
記住我

Nursing homes and other long-term care facilities (LTCFs) in the United States have been disproportionately affected by COVID-19. Due to the congregate nature of LTCFs and the close and frequent contact between staff and residents, a largely vulnerable population of older adults with underlying medical conditions, SARS-CoV-2, the virus that causes COVID-19, can spread rapidly in these facilities, resulting in high morbidity and mortality.1,2 In response to the pandemic threat, the Centers for Medicare and Medicaid Services (CMS) required nursing homes to restrict visitation and resident movements starting in March 2020.3 Still, nursing home staff had to enter and leave and new residents were being admitted, remaining potential sources of SARS-CoV-2 introduction. As the pandemic progressed, LTCFs implemented additional infection prevention and control (IPC) measures, including routine testing of staff in August 2020,4 and COVID-19 vaccines in December 2020.5 As of September 2021, COVID-19 outbreaks had been reported in nearly all 15,600 nursing homes in the United States, resulting in more than 1.3 million confirmed cases and nearly 140,000 confirmed deaths among residents and staff.6,7 By March 2021, it was estimated that nearly 1 in 12 US residents of LTCFs had died from COVID-19.8
Reflecting these national trends, long-term care facility (LTCF) residents in Fulton County, Georgia, the most populous county in the state, comprising Atlanta and the surrounding metro area, were disproportionately affected by COVID-19, especially early in the pandemic. Despite accounting for <1% of the population, nearly 20% of cases and >50% of COVID-19 deaths in Fulton County occurred among LTCF residents between March and June 2020.9
Interventions in LTCFs (like masking and case isolation) aim to interrupt virus transmission. However, transmission is rarely observed directly and the transmission process of SARS-CoV-2 remains incompletely understood, especially in these settings. Therefore, a better quantitative understanding of transmission is critical. The reproduction number (R) and how it varies over time (R(t)) quantifies transmission and can be inferred from case counts and knowledge of a pathogen’s natural history.10 In this study, we used data on the timing and magnitude of COVID-19 cases in Fulton County LTCFs to examine temporal trends in SARS-CoV-2 transmissibility. Then, we aimed to identify characteristics of cases (resident or staff, vaccination status, and disease severity) associated with greater infectiousness.
METHODS DataWith the goal of inferring transmission patterns over time, we used surveillance data on COVID-19 cases curated by the state and county health departments. First, we used this dataset to infer how transmission varied over time, quantified as the time-varying reproduction number, R(t). Then, we linked these data with case characteristics, including vaccination status, to examine whether certain groups played a larger role in transmission. In collaboration with Fulton County Board of Health (FCBOH), we developed an analysis plan for a dataset derived from the Georgia Department of Public Health’s (GDPH) statewide COVID-19 surveillance data (i.e., the surveillance dataset). Deidentified, individual-level data were downloaded on September 12, 2021, and restricted to confirmed and probable cases reported March 2, 2020, to September 12, 2021 (eFigure 1; https://links.lww.com/EDE/B933). Cases with positive results from reverse-transcription polymerase chain reaction (RT-PCR) tests were classified as confirmed and cases lacking RT-PCR results but meeting other testing, clinical, epidemiologic, or vital records criteria (e.g., a positive antigen test with clinical/epidemiologic evidence) were classified as probable.11 Because cases outside of Fulton County could not be consistently linked to individual LTCFs, we focused our analysis on Fulton County. Data were restricted to cases associated with Fulton County facilities, including skilled nursing (SNFs, also known as nursing homes) and assisted-living facilities, using unique facility identifiers provided by FCBOH. To determine COVID-19 vaccination status of cases, we used data from the GDPH COVID-19 Vaccine Breakthrough Dashboard Dataset (i.e., the vaccine dataset), which were provided by FCBOH.
