
記住我
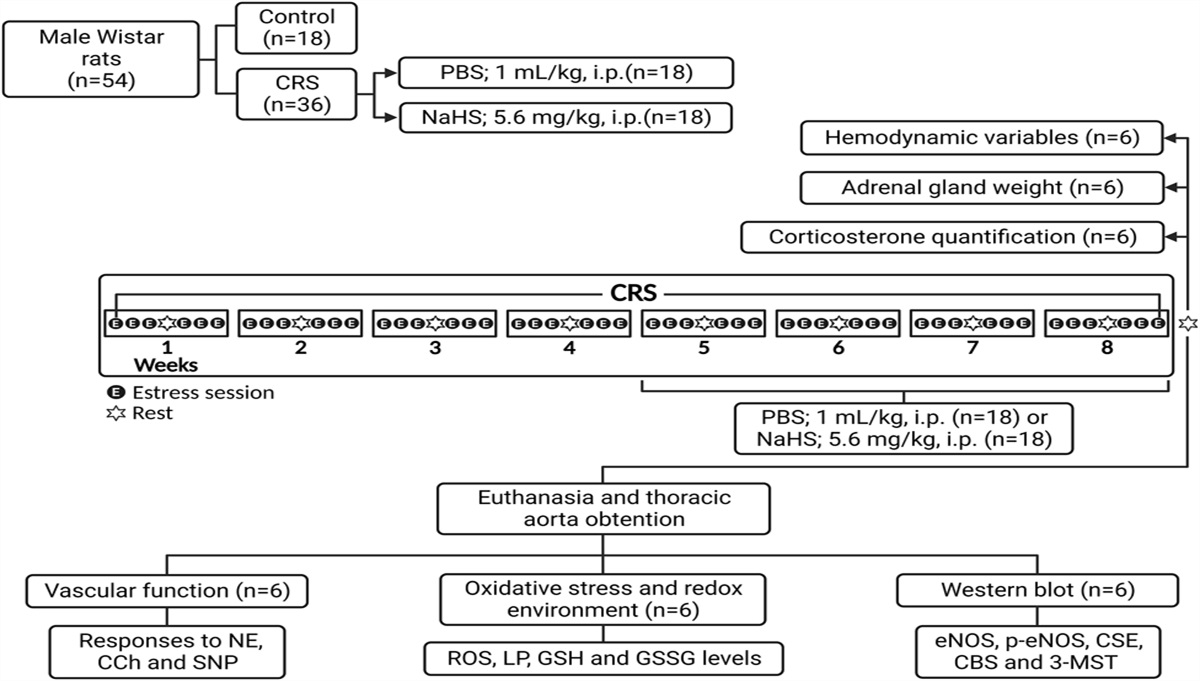
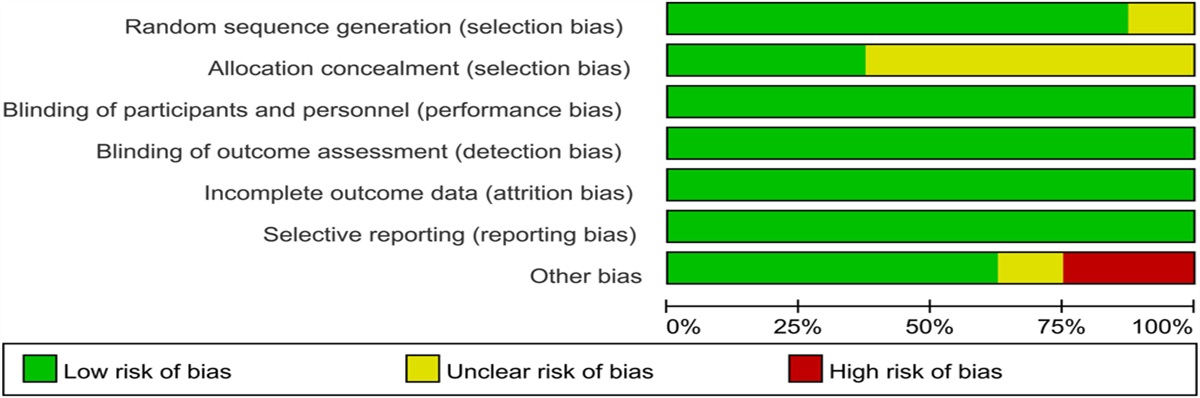
 FIGURE 1.:
FIGURE 1.: Main findings of comprehensive network meta-analysis on the evidence base informing optimal dual antiplatelet therapy (DAPT) duration after percutaneous coronary intervention with drug-eluting stent implantation in East Asians. NACCE, net adverse cerebro-cardiovascular events; RCT, randomized controlled trial.
