, the overall pooled network estimate from direct and indirect estimates permits clinical comparison of the effects of multiple medications against each other, regardless of the lack of direct head-to-head trials.
A frequentist NMA assumes specified heterogeneity, whereas a Bayesian method incorporates a degree of uncertainty in the estimation of heterogeneity, which may result in greater imprecision for the network estimates as compared to frequentist methods. Both are valid methods for conducting NMA, and a study that re-analysed multiple NMAs using both methods found no major differences between the two in terms of the direction of the treatment effect [10]. Based on prior experience, we chose a frequentist framework to reduce complexity of analysis [11–15]. Network plots were made using network map function using STATA (version 17.0; StataCorp, College Station, TX, USA) [16]. For direct comparisons, we also performed inverse variance random-effects and fixed-effect meta-analysis using restricted maximal likelihood estimator. We compared study heterogeneity using visual inspection of confidence intervals for overlap, the I2 statistic and Chi-squared test for pairwise comparisons, as well as for networks for each outcome. We considered I2 scores of 0–39% as unimportant, 40–60% as moderate, 60–75% as substantial and >75% as considerable heterogeneity [17]. When estimates were based ⩾10 studies, we assessed for publication bias by inspecting funnel plots and Egger's statistical test [18].
We performed pre-specified subgroup analysis by comparing trials at high or probably high risk of bias with trials at low or probably low risk of bias, and we assessed the credibility of the subgroup analysis if the estimate was statistically significant using the ICEMAN tool [19]. Supplementary material S4 presents more detail on specific terminology and explanation of the methods.
Judgements of the certainty of the evidenceWe used a minimally contextualised approach to assess the effects of each treatment on various outcomes and to rate the certainty of the evidence [20, 21]. Comparisons between treatments were determined by assessing whether the network point estimate for an effect exceeded the pre-specified minimally important difference (MID). When available, we sourced minimal clinically important differences (MCIDs) from the literature, e.g. 33 m for 6MWD [22]. As MCIDs are unavailable for other outcomes, we surveyed eight international pulmonary hypertension experts on proposed MIDs. Consensus thresholds for clinically significant effects of treatment included MIDs of 1% for mortality, 5% for clinical worsening and hospitalisation, 10% for change in NYHA/WHO FC, 0.5 L·min−1 for cardiac output, 0.3 L·min−1·m−2 for cardiac index and 5% for SAEs. For example, using this approach, for a drug to be effective in reducing hospitalisations, it would need to have a calculated absolute risk difference versus placebo of ⩾5%, regardless of the statistical significance (i.e. width of 95% CI). Conversely, a treatment may have a network estimated effect on an outcome that is statistically significant, but is judged ineffective because the estimate does not exceed the MID threshold.
We then assessed for certainty of the evidence independently and in duplicate using the GRADE approach for NMA [7]. The certainty of effect for each comparison and outcome were rated as high, moderate, low or very low, based on consideration of seven GRADE domains: risk of bias, inconsistency, indirectness, publication bias, intransitivity, incoherence (difference between direct and indirect effects) and imprecision. Thus, a treatment may be judged to have benefit because the network estimate of the effect on an outcome exceeds the MID threshold, but the certainty of the estimate is downgraded (e.g. from high to moderate) due to specific consideration of these other GRADE domains (e.g. risk of bias, imprecision). For all outcomes, we present the most credible estimates of treatment effectiveness compared to placebo, preferably from NMA, but instead may present direct pairwise estimates if this provides higher certainty.
In the NMA process, transitivity is a key assumption that study populations in different trials are sufficiently similar that a randomised subject would be eligible to receive any of the treatments being compared. For example, the transitivity assumption would be violated by a WHO functional class IV PAH patient being considered for lung transplant would be compared to a patient eligible for oral monotherapy. Such important effect modifiers that may violate transitivity were specifically considered, including aetiology of PAH, baseline WHO FC and 6MWD, and assessed using regression.
We report results using GRADE standard language summaries [23]. Supplementary material S4 presents additional details on GRADE, terminology relating to NMA and other methods for readers unfamiliar with these methods.
ResultsOur search yielded 5006 records, of which the full texts of 222 records were reviewed and 53 studies (10 670 patients) were eligible for analysis. Figure 1 presents more detail on the inclusion and exclusion of records.
 FIGURE 1
FIGURE 1 Preferred Reporting Items for Systematic Review and Meta-Analysis flow diagram for inclusion of randomised controlled trials. #: Cochrane Central Register of Controlled Trials.