We categorized cases hospitalized at any time during their illness as hospitalized. We defined COVID-19 deaths as confirmed cases that were reported as deceased, had COVID-19 indicated as the cause of death on death certificates, or had evidence that COVID-19 contributed to death.11 If cases were missing information on COVID-19 death, we assumed they did not die from COVID-19 (eTable 1; https://links.lww.com/EDE/B933). When examining COVID-19 hospitalizations and deaths, we restricted data to cases with symptom onset dates before August 1, 2021, to account for lags in hospitalization and death.
We imputed missing symptom onset dates based on first positive specimen collection date, when available, or case report date (eFigure 4; https://links.lww.com/EDE/B933).12 We modeled the number of days between symptom onset and first positive specimen collection or case report date using negative binomial regression with the first positive specimen collection or case report date as the predictor (eFigures 5–6; https://links.lww.com/EDE/B933). For asymptomatic cases (n = 677), imputed symptom onset dates, which were needed to calculate R(t), can be interpreted as the time that they developed weak/negligible symptoms.
Case and Outbreak CharacteristicsWe considered the following variables in our study: LTCF role (resident or staff), vaccination status, hospitalization, and COVID-19 death. We determined facility role using a number of variables, including whether “Staff” was entered into free-text fields and age of cases (eFigure 2; https://links.lww.com/EDE/B933). We also conducted a sensitivity analysis in which we assumed that all cases missing “Staff” in free-text fields were residents, as FCBOH members were instructed to enter “Staff” for all staff cases, and to leave these fields blank for resident cases.
Using the surveillance and vaccine datasets, we categorized cases as vaccinated (n = 18) if they had received at least one vaccine dose ≥14 days before their first positive specimen collection date and had illness onset after December 31, 2020 (eFigure 3; https://links.lww.com/EDE/B933). Information on full or partial vaccination, vaccine manufacturer, and date of most recent dose was available for cases in the vaccine dataset. For fully vaccinated cases, we imputed the date of their first dose based on recommended vaccine dosing intervals.13 If cases were not in the vaccine dataset, but were listed as vaccinated in the surveillance dataset (n = 11, 61% of cases categorized as vaccinated), we categorized them as vaccinated. For these cases, we could not determine the number of doses received. Therefore, for all analyses, we classified both partially and fully vaccinated cases as “vaccinated” and could not examine partial and full vaccination status separately.
For the purposes of this analysis, we defined COVID-19 outbreaks as ≥2 reported case(s) of COVID-19 among residents or staff in a LTCF. If no new cases were reported for >14 days, the outbreak was considered to have ended. Singleton cases were defined as those with dates of onset 14 days before or after other cases in a facility. To fully investigate transmission, it is critical to include singleton and other nontransmitting cases, so these are included in all such analyses. Singleton cases and outbreaks are referred to collectively as “events.” The terms “cases” (singleton or outbreak-associated) and “outbreaks” have precise meanings and are used accordingly throughout the article.
Time Periods ExaminedTo examine trends in transmission, we divided the data into three periods corresponding to different waves of COVID-19: March 11–September 26, 2020 (wave 1), September 27, 2020–March 21, 2021 (wave 2), and March 22–September 12, 2021 (wave 3). We determined waves by visually examining Fulton County LTCF case counts by report date. We also considered the following dates: May 31, 2020 (shortly after states began lifting community pandemic restrictions and CMS released reopening guidelines for US nursing homes),14,15 August 31, 2020 (shortly after CMS began requiring routine COVID-19 testing of nursing home staff),4 and December 31, 2020 (shortly after the first COVID-19 vaccines were distributed to US nursing homes).5