In short, you cannot let the deadline define the mission. The mission has to define the duration.
Richard Holbrooke
In the setting of atherosclerotic coronary artery disease requiring myocardial revascularization, the goal of dual antiplatelet therapy (DAPT) is to prevent local thrombotic complications related to stent implantation and to blunt prothrombotic systemic burden, to reduce ischemic events.1 In the broad spectrum of coronary artery disease manifestations, the optimal duration DAPT after percutaneous coronary intervention (PCI) represents a challenging situation. It essentially includes the selection of a more appropriate and effective P2Y12 inhibitor as addressed by patient clinical presentation and individual risk profile. As a part of the problem, the minimally required DAPT duration after new-generation DES implantation, designed to overcome most of the limitations of first-generation DES need to be faced with overall ischemic and hemorrhagic complications.2–4 A key premise is also that risk of ischemic events seem relevant in the first month and then decrease.5
Therefore, the balance between ischemia and bleeding requires not only an understanding of the thrombotic risk of the individual patient, mainly related to patient clinical characteristic and comorbidities, but also a clear assessment of the hemorrhagic risk linked to the chosen antiplatelet regimen.
RISK STRATIFICATION TOOLS FOR ISCHEMIA AND BLEEDING RISKSIt is widely recognized that in the same patient, increased ischemic and hemorrhagic risk profile may coexist, thus making difficult decisions on purinergic inhibitor selection and DAPT length. Despite that, the DAPT score6 and the PRECISE-DAPT score7 have gained a major role over other available risk scores to guide and inform decision-making on DAPT duration (Class of Recommendation IIb, Level of Evidence A). Relying on the DAPT score, prolonging P2Y912 inhibitor use beyond 12 months is expected to decrease ischemic events (without a substantial increase in bleeding) or to increase bleeding (without a substantial reduction in ischemic events) in patients with >2 or <2 points, respectively. Indeed, the case can be made to exploit the PRECISE-DAPT score to improve decision-making on top of the DAPT score to better risk-stratify patients for the risk of out of hospital bleedings.3,8
PATIENTS UNDERGOING PCI FOR STABLE CORONARY ARTERY DISEASEIn patients with chronic coronary syndrome, the 2016 American College of Cardiology/American Heart Association guideline update recommended DAPT (aspirin and a P2Y12 inhibitor) for 6 months after PCI with DES, potentially extended for a longer duration in those who remain free of a bleeding complication during this period and do not carry high bleeding risk. Conversely, patients at high bleeding risk may discontinue DAPT at 3 months.3
Likewise, the European Society of Cardiology (ESC) guidelines for the diagnosis and management of chronic coronary syndromes recommend 6-month DAPT in patients who underwent PCI with stenting for stable angina, with prolongation of DAPT after ACS in patients with low bleeding risk, but high thrombotic risk. However, a shorter duration of DAPT may be considered in those at high risk of life-threatening bleeding in view of the very low risk of stent thrombosis after 1–3 months.
