
記住我






A 48-year-old woman was referred from primary care to our hospital. The patient had a month-long history of chronic abdominal pain, fullness, constipation, and diarrhoea; was diagnosed with irritable bowel syndrome by her family doctor; and was treated with ramosetron hydrochloride. The patient had a history of mild depression, but no other comorbidities. Her abdomen was soft and flat, with no peritoneal signs.
Laboratory data were as follows: white blood cell count, 7250/μL; C-reactive protein level, 0.98 mg/dL; carbohydrate antigen 19-9 level, 2.9 U/mL (normal < 37.0 U/mL); and carcinoembryonic antigen level, 2.1 ng/mL (normal < 5.0 ng/mL). Colonoscopy revealed 30-mm submucosal tumour-like findings in the cecum, which was probably the appendix opening (Fig. 1). No biopsy was performed. Enhanced computed tomography showed a 100-mm irregular swelling in the appendix and thickening of the appendiceal wall with cystic dilatation (Fig. 2).
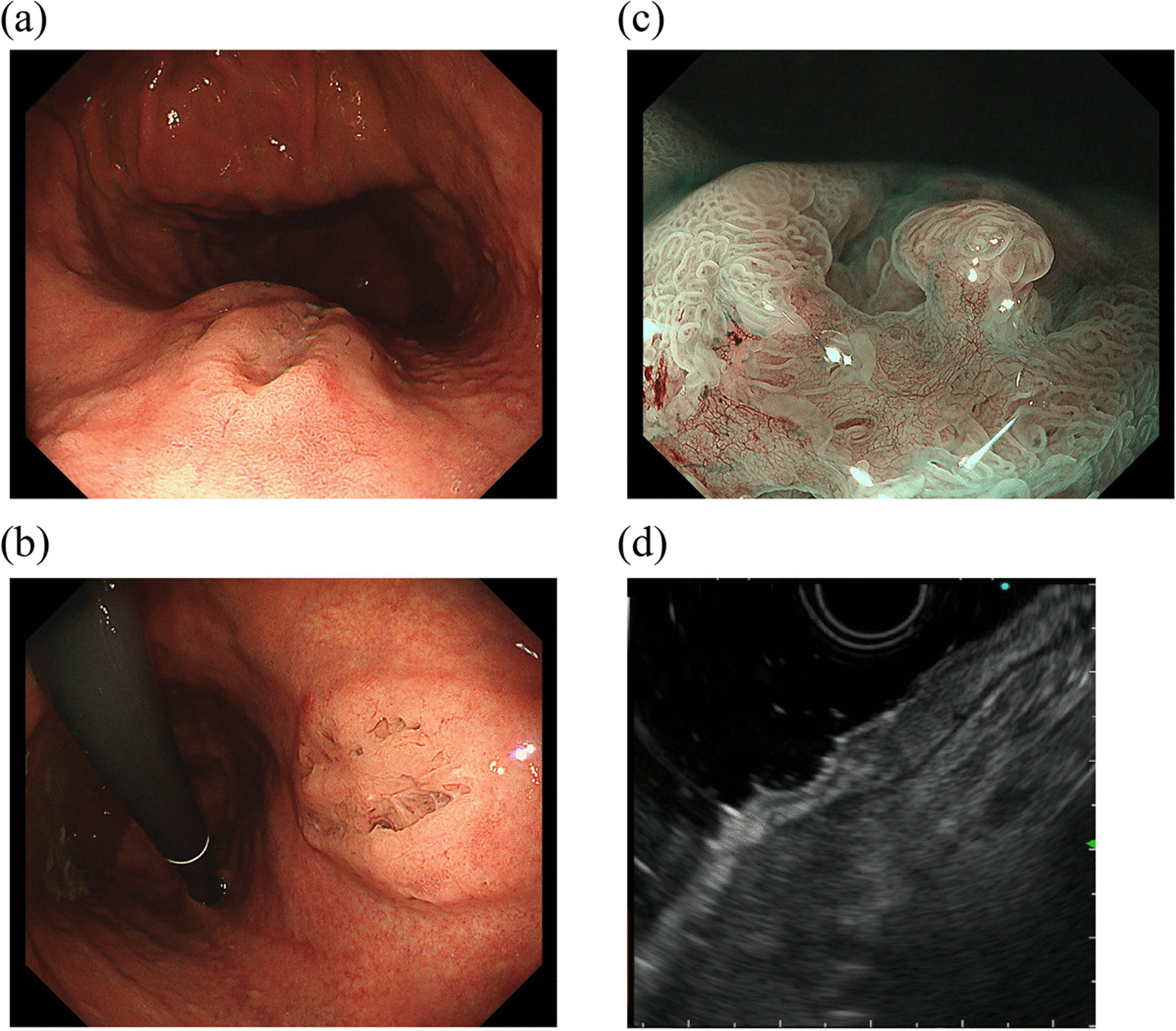
Fig. 1