SARS-CoV-2 Transmissibility and Case InfectiousnessWe quantified SARS-CoV-2 transmissibility using the time-varying reproduction number, R(t), which is the expected number of cases directly caused by a single infectious individual with symptom onset at time t. We estimated R(t) using a method originally developed by Wallinga and Teunis.10,16 This method estimates probabilities of transmission between any pair of cases in an outbreak using symptom onset dates and the distribution of the serial interval, defined as the time interval between symptom onset in a primary (infector) and secondary case (infectee). These probabilities are used to construct a number of epidemic trees, from which the mean and variance R(t) can be estimated.16 We constructed 1,000 epidemic trees for each outbreak. Rather than taking the mean and variance R(t), we created a total of 1,000 datasets, each of which contained R(t) estimates for all outbreaks from a single constructed epidemic tree. By creating these separate datasets, we were able to incorporate the uncertainty of R(t) estimates into regression results. We defined outbreaks based on symptom onset dates and considered them over if no new cases developed symptoms within 14 days of the last symptom onset date. We assumed outbreaks to be independent and completely enumerated, such that cases from different outbreaks could not infect one another and all individuals involved in transmission were captured. We assigned singleton cases a R(t) of 0. All cases in our dataset had symptom onset >14 days before data download, so right censoring could be ignored.17
A key input for estimating R(t) is the serial interval. The serial interval is the time between equivalent stages in the infection process (e.g., symptom onset) in successive pairs of cases, so is required to infer the likelihood that one person acquired infection from another. To estimate the serial interval, we examined known transmission pairs, identified by case interviews and contact tracing, of LTCF resident and staff cases in Georgia (eFigure 7; https://links.lww.com/EDE/B933). Transmission pairs with serial intervals <1 or >50 days were excluded. We identified a total of 184 known transmission pairs, from which the serial interval was estimated to follow a gamma distribution (mean = 8.0 days; SD = 6.9 days) using a maximum likelihood method.12 To examine the sensitivity of regression results to serial interval assumptions, we conducted two sensitivity analyses in which we used gamma serial interval distributions estimated by Zhang et al18 (mean = 6.2 days; SD = 3.6 days) and Wang et al12 (mean = 5.0 days; SD = 3.5 days) to calculate R(t). We also examined whether the serial interval distribution changed over time, and found no meaningful differences between time periods (eTable 2 and eFigure 8; https://links.lww.com/EDE/B933).
To examine temporal trends in R(t) among Fulton County LTCF cases, we plotted daily R(t) estimates with a locally estimated scatterplot smoothing (LOESS) trendline. Because R(t) naturally declines as events progress and individuals acquire immunity, only R(t) estimates for the first five event days (defined as symptom onset days for an individual event excluding days with no cases) were examined.
Next, to identify if there were characteristics of cases associated with heightened infectiousness, we modeled the relationship between R(t) and various case variables. To examine associations between case characteristics and R(t), we used linear-mixed regression models. Model covariates were determined a priori using a directional acyclic graph (eFigure 9; https://links.lww.com/EDE/B933). Because the outcome variable, R(t), was by symptom onset day, the unit of analysis for regression models was also symptom onset day, since we could not distinguish the transmissibility of individuals with the same onset day. To incorporate the uncertainty of R(t) estimates into regression results, we used R(t) estimates from all 1,000 constructed epidemic trees and combined regression results using Rubin’s Rules.19,20 We fitted four separate models based on the following form:
R(t,j)=(β1+b1j)(yt−nt)+(β2+b2j)nt
where R(t,j) was the time-varying reproduction number for cases with symptom onset on day t in the jth facility, yt was the number of cases with symptom onset on day t, nt was the number of cases with symptom onset on day t who were residents, and yt- nt, was the number of cases with symptom onset on day t who were staff. In the subsequent three models, nt represented vaccinated, not hospitalized, and survived from COVID-19. The intercept was constrained to equal zero so that R(t) equaled zero for days with no cases. Random slopes were included to account for correlation in R(t) within facilities and to allow associations between R(t) and case characteristics to vary by facility. For LTCF role, the model can be interpreted as follows: the expected value of R(t) increased by β1 for every staff case and by β2 for every resident case. Because we constrained the intercept to equal zero, we can interpret β1 and β2 as the average individual reproduction number, Ri (i.e., the number of secondary cases, irrespective of case characteristics, infected by a single case) for staff and resident cases, respectively.