In addition, a recent network meta-analysis including almost 80,000 patients, followed for a period of 18 months, suggested that, in comparison with 12-month DAPT, short-term DAPT (<6-months) followed by P2Y12 inhibitor monotherapy may reduce major bleeding after PCI with DES, whereas extended-term DAPT (>12 months) may reduce the risk of myocardial infarction, yet at the expense of more bleeding events.9
PATIENTS UNDERGOING PCI FOR ACSThe risk of recurrent cardiovascular ischemic events or death is highest in the first year after an ACS event and remains elevated long-term.10,11 Based on the heightened and persistent platelet activity that characterizes pathophysiology of ACS, antiplatelet therapy remains crucial to improve acute PCI results and to prevent stent thrombosis afterward while also mitigating the risk of atherothrombosis in other coronary segments. Accordingly, international guidelines routinely recommend low-dose aspirin therapy at long-term in all individuals with ST-elevation myocardial infarction (STEMI) or non–ST-elevation acute coronary syndromes (NSTEACS) without absolute contraindications, together with a P2Y12 inhibitor in STEMI or NSTEACS treated with PCI for at least 12 months unless hemorrhagic risk is considered too high.3,4,12 In 2016, the American College of Cardiology/American Heart Association guideline focused update, exploiting a comprehensive systematic review of randomized trials comparing different durations of DAPT, offered novel insights and input on DAPT for STEMI and NSTEACS.3
Specifically, it pointed out that it is appropriate to prolong DAPT beyond 1 year in subjects with STEMI or NSTEACS, when it is clear that DAPT has been well tolerated, no bleeding event has occurred, and bleeding risk remains reasonably low. Conversely, it is reasonable to discontinue the P2Y12 inhibitor after 6 months in patients who have undergone PCI with DES implantation after NSTE-ACS and who have a high risk of bleeding (eg, receiving concomitant treatment with OAC therapy), are at high risk of a severe bleeding complication (eg, major intracranial surgery), or develop significant overt bleeding. Likewise, the 2017 and 2020 European guidelines recommend continuing DAPT for >12 months in patients who tolerate DAPT without a bleeding complication.7,11 However, the potential for increased bleeding with prolonged DAPT is important to consider. The need for a carefully balanced decision is reinforced by high-quality evidence suggesting that long-term DAPT may provide meaningful protection from atherothrombosis in carefully selected individuals.
Briefly, the DAPT study showed that prolonged DAPT after DES implantation was associated with beneficial effects in prevention from stent thrombosis, and other major atherothrombotic events, despite an increase in the risk of bleeding.5 The PEGASUS-TIMI 54 trial, comparing ticagrelor therapy at different intensity regimens and placebo, suggested that nonfatal atherothrombotic events can be reduced by long-term ticagrelor, especially at lower (60 twice daily) dose.13
DAPT IN ASIAN PATIENTSThe effect of ethnicity on the most appropriate DAPT duration is an important research topic, with profound clinical implications, given the different thrombotic and bleeding risk of Asian patients in general, and even when comparing East Asians versus non-East Asians (Figure 1).14 This may be partly because of a lower risk atherothrombotic events and a higher tendency for bleeding in East Asian individuals over Caucasian individuals, and other non-East Asian populations, which in turn may depend on several genetic (CYP2C19 gene loss-of-function alleles), epigenetic, and behavioral differences (eg, diet, prevalence of smoking, and sedentary lifestyle). Intriguingly, it has been shown that East Asians, despite more frequent resistance to clopidogrel, may experience fewer ischemic events and more bleeding events with prolonged and intense DAPT, leading to a veritable “East Asian paradox.”15–17 Even in the CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance) trial, Asian patients had a lower risk of atherothrombotic events and a higher rate of bleedings during DAPT in comparison to other ethnic groups.18
It is clear that risk-stratification and prognostication based on scores is an active field of research, with DAPT and PRECISE-DAPT scores being established information sources on the most appropriate DAPT duration.5,6 However, these scores mainly focus on Western patients. To address this limitation, Kang and colleagues have generated the ADAPT score, suitable to guide optimal combinations, doses and durations of antithrombotic regimens.7 In this issue of the Journal of Cardiovascular Pharmacology Zhong et al19 highlight the pros and cons of prolonged DAPT duration in East Asians, poignantly showing through refined network meta-analytic tools that abbreviated DAPT regimens may indeed maintain adequate antithrombotic protection while minimizing bleeding risk, strong of a total sample of more than 30,000 patients. Indeed, this work reinforces the concept that a gentler approach at DAPT intensity and duration is warranted in East Asians, to maximize protection from both ischemic and bleeding events. Accordingly, Western recommendations for potent P2Y12 inhibition and DAPT duration after PCI should not be applied without individualized decision making in East Asian population. This holds true notwithstanding that prolonged DAPT may be considered appropriate in fit patients at low risk of bleeding, high thrombotic risk, and motivation to prevent ischemic events (eg, younger men with high SYNTAX score).