Participants were predominantly female (78.7%); the median age was 49 years; however, 19 (35.8%) trials allowed for recruitment of patients aged <18 years, but did not routinely report the numbers enrolled [24–42]. We judged that <20% of recruited subjects were aged <18 years for all included trials. Most subjects were classified as NYHA/WHO FC 3 or 4. The most common aetiology of PAH was idiopathic/heritable, followed by connective tissue disease associated PAH. Table 1 and supplementary material S5 and S6 present details on trial and baseline subject characteristics [23–76].
TABLE 1Basic demographic and clinical characteristics of participants across trials of pulmonary arterial hypertension (PAH) treatments
For all outcomes, we present the most credible estimates (either from pairwise analysis or NMA) of drug effectiveness compared to placebo. Supplementary material S7 presents all direct and indirect estimates and their associated GRADE ratings. Given the number of analyses, we only present moderate to high certainty results. There was no evidence of incoherence in our analyses using node-splitting models in order to compare direct and indirect estimates. Nor was there evidence of intransitivity in our analysis.
Risk of biasThere were five trials at risk of bias due to the randomisation process; six at risk of bias due to deviations from the intended interventions; 11 at risk of bias due to missing data; three at risk of bias due to measurement of the outcomes; and none at risk of bias due to selective reporting. Supplementary material S8 presents our complete risk-of-bias assessments.
Network meta-analysisWe present the results of eight separate networks. Supplementary figure S1 presents the network diagrams for all outcomes other than clinical worsening (figure 2). The network geometry demonstrates that most treatments were connected directly to placebo/standard of care. Given only active comparators (either ERA or PDE5i) in the RCT of ERA+PDE5i, this combination was only indirectly connected to placebo via ERA and PDE5i. The credibility of such network estimates that have no direct comparisons to placebo (e.g. ERA+PDE5i) depends directly on the credibility of the direct estimates that connect them (i.e. ERA+PDE5i versus either ERA or PDE5i).
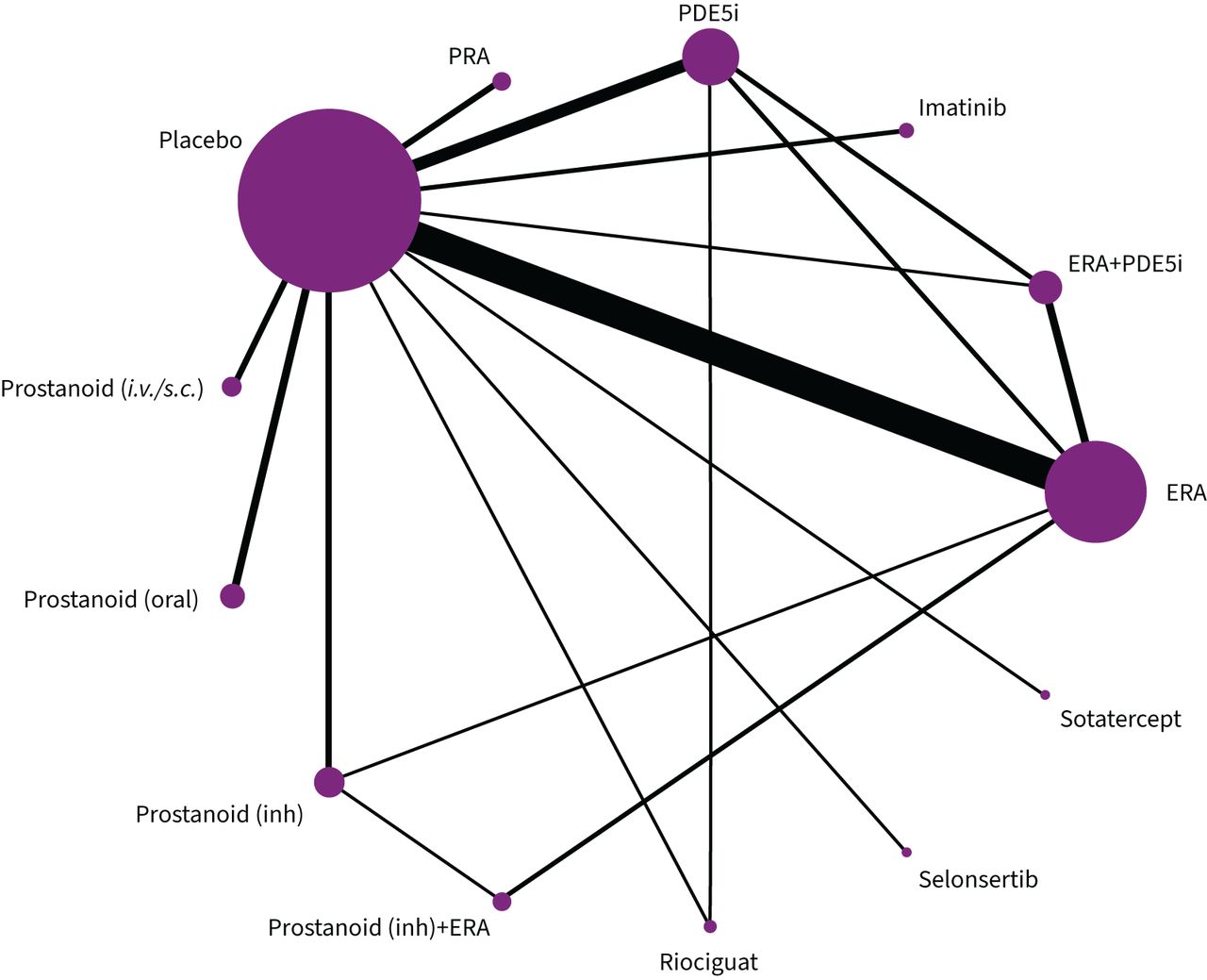 FIGURE 2
FIGURE 2 Network diagram for risk of clinical worsening in randomised controlled trials of pulmonary arterial hypertension treatments. Each node represents a drug or drug combination that has been tested in trials; the size of the nodes is proportional to the number of patients that have received that drug or drug combination; and the thickness of the connecting lines is proportional to the number of trials. PDE5i: phosphodiesterase-5 inhibitor; ERA: endothelin receptor antagonist; inh: inhalation; i.v.: intravenous; s.c.: subcutaneous; PRA: prostacyclin receptor agonist.
