
記住我




More than 1.9 million children sustain a concussion in the United States annually, with adolescents accounting for more than 50% of these injuries.1 Sport- and recreation-related concussion is a complex injury that affects multiple neurological domains simultaneously and can negatively impact many aspects of daily adolescent life, including school and sport.2–4 Visual and autonomic deficits frequently occur in adolescents after concussion.5–7 Specifically, nearly 70% of concussed adolescents evaluated in a specialty care setting presented with visual deficits, such as convergence insufficiency, accommodative disorders, and/or saccadic dysfunction.5 Although most children with concussion achieve symptom recovery within 4 weeks, the presence of visual deficits after injury predicts prolonged symptoms and recovery.8,9 As such, accurate detection of visual deficits soon after a concussion may allow for earlier intervention, potentially reducing overall symptom burden or the likelihood of experiencing persistent post-concussion symptoms.
Currently, visual deficits are assessed clinically via vision-specific symptom inventories and clinical examination of saccades, smooth pursuits, accommodation, and convergence.10–14 Although these measures have demonstrated both utility and reliability among pediatric patients with concussion, they are not used ubiquitously among athletic trainers, who are often the first health care providers to conduct concussion assessments.15 Recent advances have enabled objective eye tracking to quantify visual deficits in acutely concussed children, adolescents, and adults.16–18 Previous reports using this eye tracking methodology have described its utility in identifying deficits in eye positioning during a smooth pursuit task, achieving 71.9% sensitivity and 84.4% specificity in identifying concussion among a cohort of pediatric patients with a moderate level of reliability among uninjured adolescent athletes.16,19 The utility of eye tracking for characterizing saccadic movement and pupillary dynamics is of particular interest because deficits in saccadic eye movements and pupillary dynamics have been described by researchers using other methods in the pediatric and adolescent concussion populations.10,20,21 An eye tracking assessment that includes pupillary dynamic metrics may also provide useful information for both visual and autonomic function. Measuring right and left eye position, saccadic movement, and pupillary dynamics simultaneously during an eye tracking task could more comprehensively and objectively characterize deficits that may contribute to acute and persistent symptoms.
The purpose of this study was to determine if there are differences in objective eye tracking metrics that characterize eye position, saccadic movement, and pupillary dynamics between uninjured adolescents, adolescents with acute concussion symptoms (≤28 days since injury), and adolescents with persistent concussion symptoms (>28 days since injury). We hypothesized that those with acute or persistent concussion symptoms would have disconjugacy in left and right eye position, abnormal saccadic movement, and abnormal pupillary dynamics compared with the uninjured adolescent comparison group. We also hypothesized that there would be sex-specific differences between uninjured adolescents and those with acute or persistent concussion symptoms in these objective eye tracking metrics because female adolescents demonstrate greater oculomotor and vestibular dysfunction in comparison with male adolescents after a concussion.22
METHODS Study Design, Setting, and ParticipantsParticipants aged 13 to 17 years were enrolled between August 2017 and June 2021 as part of a prospective observational cohort study assessing a suite of clinical and objective measures, including objective eye tracking, approved by the Children's Hospital of Philadelphia Institutional Review Board.13 Participants and/or their parents/legal guardians provided written assent/informed consent. Uninjured athletes (n = 180) were recruited from a private suburban high school and completed an objective eye tracking assessment before their sports season. Concussed participants (n = 224) were recruited during a clinical care visit from the Children's Hospital of Philadelphia Minds Matter Concussion program, as well as from the high school. Thirty-two participants who enrolled in the uninjured cohort subsequently sustained a concussion and, for the purposes of this analysis, were included only in the concussed cohort. Concussion diagnosis was made by a trained sports medicine pediatrician according to the most recent Consensus Statement on Concussion in Sports.4 Concussed participants performed the objective eye tracking assessment during a clinical visit. If a participant with concussion had multiple eye tracking assessments across several visits, only the first assessment was used in this analysis. Participants with a concussion diagnosis were categorized into two groups for analysis: an acute group, who completed their first eye tracking assessment ≤28 days since injury, and a persistent group, who completed their first eye tracking assessment >28 days since injury. Exclusion criteria for both concussed and uninjured participants included a previous concussion within 1 month of injury or pre-injury assessment, and any ocular or neurologic condition that could affect eye tracking responses.
Of the 346 participants enrolled, valid eye tracking assessments were obtained for 178 of 180 uninjured (98.8%) and 219 of 224 (97.8%) concussed participants. Among those without a valid assessment, five had insufficient data capture during the assessment of one or both eyes. Data from two additional subjects were lost because of device error.