Endoscopic appearance of the appendix opening in the cecum on colonoscopy. The submucosal tumour was soft, with a positive cushion sign when we used forceps to compress the tumour
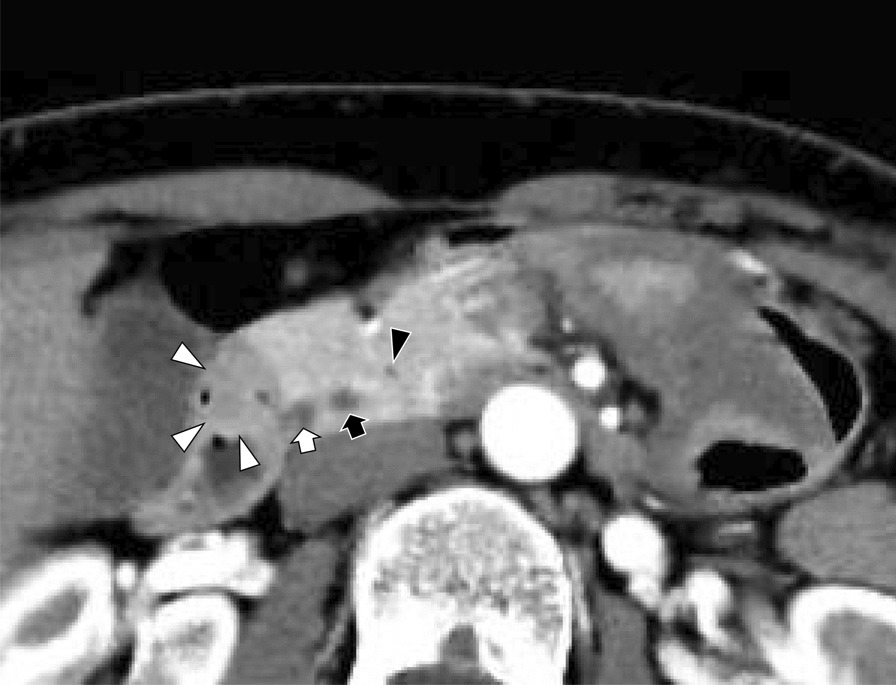
Fig. 2
Axial images of contrast-enhanced computed tomography showing an irregular appendix (white arrows) swelling and thickening of the appendix wall with cystic dilation. Calcified lesions are also found inside the appendix
Laparoscopic ileocecal resection with D3 lymph node dissection was performed with a preoperative diagnosis of appendiceal cancer. Laparoscopic findings included an irregular swelling of the appendix and a partial white discoloration on the appendiceal serosa surface; however, no invasion of surrounding tissues was observed. The appendiceal tumour was expansive, meandering, and thickened. Although a tumour-like mass was noted on the proximal side of the appendix, its boundary was unclear, and no tumour was found to form a clear nodule (Fig. 3). The appendiceal tumour in the resected specimen measured 80 × 60 × 40 mm.