In conclusion, the consensus on antiplatelet therapy for patients with ACS or undergoing PCI in East Asians in 2018 recommends that DAPT can be extended to more than 12 months to prevent recurrent ischemic events in high-risk patients, conversely it should be shortened in patients with high-risk of bleeding or intolerance long-term DAPT in East Asians.
REFERENCES 1. Capodanno D, Alfonso F, Levine GN, et al. ACC/AHA versus ESC guidelines on dual antiplatelet therapy: JACC guideline comparison. J Am Coll Cardiol. 2018;72:2915–2931. 2. Giacoppo D, Matsuda Y, Fovino LN, et al. Short dual antiplatelet therapy followed by P2Y12 inhibitor monotherapy vs. prolonged dual antiplatelet therapy after percutaneous coronary intervention with second-generation drug-eluting stents: a systematic review and meta-analysis of randomized clinical trials. Eur Heart J. 2021;42:308–319. 3. Bittl JA, Baber U, Bradley SM, et al. Duration of dual antiplatelet therapy: a systematic review for the 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68:1116–1139. 4. Amsterdam EA, Wenger NK, Brindis RG, et al. AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014 2014;64:e139–e228. 5. D'Ascenzo F, Biolè C, Raposeiras-Roubin S, et al. Average daily ischemic versus bleeding risk in patients with ACS undergoing PCI: insights from the BleeMACS and RENAMI registries. Am Heart J. 2020;220:108–115. 6. Mauri L, Kereiakes DJ, Yeh RW, et al.; DAPT Study Investigators. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N Engl J Med. 2014;371:2155–2166. 7. Costa F, van Klaveren D, James S, et al.; PRECISE-DAPT Study Investigators. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet. 2017;389:1025–1034. 8. Valgimigli M, Bueno H, Byrne RA, et al.; ESC Scientific Document Group; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39:213–260. 9. Khan SU, Singh M, Valavoor S, et al. Dual antiplatelet therapy after percutaneous coronary intervention and drug-eluting stents: a systematic review and network meta-analysis. Circulation. 2020;142:1425–1436. 10. Pedersen F, Butrymovich V, Kelbæk H, et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. 2014;64:2101–2108. 11. Jernberg T, Hasvold P, Henriksson M, et al. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. Eur Heart J. 2015;36:1163–1170. 12. Collet JP, Thiele H, Barbato E, et al.; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289–1367. 13. Bonaca MP, Bhatt DL, Cohen M, et al.; PEGASUS-TIMI 54 Steering Committee and Investigators. Long-term use of ticagrelor in patients with prior myocardial infarction. N Engl J Med. 2015;372:1791–1800. 14. Ki YJ, Kang J, Park J, et al. Efficacy and safety of long-term and short-term dual antiplatelet therapy: a meta-analysis of comparison between Asians and non-Asians. J Clin Med. 2020;9:652. 15. Kang J, Kim HS. The evolving concept of dual antiplatelet therapy after percutaneous coronary intervention: focus on unique Feature of East Asian and “Asian paradox”. Korean Circ J. 2018;48:537–551. 16. Kang J, Park KW, Ki YJ, et al. Development and validation of an ischemic and bleeding risk evaluation tool in East Asian patients receiving percutaneous coronary intervention. Thromb Haemost. 2019;119:1182–1193. 17. Huo Y, Jeong Y, Gong Y, et al. 2018 update of expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Sci Bull (Beijing). 2019;64:166–179. 18. Bhatt DL, Fox KA, Hacke W, et al.; CHARISMA Investigators. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:1706–1717. 19. Zhong P, Shang Y, Bain N, et al. Dual antiplatelet therapy after drug-eluting stents implantation in East Asians: a network meta-analysis of randomized controlled trials. J Cardiovasc Pharmacol. 2022. in press.
留言 (0)