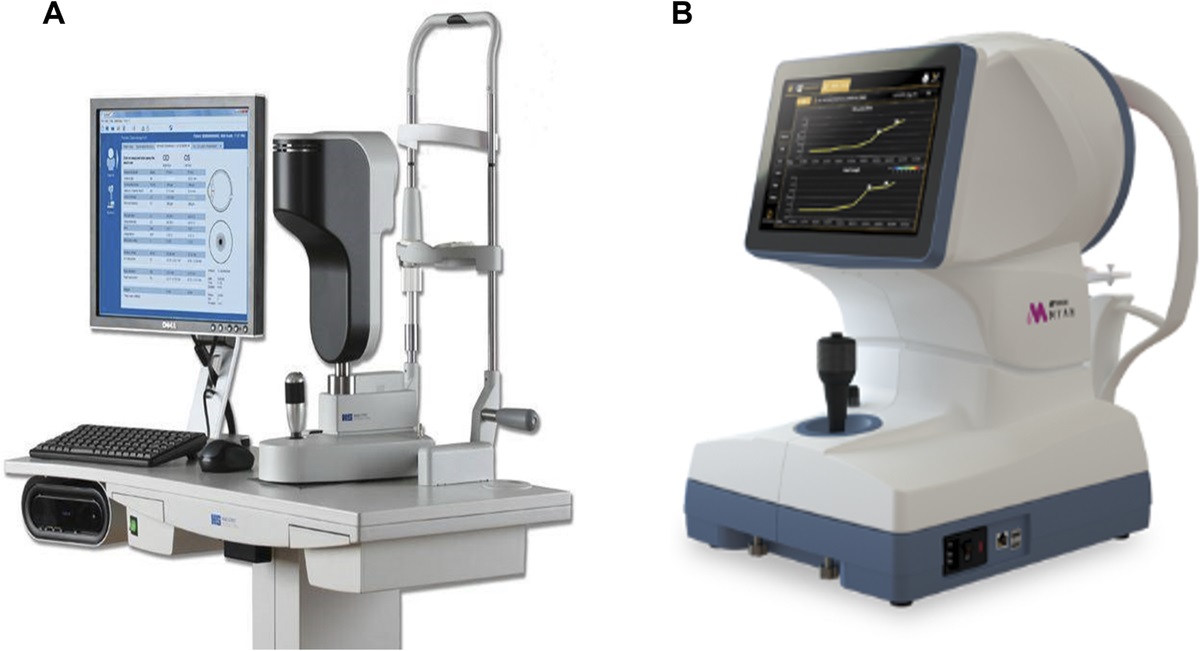
InstrumentationEye movements were recorded using EyeBOX (Oculogica, Inc, New York, NY), which uses an Eyelink 1000 (SR Research, Ottawa, Ontario, Canada), positioned at a fixed distance of 55 cm from the participant's eyes while they track during a 220-second stimulus video (Fig. 1). The stimulus video, a 220-second child's movie music video clip with a 4:3 aspect ratio, occupied approximately one-ninth of the display monitor area and moved in a smooth clockwise direction along the outer edges of the monitor at a rate of 10 seconds per edge of the monitor. The total visible span of the moving aperture was approximately 17° horizontally and 13° vertically from the middle of the screen. Eye position data from both eyes were obtained independently at 500 Hz. Because the position of the head was fixed, it is important to note that the eye position, the position of the eye in the orbit, and the gaze position, the position of the eye and head combined, are equivalent. The EyeBOX is not spatially calibrated, as the metrics of interest are derived from changes in eye position over time, allowing for independent analysis of each pupil position with respect to the moving visual stimulus. The EyeBOX pupil mode was set to center of mass. The first and last 10 seconds of the assessment were discarded to reduce potential noise from capturing the onset and completion of the eye tracking task. The eye tracking data were then automatically processed to yield 256 eye tracking metrics that quantify (a) eye position (the position of the left and right pupils independently and comparisons of their positions over time during the task), (b) saccadic movement in each eye, and (c) pupillary dynamics for each eye, both independently and together. Eye position metrics were derived from the x and y spatial coordinates of each pupil and by comparing the coordinates of one eye to the other eye at any given time point throughout the entire assessment.23 There were a total of 183 metrics of eye position, 60 metrics of saccadic movement metrics, and 13 metrics of pupillary dynamics. The large number of eye position and saccadic movement metrics are due to the fact that these metrics are evaluated based on the side of the screen the video was on (i.e., the top, right, bottom, and left) for both the eyes individually and comparisons between the two. Although the video stimulus moves smoothly along the edges of the screen, saccadic eye movements were captured when the participant glanced between objects, such as two characters, within the video stimulus. Saccadic eye movements were automatically detected based on right and left eye position velocities.