We determined a priori that vaccination status may confound the association between LTCF role and R(t). Because the unit of analysis for regression models was symptom onset day, we could not directly adjust for individual vaccination status. Therefore, we considered only unvaccinated cases by restricting the data in the model to symptom onset dates before vaccine distribution. Similarly, when examining the association between vaccination status and R(t), we considered only resident cases by restricting the data to days on which only residents (and not staff) had symptom onset. To examine temporal changes in the association between LTCF role and R(t), we restricted the data to days during the first and second pandemic waves. Last, when examining associations between measures of disease severity (hospitalization and death) and R(t), we considered only resident cases, unvaccinated cases, and changes in time by restricting the data to days before vaccine distribution and days on which only residents had symptom onset (overall and during the first and second pandemic waves).
Finally, because there are important differences between skilled nursing and assisted-living facilities, with skilled nursing facilities providing a higher level of care,21 we also conducted a sensitivity analysis in which we restricted the dataset to cases from skilled nursing facilities (n = 1,863; 65% of cases).
We performed all statistical analyses using R v.4.1.1. We calculated R(t) using the EpiEstim package v.2.2-4. This activity was determined by the GDPH Institutional Review Board to be nonresearch and consistent with public health surveillance as per title 45 code of Federal Regulations 46.102(l)(2).
RESULTS Case and Outbreak CharacteristicsWe included a total of 2,849 LTCF COVID-19 cases in the analysis, of whom 2,093 (73%) were residents and 756 (27%) were staff (Table 1). Of the 299 cases with symptom onset after December 31, 2020, 18 (6%) were vaccinated, of whom 10 were residents (5% of resident cases) and eight were staff (8% of staff cases).
TABLE 1. - Characteristics of Fulton County, Georgia, LTCF COVID-19 Casesa Reported March 11, 2020, to September 12, 2021, by LTCF Role (Resident or Staff) Characteristic Resident Cases (n = 2,093) Staff Cases (n = 756) All Cases (n = 2,849) Age, years [median (IQR)] 77 (67, 86) 47 (36, 56) 70 (55, 83) Race/ethnicity [N (%)]b,c Black 1,187 (59) 579 (80) 1,766 (65) White 737 (37) 91 (13) 828 (30) Other 79 (4) 50 (7) 129 (5) Female [N (%)]b 1,228 (59) 648 (86) 1,876 (66) Hospitalized [N (%)]b 623 (40) 39 (6) 662 (30) COVID-19 death [N (%)]b 489 (24) 5 (1) 494 (18)aConfirmed and probable cases were included in the analysis.