We found a range of heterogeneity estimates throughout the networks; however, the heterogeneity for most clinical outcomes was unimportant (including mortality and clinical worsening). The I2 for the NMA (mortality 0%, clinical worsening 32.7%, hospitalisation 14.6% and NYHA/WHO FC networks 32.8%) had unimportant heterogeneity. 6MWD (90.9%) had considerable heterogeneity, accounted for by the marked inconsistency of PDE5i and oral prostanoid versus placebo estimates. In addition, we found considerable heterogeneity in the cardiac index network (75.1%), owing to inconsistent estimates for ERA and intravenous prostanoids versus placebo. We took this into consideration when rating for inconsistency. The SAEs (45.1%) and cardiac output (64.3%) networks have substantial heterogeneity, owing largely to inconsistency in the direct estimates for several treatments (PDE5i, inhaled and oral prostanoids) versus placebo. We took this into account when rating for inconsistency.
Clinical worseningThe network addressing clinical worsening included 41 trials, comprising 9673 randomised patients, and reported 1744 clinical worsening events over a median follow-up of 16 weeks. Figure 2 presents the network geometry and figure 3 presents the forest plot.
 FIGURE 3
FIGURE 3 Forest plot for dichotomous outcomes. The vertical line indicates any effect. Figure 4 presents data in absolute effects with minimally important difference thresholds and Grades of Recommendation, Assessment, Development, and Evaluation ratings. ERA: endothelin receptor antagonist; PDE5i: phosphodiesterase-5 inhibitor; PRA: prostacyclin receptor agonist; inh: inhalation; i.v.: intravenous.
Several PAH-targeted medications reduced risk of clinical worsening as compared to placebo with high certainty. These include combination therapy with ERA+PDE5i (120.7 fewer events per 1000, 95% CI 136.8–93.4 fewer events per 1000), and monotherapy with riociguat (133.6 fewer events per 1000, 95% CI 151.3–85.3 fewer events per 1000), PDE5i (85.3 fewer events per 1000, 95% CI 107.9–51.5 fewer events per 1000) or ERA (75.7 fewer events per 1000, 95% CI 95.0–51.5 fewer events per 1000) as compared to placebo.
Head-to-head comparison of ERA+PDE5i combination therapy was identified as probably (moderate certainty) more effective than monotherapy with either ERA (37.7 fewer events per 1000 for ERA+PDE5i, 95% CI 50.7–17.4 fewer events per 1000) or PDE5i (36.3 fewer events for ERA+PDE5i, 95% CI 52.5–9.3 fewer events per 1000).