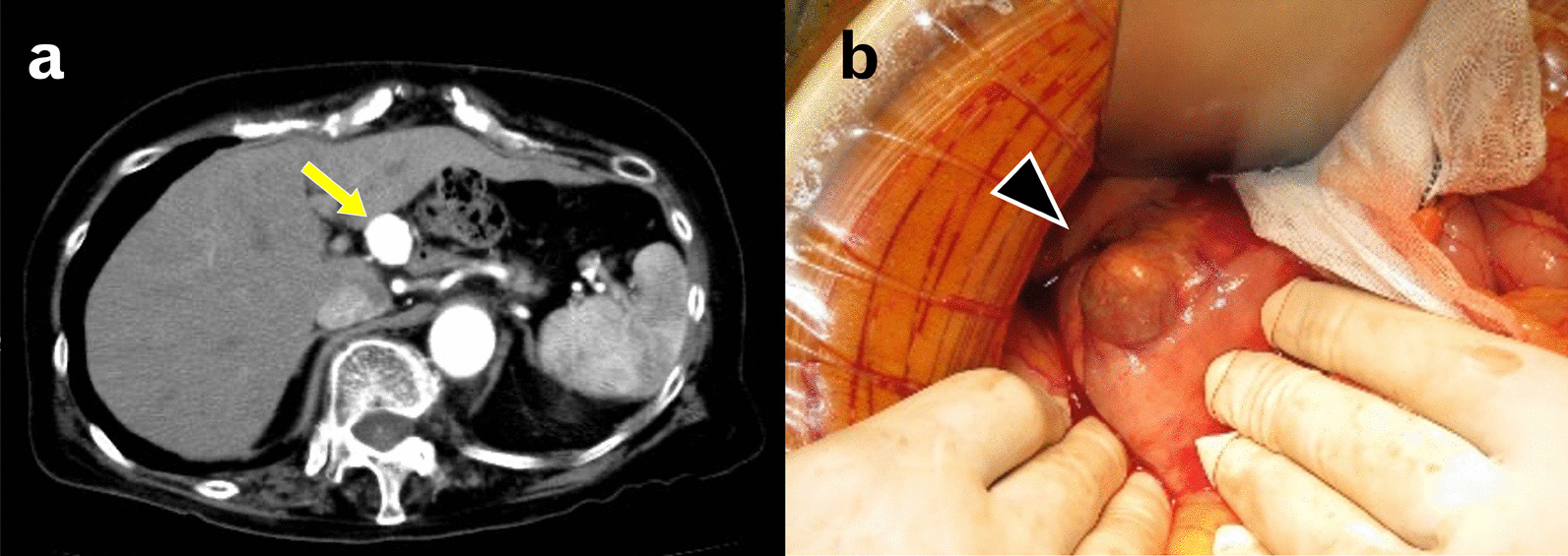
Fig. 3
Intraoperative findings of the appendix. The appendix (black arrows) was dilated, and the border with the cecum (*) was unclear
Histologically, atypical cells mainly composed of signet-ring-like cells were found to proliferate solidly and invasively in the appendiceal mucosa, and they reached the subserosa (Fig. 4A). The tumour cells contained abundant mucus that was stained using alcian blue, and the infiltration was prominent in and around the nerves (Fig. 4B). Immunostaining results were as follows: CD56 (NCAM) (−), S-100 (−), chromogranin A (CGA) (−), synaptophysin (−), insulinoma-associated protein 1 (INSM1) (−), CEA (Mo) (+), CK (AE1/AE3) (+), CK7 (±), and CK20 (+). Tumour differentiation into neuroendocrine cells was unclear (Fig. 4C–F); thus, the tumour was considered a signet-ring cell carcinoma. No tumour invasion was observed in the veins and lymph vessels, and no metastases were noted in the lymph nodes. Additionally, spindle-shaped cells were observed to spread mainly in the mucosa from the appendix to the ascending colon continuously and from the submucosa to the muscularis depending on the region (Fig. 4G). Immunostaining showed that spindle-shaped cells were positive for neural markers, and the results were as follows: CD117 (c-kit) (−), CD34 (−), SMA (−), Desmin (−), S-100 (+), CD56 (NCAM) (+), CGA (±), synaptophysin (+) and Ki-67 (MIB-1) (low), indicating a ganglioneuromatosis (Fig. 4H).
Fig. 4
Histopathological examination. Proliferation of atypical cells, mainly signet-ring-like cells, in the appendix mucosa is observed using haematoxylin–eosin staining (A). Abundant mucus is confirmed using alcian blue staining (B). Immunohistochemical staining for chromogranin A (C) and synaptophysin (D) are negative in the cytoplasm of tumour cells. The immunoactivity for synaptophysin reveals nerve fibre proliferation in the mucosa of appendix. Immunohistochemical staining for insulinoma-associated protein 1, which is nuclear marker of neuroendocrine differentiation, is negative in the tumour cells (E). Immunostaining for CK (AE1/AE3) highlights the cytoplasm of the tumour cells and normal epithelium (F). Proliferation of spindle-shaped cells from the lamina propria to the lower layer in the colon is noted (G), and the neural marker (CD56) is positive (H)
After several days of postoperative treatment, the patient recovered well and did not have any abdominal pain, fullness, and diarrhoea. The patient agreed to four courses of capecitabine plus oxaliplatin (CAPEOX) as postoperative adjuvant chemotherapy for high-risk stage IIA (T3, N0) appendiceal cancer. Twenty-three months after surgery, the patient is alive and in good condition without recurrence.
留言 (0)