bPercentages were calculated by excluding cases with missing information.
cRace/ethnicity was categorized as non-Hispanic Black, non-Hispanic White, or Other; Other race/ethnicity included Hispanic (any race), Asian, and individuals who reported their race as “other.”
LTCF indicates long-term care facility.
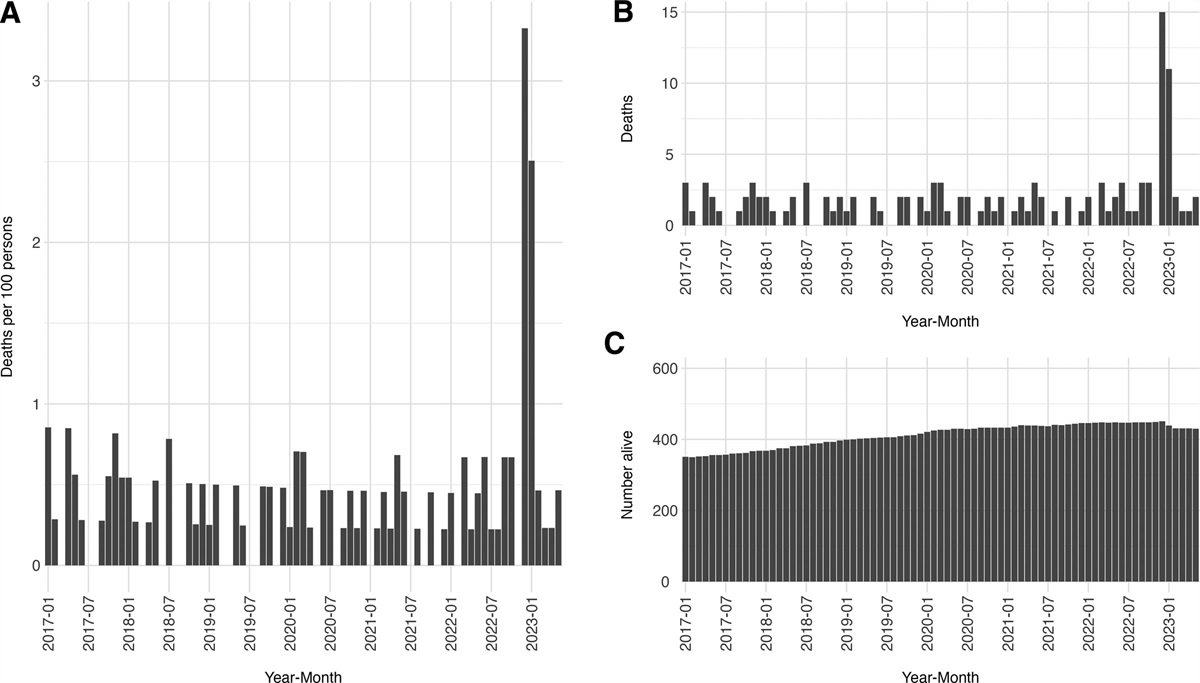
The first LTCF wave was the largest with 2,010 cases, followed by the second wave with 763 cases, and the third with 76 cases (Figure 1A; Table 2). Despite increases in community cases in the third wave (as a result of the Delta variant),22 incidence in LTCFs declined rapidly and remained low after December 2020, with averages of 8.4 cases reported per day in 2020 and 1.5 cases reported per day in 2021. Over the study period, the percentage of cases, hospitalizations, and deaths in Fulton County that occurred in LTCFs declined (eFigure 10; https://links.lww.com/EDE/B933). Overall, 1.7% of cases (n = 2,849), 7.2% of hospitalizations (n = 661), and 19.3% of deaths (n = 492) in Fulton County occurred in LTCFs.
TABLE 2. - Characteristics of Fulton County, Georgia, Long-term Care Facility COVID-19 Cases and Outbreaksa Reported March 11, 2020, to September 12, 2021, by Waveb,c Measure Wave 1 Wave 2 Wave 3 Total Study Period Facilities reporting cases [N] 56 49 20 60 Total cases [N] 2,010 763 76 2,849 Singleton cases [N] 54 49 28 131 Total outbreaks [N] 74 61 13 148 Eventsd per facility [med (IQR)] 2 (1, 3) 2 (1, 3) 2 (1, 3) 4.5 (3, 6.3) [mean (min, max)] 2.3 (1, 5) 2.2 (1, 6) 2 (1, 5) 4.7 (1, 11) Eventd sizee [med (IQR)] 2.5 (1, 15) 2 (1, 5) 1 (1, 2) 2 (1, 7) [mean (min, max)] 15.7 (1, 190) 7 (1, 76) 1.8 (1, 9) 10.2 (1, 190) Eventd lengthf [med (IQR)] 65 (34, 75) 36 (19, 49) 1 (1, 12) 51 (23, 75) [mean (min, max)] 56.9 (1, 122) 38.0 (1, 93) 9.6 (1, 42) 50.6 (1, 122)aCOVID-19 outbreaks were defined as 2 or more cases reported in the same facility. If no new cases were reported in more than 14 days, the outbreak was considered over and any cases reported after 14 days were considered part of a separate outbreak.
bWave 1 included cases reported before September 27, 2020; wave 2 included cases reported September 27, 2020 to March 21, 2021; wave 3 included cases reported March 22, 2021 to September 12, 2021.
cTwo outbreaks involved cases with report dates in both waves 2 and 3. These outbreaks were categorized into waves based on the first outbreak report date.
dEvent includes both singleton cases and outbreaks with two or more cases.
eEvent size is the number of cases in an event.
fEvent length is the time, in days, between the first and last case report dates for an event.