MortalityThe network addressing mortality consisted of 48 trials, including 10 336 patients, and reported 653 deaths over a median follow-up of 16 weeks.
PDE5i monotherapy probably reduces mortality as compared to placebo (24.9 fewer deaths per 1000, 95% CI 35.2 fewer to 2.1 more deaths per 1000); direct estimate. i.v./s.c. prostanoid analogues probably reduce mortality as compared to placebo (18.3 fewer deaths per 1000, 95% CI 28.6 fewer to 0 deaths per 1000). Riociguat probably reduces mortality as compared to placebo (29.1 fewer deaths per 1000, 95% CI 38.6 fewer to 8.7 more deaths per 1000) (all moderate certainty). Figure 3 presents the forest plot and figure 4 presents the estimates and GRADE ratings.
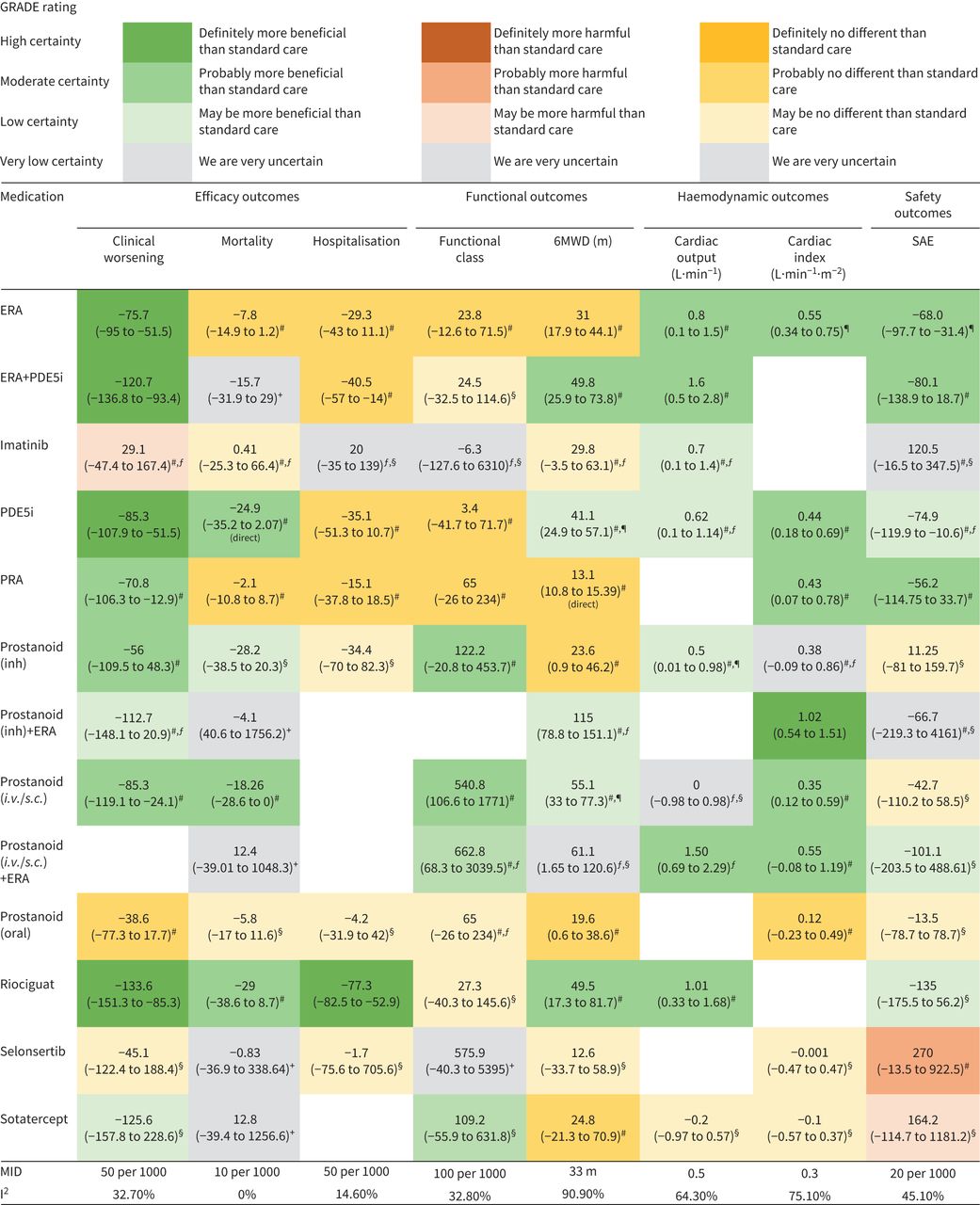 FIGURE 4
FIGURE 4 Network estimates of the effects of pulmonary arterial hypertension medications versus placebo on clinical and haemodynamic outcomes, presented in absolute risk difference per 1000 patients (95% CI); negative values indicate fewer events and positive values indicate more events per 1000. Colour arrangement reflects certainty of evidence. All estimates are network estimates unless otherwise specified. Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) working group grades of evidence are as follows. Interpretation: each node estimate is compared against placebo; the comparative effectiveness of a treatment on an outcome versus another treatment can be assessed by comparing respective cells; high certainty: we are very confident that the true effect lies close to that of the estimate of the effect; moderate certainty: we are moderately confident in the effect estimate (the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different); low certainty: our confidence in the effect estimate is limited (the true effect may be substantially different from the estimate of the effect); very low certainty: we have very little confidence in the effect estimate (the true effect is likely to be substantially different from the estimate of effect). 6MWD: 6-min walk distance; SAE: serious adverse events; ERA: endothelin receptor antagonist; PDE5i: phosphodiesterase-5 inhibitor; PRA: prostacyclin receptor agonist; inh: inhalation; i.v.: intravenous; s.c.: subcutaneous; MID: minimally important difference. GRADE rating: #: imprecision; ¶: inconsistency; +: rate down three times for imprecision; §: rate down twice for imprecision; ƒ: risk of bias.
HospitalisationsThe network addressing hospitalisations consisted of 26 trials, including 8084 patients, and reported 900 events over a median follow-up of 16 weeks. Riociguat reduced hospitalisations as compared to placebo (77.3 fewer events, 95% CI 82.5–52.9 fewer) (high certainty). None of the network estimates for any other treatment exceeded our pre-specified MID for hospitalisation. Figure 3 presents the forest plot and figure 4 presents the estimates and GRADE ratings.
6MWDThe network addressing 6MWD comprised 49 trials, including 9565 patients with a median follow-up of 16 weeks. Combination therapy with ERA+PDE5i (49.9 m, 95% CI 25.9–73.8 m) and riociguat monotherapy (49.5 m, 95% CI 17.3–81.7 m) both probably increase 6MWD as compared to placebo (moderate certainty). Figure 5 presents the forest plot.
 FIGURE 5
FIGURE 5 Forest plot for 6-min walk distance. The solid line indicates any effect; figure 4 presents data in absolute effects with minimally important difference thresholds and Grades of Recommendation, Assessment, Development, and Evaluation ratings. ERA: endothelin receptor antagonist; PDE5i: phosphodiesterase-5 inhibitor; PRA: prostacyclin receptor agonist; inh: inhalation; i.v.: intravenous.
Cardiac functionThe network addressing cardiac index included 22 trials with 2200 patients, whereas the network addressing cardiac output included 12 trials with 1362 patients.
Combination therapy with ERA+prostanoid(inhaled) improves cardiac index as compared to placebo (1.02 L·min−1·m−2, 95% CI 0.54–1.51 L·min−1·m−2; high certainty), and probably improves cardiac output (1.6 L·min−1, 95% CI 0.5–2.8 L·min−1; moderate certainty). ERA probably improves cardiac index (0.55 L·min−1·m−2, 95% CI 0.34–0.75 L·min−1·m−2) and cardiac output (0.8 L·min−1, 95% CI 0.1–1.5 L·min−1) as compared to placebo (both moderate certainty). PDE5i probably improves cardiac index as compared to placebo (0.44 L·min−1·min−2, 95% CI 0.18–0.69 L·min−1·m−2; moderate certainty). Riociguat probably improves cardiac output as compared to placebo (1.01 L·min−1, 95% CI 0.33–1.68 L·min−1; moderate certainty). Supplementary material S9 presents the forest plot.
Serious adverse eventsThe network addressing SAEs included 38 trials, with 8560 patients, and reported 2253 events over a median follow-up of 12 weeks. None of the United States Food and Drug Administration (FDA)-approved PAH treatments appeared to increase SAEs.