IQR indicates interquartile range; med, median; min, minimum; max, maximum
 Figure 1.:
Figure 1.: Epidemic curves for Fulton County, Georgia, communitya and LTCF COVID-19 casesb with pandemic wavesc shown by shaded regions (A) and trends in the COVID-19 time-varying reproduction number, R(t), in Fulton County, Georgia, LTCFs (B) with dates examinedd shown by dashed vertical lines. aCases that were not residents or staff in LTCFs were considered community cases. bConfirmed and probable cases were included in the analysis. cWaves were determined by weekly Fulton County LTCF case counts based on report dates. The first wave included cases reported before September 27, 2020, the second wave included cases reported September 27, 2020, to March 21, 2021, and the third wave included cases reported March 22, 2021, to September 12, 2021. Note that symptom onset dates occurred earlier than report dates. dDates examined included: May 31, 2020 (shortly after states began lifting pandemic restrictions in the community and the CMS released reopening guidelines for US nursing homes), August 31, 2020 (shortly after CMS began requiring routine COVID-19 testing of nursing home staff), and December 31, 2020 (shortly after the first COVID-19 vaccines were administered to LTCF residents and staff). eR(t) for symptom onset days (rather than individuals) are shown. A dashed horizontal line at R(t) = 1 signifies the extinction threshold below which each case, on average, infects less than one other case. A LOESS trendline with 95% confidence intervals is shown in blue. fEvent day refers to the day of an individual event, defined as a singleton cases or outbreaks of COVID-19, on which cases had symptom onset, excluding days on which no cases had symptom onset. For example, if an event consisted of cases with symptom onsets on May 1, May 5, and May 7, 2020, the corresponding event days would be 1, 2, and 3, respectively. gCase counts (for all event days) by symptom onset week are shown by gray bars. hRefers to the number of prior events in a facility. For example, a daily R(t) estimate shown in pink (for 0 previous events) is an R(t) estimate from the first event that occurred. CMS indicates Centers for Medicare and Medicaid Services; LTCF, long-term care facility; LOESS, locally estimated scatterplot smoothing.
A total of 279 COVID-19 events (including singleton cases and outbreaks) from 60 facilities were reported over the study period (Table 2). Although the average number of events reported per facility remained about the same, the average event size decreased from 15.7 cases in the first wave to 7.0 and 1.8 cases in the second and third waves, respectively. The average event length decreased from 56.9 days in the first wave to 38.0 and 9.6 days in the second and third waves, respectively. Furthermore, the proportion of singleton cases increased from 42% in the first wave to 45% and 68% in the second and third waves, respectively (eFigure 11; https://links.lww.com/EDE/B933).
Time-Varying Reproduction Number, R(t)To examine transmission patterns unaffected by depletion of susceptibles from the current event, we estimated R(t) in the initial days of each. R(t) estimates for event days 1–5 declined from March to September 2020, increased slightly from the end of September to the end of November 2020, and then declined from December 2020 to September 2021 (Figure 1B). After January 2021, R(t) remained below 1, approaching 0 by June 2021.