Both of the investigational treatments selonsertib (270 more events per 1000, 95% CI 14 fewer to 923 more events per 1000; moderate certainty) and sotatercept (164 more events, 95% CI 115 fewer to 1181 more events per 1000; low certainty) may increase the risk of SAEs as compared to placebo. Figure 3 presents the forest plot.
Subgroup analysisWe did not find any credible subgroup effect for studies at high/probably high risk of bias versus low/probably low risk of bias (p>0.05).
DiscussionMain findingsWe present the results of an NMA on all published RCTs of clinically relevant benefits of drug treatments for PAH over a median of 12–16 weeks, including FDA-approved and novel investigational treatments, using current GRADE methodology for reporting. High-certainty evidence indicates that combination therapy of ERA+PDE5i, as well as monotherapy with either riociguat, PDE5i or ERA reduce the risk of clinical worsening, with moderate-certainty evidence that ERA+PDE5i is more effective than either PDE5i or ERA alone. Only riociguat reduced hospitalisations with high certainty. There was moderate certainty that several PAH treatments improved survival, including monotherapy with PDE5i, riociguat or i.v./s.c. prostanoid analogues. It is noteworthy that the mortality estimates were not statistically significant in our analysis, being underpowered due to low event rates over median follow-up of only 12 weeks.
No treatment individually or in combination improved NYHA/WHO FC with moderate- to high-certainty evidence. Exercise capacity (6MWD) was probably improved by ERA+PDE5i combination therapy and riociguat monotherapy, and although ERA effect did not exceed MID for 6MWD, imprecision does not rule out benefit. Cardiac function (cardiac index or cardiac output) were probably improved by ERA+ prostanoid(inhaled), as well as monotherapy with ERA, PDE5i or riociguat.
In relation to other findingsOther NMAs of PAH treatments have been reported [77, 78]. A 2017 NMA presented data from 31 RCTs and found similar benefits of PAH treatments with regards to reduced clinical worsening [78]. No significant mortality benefit was reported in this published NMA, in contrast to our findings of moderate-certainty evidence for reduced mortality following monotherapy with riociguat, PDE5i and i.v./s.c. prostanoid analogues. Important limitations of the 2017 NMA include smaller database of included RCTs and outdated GRADE methodology (revised 2018). The present NMA benefits from a higher mortality event rate due to inclusion of additional recent trials, as well as methodological improvements and interpretation using the current GRADE reporting framework. Possibly for similar reasons, we also found that combination ERA+PDE5i therapy and riociguat probably improve 6MWD, exceeding the a priori 33 m MCID, whereas the previously published analysis had not identified any such benefit [78].
More recently, a Bayesian NMA published in 2021 did not report any absolute effects of treatments and did not use GRADE or any other method for assessment of the certainty of the evidence, making the results less meaningful for clinicians [77]. Furthermore, the reported creation of nodes, for example, grouping of all treprostinil treatments together regardless of the route of administration (e.g. oral versus i.v./s.c.) despite recognised efficacy differences, renders it difficult to discern which individual treatments may be beneficial.
Novel findingsThis NMA of the potential benefits of PAH treatments uses the current methodology for ascertainment of certainty of evidence and NMA reporting, as applied by an experienced methodologist. We recognise that previous NMAs were completed prior to this major guidance change to the reporting of NMAs [79], driven in part by appreciation that previous reporting was inconsistent with how end-users interpret and use the certainty of evidence in clinical decision-making. Moreover, the present NMA benefits from increased trial data and events, explicit therapeutic drug node classification, and assessment of MIDs for a broad range of clinically relevant outcomes, based on a consensus of PAH experts.
In addition, the present analysis is the first to report on comparative effectiveness of experimental biologic therapies versus FDA-approved treatments. For example, low-certainty evidence suggests that sotatercept may reduce clinical worsening in patients already on background PAH therapy (91% on double or triple pulmonary hypertension-targeted medications), but there was minimal evidence for any other clinically relevant benefits.
LimitationsA key limitation of such an NMA which includes RCTs from over 25 years is the significant heterogeneity of the PAH patient population, despite largely uniform clinical and haemodynamic definitions, such that modern global trials include patients from many countries and ethnic backgrounds, of broader, generally older age and with many PAH aetiologies [80]. This may affect the generalisability of our findings to all PAH patients, as may the heterogeneity between trials of definition of one of the key outcomes, clinical worsening [81]. Furthermore, most PAH RCTs are relatively short-term, assessing outcomes after 12–26 weeks of treatment, resulting in low event rates for some clinical outcomes, e.g. hospitalisation and mortality. Thus, the evidence base is likely to underestimate the potential beneficial effect of treatment on these outcomes, which may be better addressed by studies with longer follow-up.