Associations Between Case Characteristics and R(t)Next, using regression models, we examined heterogeneity in infectiousness as a function of case characteristics. Because of the large proportion of singleton cases included in analyses (47% of events), and because all outbreaks eventually ended, average Ri estimates were all less than 1. Over the full study period, staff cases were estimated to be more infectious than resident cases (average Ri = 0.6 [95% confidence intervals (CI) = 0.4, 0.7] and 0.1 [95% CI = 0.1, 0.2], respectively); these associations were unchanged after accounting for vaccination (Table 3). Results were similar in a sensitivity analysis in which we assumed all cases missing “Staff” from free-text fields were residents (eTable 3; https://links.lww.com/EDE/B933). When stratified by pandemic wave, the association between LTCF role and R(t) was slightly attenuated for wave 2 (average Ri = 0.6 [95% CI = 0.5, 0.7] and 0.4 [95% CI = 0.3, 0.5] for staff and resident cases, respectively), but staff cases were still estimated to be more infectious than resident cases. Among residents in the first pandemic wave, hospitalized cases were estimated to be more infectious than nonhospitalized cases (average Ri = 0.6 [95% CI = 0.4, 0.9] and 0.1 [95% CI = 0.0, 0.3], respectively) and cases who died from COVID-19 were estimated to be more infectious than cases who survived (average Ri = 0.8 [95% CI = 0.5, 1.2] and 0.2 [95% CI = 0.0, 0.4], respectively). However, during the second pandemic wave, hospitalized and nonhospitalized resident cases were equally infectious, as were resident cases who died and survived from COVID-19. Vaccinated resident cases were less infectious than unvaccinated resident cases (average Ri = 0.1 [95% CI = 0.0, 0.7] and 0.5 [95% CI = 0.4, 0.6], respectively); however, estimates and confidence intervals were imprecise as a result of relatively few vaccinated cases.
TABLE 3. - Associationsa Between the COVID-19 Time-varying Reproduction Number, R(t), and Case Characteristics in Fulton County, Georgia, Long-term Care Facilities for Cases Reported March 11, 2020, to September 12, 2021 Days Includedb AllRi (95% CI) Residents OnlyRi (95% CI) PrevaccinationRi (95% CI) Wave 1cRi (95% CI) Wave 2cRi (95% CI) Vaccinatedd Yes 0.2 (0.0, 0.8) 0.1 (0.0, 0.7) – – – No 0.4 (0.3, 0.5) 0.5 (0.4, 0.6) – – – LTCF role Staff 0.6 (0.4, 0.7) – 0.6 (0.5, 0.7) 0.6 (0.5, 0.8) 0.6 (0.5, 0.7) Resident 0.1 (0.1, 0.2) – 0.1 (0.0, 0.1) 0.1 (0.0, 0.1) 0.4 (0.3, 0.5) Hospitalizede Yes 0.4 (0.2, 0.5) 0.6 (0.4, 0.8) 0.4 (0.2, 0.5) 0.6 (0.4, 0.9) 0.6 (0.4, 0.8) No 0.4 (0.3, 0.5) 0.4 (0.3, 0.6) 0.4 (0.3, 0.5) 0.1 (0.0, 0.3) 0.6 (0.4, 0.8) COVID-19 deathe Yes 0.3 (0.2, 0.5) 0.8 (0.6, 1.1) 0.4 (0.2, 0.6) 0.8 (0.5, 1.2) 0.6 (0.4, 0.9) No 0.3 (0.2, 0.4) 0.4 (0.3, 0.5) 0.3 (0.2, 0.4) 0.2 (0.0, 0.4) 0.6 (0.4, 0.7)aAssociations between case characteristics and R(t) were examined using linear-mixed regression models. Regression coefficients can be interpreted as the average individual reproduction number, Ri (i.e., the number of secondary cases infected by a single case) for cases with different characteristics.
bThe analysis was stratified by the following symptom onset days: (1) all days during the study period, (2) days on which only resident cases had symptom onset, (3) days before vaccine administration (January 1, 2021), (4) days in the first pandemic wave (before September 27, 2020), and (5) days in the second pandemic wave (September 27, 2020, to March 21, 2021).
cFor variables Hospitalized and COVID-19 death, included days in the first and second pandemic waves on which only resident cases had symptom onset.
dAssociations between vaccination and R(t) were restricted to symptom onset dates after December 31, 2020, the approximate date when COVID-19 vaccines were first administered to US nursing home residents and staff.
eAssociations between hospitalizations and deaths and R(t) were restricted to symptom onset dates before August 1, 2021 (6 weeks before data download) to account for lags in hospitalization and death.
CI indicates confidence interval; LTCF, long-term care facility; Ri, individual reproduction number.