Importantly, early trials of PAH treatments were in treatment-naïve patients, but the increasing availability of PAH treatments over the past 25 years has resulted in PAH trials typically enrolling subjects already receiving background standard-of-care PAH treatment, with recognised blunting of measurable clinical benefit, e.g. NYHA/WHO FC and 6MWD. We recognise that the inclusion of investigational medications in our analysis (i.e. sotatercept) may be premature, given the availability of only phase 2 trial data. Therefore, these results need to be interpreted with caution and the analysis requires updating once phase 3 trials are complete (NCT04576988, NCT04896008, NCT04811092, NCT04796337).
Our conclusions are necessarily limited by the evidence, specifically the number of studies investigating each treatment and the number and completeness of the assessment of clinically-relevant outcomes reported for those treatments. For example, although i.v. prostanoid analogues are widely accepted as one of the most effective PAH medications, evidence for their benefits derives from relatively few studies. As a result, our analysis concluded only moderate-to-low certainty evidence for benefit of i.v./s.c. prostanoid analogues across a spectrum of patient-relevant outcomes, in part because of lack of assessment and reporting (e.g. clinical worsening, hospitalisation).
Another current concern over the published PAH treatment evidence base is that none of the RCTs have assessed the effects of treatment on the risk status of individual patients, e.g. low, intermediate or high risk for mortality and other poor outcomes. This is an important information gap in supporting clinical practice, as current clinical practice guidelines strongly recommend that treatment should be guided by individual patient risk stratification based on multiparameter assessment of clinical, functional and haemodynamic measures [5, 81].
We also recognise potential methodological limitations of our analysis. Although undetected, there is potential for violation of the assumptions of NMA, including intransitivity. In addition, in the absence of published data on MIDs for several clinically relevant outcomes, potential MIDs were determined through a simplified consensus process of a small number of PAH experts. This approach may result in underestimation of the clinical effectiveness of PAH medications. For example, ERA, PDE5i and ERA+PDE5i were rated as having no effect in reducing hospitalisations, despite reducing hospitalisations by a risk difference of 2.9%, 3.5% and 4.5%, respectively. Clinicians and evidence users may reasonably determine more liberal thresholds as clinically relevant MIDs. Another methodological limitation includes the use of aggregate data to make conclusions in a heterogeneous population, whereas individual patient data meta-analysis would be able to investigate for more credible subgroups.
ConclusionUsing available aggregate RCT data and the most current GRADE methodology, this NMA found moderate-to-high certainty that current PAH treatments improve clinically relevant outcomes, including reduced clinical worsening and mortality, as well as improved 6MWD and cardiac function. However, the spectrum, degree and certainty of benefit vary between treatments, in part because the evidence base is limited by relatively small, largely placebo-controlled RCTs with few active treatment comparative trials, as well as heterogeneity of RCT study populations and comprehensiveness of outcome assessment. As such, given limitations in the evidence base as well as assumptions of NMA, we would emphasise caution in making firm conclusions about our findings of moderate-to-high certainty evidence of lack of effect of certain medications, without further context.
Overall, these data support current clinical practice guidelines recommendations for combination pulmonary hypertension-targeted therapy in most PAH patients, especially those at intermediate-to-high risk of future clinical worsening and premature mortality. Further research is essential to better understand the effects of PAH treatments on the current best measures of individual patient wellbeing and risk of poor long-term outcomes, specifically multiparameter risk assessment and RV function. We expect that integration of the evidence base summarised data from this analysis with real-world evidence and clinical experience may inform future clinical practice guidelines and clinical will inform decision-making for optimal care of PAH patients.
AcknowledgementsThe authors gratefully acknowledge the contributions of pulmonary hypertension expert colleagues Nathan Brunner (University of British Columbia, Vancouver, Canada), Murali Chakinala (Washington University, St. Louis, MO, USA), Sean Gaine (Mater Misericordiae, Dublin, Ireland), Naushad Hirani (University of Calgary, Calgary, Canada), Steeve Provencher (Laval University, Quebec, Canada), Jason Weatherald (University of Alberta, Edmonton, Canada).
留言 (0)