In sensitivity analyses using serial interval estimates from the literature to estimate R(t), results were robust (eTable 4; https://links.lww.com/EDE/B933). Finally, when the data were restricted to cases from skilled nursing facilities, results were also robust.
DISCUSSIONWe examined SARS-CoV-2 transmission dynamics in Fulton County LTCFs, leading to several important findings. First, case counts, event (singleton cases and outbreaks) size and duration, and SARS-CoV-2 transmissibility in LTCFs rapidly declined and remained low after December 2020, when COVID-19 vaccines were first distributed to US facilities. This decline occurred despite increases in community incidence in summer 2021, suggesting that vaccines were effective in reducing transmission in LTCFs. Second, staff cases were about six times more infectious than resident cases. Third, resident cases with severe outcomes (hospitalization and COVID-19 death) were more infectious than resident cases without severe outcomes, but only during the first pandemic wave (before October 2020). Finally, breakthrough vaccinated resident cases appeared to be slightly less infectious than unvaccinated resident cases; however, results were inconclusive due to small sample sizes.
Other studies have similarly found that the burden of COVID-19 in US LTCFs declined over time23 and that vaccines accelerated declines.24 Decreases in SARS-CoV-2 transmission in Fulton County facilities can likely be attributed to improved infection prevention and control measures, such as improved access to personal protective equipment (PPE), increased testing, and COVID-19 vaccines. Indeed, although there were extreme shortages of PPE in LTCFs as late as August 2020,25 these shortages improved after summer 2020.26 Testing capacity in LTCFs also improved,26 and a previous study found that routine testing of asymptomatic staff in Fulton County facilities led to reduced SARS-CoV-2 transmission.27 Last, nearly 80% of US nursing home residents were vaccinated by February 2021,26 which likely contributed to the rapid declines in SARS-CoV-2 transmission after December 2020.
Although LTCF transmission trends may also be explained by trends in community transmission, case counts in such facilities remained low after December 2020, despite the surge in community cases in summer 2021. Therefore, factors other than community transmission likely contributed to declines in facility transmission. Moreover, although event size and duration decreased over time, the number of events reported per facility remained the same and the proportion of events that were singleton cases increased. This suggests that the number of introductions from the community remained about the same, and that declines in transmission were likely due to improved infection prevention and control measures. Finally, transmission trends in LTCFs may also be attributed to decreases in population susceptibility from natural infection. However, staff turnover rates in nursing homes are high,28 and although staff could also have acquired immunity from community infections, infection rates in the community were much lower than those in LTCFs.29 Furthermore, new residents were still being admitted even early in the pandemic,30 so it is unlikely that a decrease in susceptibility from natural infection alone explains trends in transmission.
Our study is the first, to our knowledge, to quantify the difference in infectiousness between LTCF residents and staff. We found that staff were substantially more infectious than residents, which is likely because staff typically care for multiple residents and also interact with other staff, whereas residents were largely confined to their rooms.3 This has important implications for infection prevention and control practices in LTCFs, as it provides evidence that staff are the primary drivers of SARS-CoV-2 transmission. Therefore, interventions targeted at staff, such as ensuring access to PPE and training, routine testing of asymptomatic staff, and vaccination campaigns targeted at staff, could greatly reduce transmission in LTCFs. Because vaccination acceptance among LTCF staff remains low, with more than a quarter of US nursing home staff still not fully vaccinated as of October 31, 2021,31 improving vaccination rates among staff should be a priority.
Our finding that resident cases with more severe disease were more infectious than those with less severe disease may be explained by higher viral loads or more prolonged and intensive care requirements (before hospitalization or death) for more severe cases.32 Although these cases may also have been more easily identified and placed on transmission-based precautions, PPE shortages early in the pandemic,25 along with overwhelming numbers of COVID-19 cases, may have made these precautions difficult to follow. During the second pandemic wave, resident cases with more severe disease were as infectious as those with less severe disease, suggesting that infection prevention and control practices may
留言 (0)