 FIGURE 1:
FIGURE 1: (A) Image of eye tracker with trained research staff and mock participant completing the assessment. (B) Image of screen that participant views during the assessment with the x and y axes labeled. Some eye tracking metrics related to eye position and saccadic movement are measured in either the x and y axis directions.
ProceduresParticipants completed questionnaires to capture demographic and clinical characteristics, such as age at the time of assessment, sex, race/ethnicity, and prior history of concussion. The Post-Concussion Symptom Inventory (PCSI), a self-report of symptom severity over the past 2 days (21 items on a 7-point Likert scale [0, none; 6, most severe], total score range of 0 to 126), was completed on the day of the eye tracking assessment for participants with acute or persistent concussion symptoms and within 7 days of the eye tracking assessment for uninjured participants.24 Trained research staff conducted the objective eye tracking assessment in an athletic training room or sports medicine office and were not blinded to concussion status. Participants sat in a chair and placed their chin on a height-adjustable chin rest to limit movement. To confirm detection of pupils, participants were instructed to focus on the computer monitor, and research staff confirmed that the device detected both left and right pupils around all four edges of the computer screen. Participants then were instructed to focus on a 220-second video clip that traveled in a smooth clockwise rotation along the edges of the monitor while eye movements were recorded as described previously.
Statistical AnalysesDistributions of demographic and clinical characteristics for those with acute or persistent concussion symptoms and uninjured adolescents were compared using χ2 statistics and Fisher exact tests for categorical variables (sex, race/ethnicity, and history of prior concussion) and analysis of covariance with Tukey honestly significant difference post hoc testing for continuous variables (age and PCSI score). All 256 eye tracking metrics were compared among uninjured adolescents and those with acute or persistent concussion symptoms, with Kruskal-Wallis tests and Dunn post hoc tests. In an exploratory analysis of differences in eye movement post-injury by sex, eye tracking metrics were compared between uninjured participants and those with acute or persistent concussion symptoms among female and male subjects separately, with Kruskal-Wallis tests and Dunn post hoc tests. Multiple comparisons were accounted for by calculating Bonferroni corrections where a P < .05/256 or .00019 was considered significant for the Kruskal-Wallis tests and P < .05/768 or .000065 was considered significant for the Dunn post hoc tests. We also calculated area under the curve (AUC) values from receiver operating characteristic (ROC) curves and Cohen d effect sizes for metrics significantly different between groups. Finally, an analytic regression model based on the discriminatory eye tracking metrics using principal components analysis was created. All analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria).25
RESULTS Study PopulationAmong participants with a concussion and evaluable eye tracking assessments, 130 (59.4%) had acute concussion, and 89 (40.6%) had persistent concussion symptoms (Table 1). A total of 75.8% had a sport- or recreation-related concussion. The uninjured cohort differed from the persistent concussion symptom cohort in race and ethnicity. The uninjured cohort was also slightly younger than the persistent concussion symptom cohort. Those with acute concussion symptoms completed an eye tracking assessment within a median interquartile range of 11 (4 to 19.75) days after injury, whereas those persistent with concussion symptoms completed an eye tracking assessment within a median interquartile range of 53 (40–68) days after injury. Participants with acute and persistent concussion symptoms reported significantly greater overall symptom severity than uninjured participants. The persistent concussion symptom group had a significantly higher proportion of females (69.7%) than the acute concussion symptom group (47.7%, P = .004) and the uninjured group (53.4%, P = .02). A significantly greater proportion of the acute and persistent concussion symptom groups reported a prior history of concussion compared with the uninjured group. Demographic and clinical characteristics associated with concussion status were not subsequently included as covariates in comparisons of eye tracking metrics across groups, as these variables did not show an association with the eye tracking metrics.
TABLE 1 - Demographic and clinical characteristics of the study cohort, with continuous data presented as median (IQR) Acute concussion symptoms (n = 130) Persistent concussion symptoms (n = 89) Uninjured (n = 178) P Post hoc test P Age, median (IQR) (y) 15.6 (14.5–16.9) 16.0 (14.7–17.0) 15.1 (14.3–16.3) .01 Acute vs. persistent: .74Bold values are significant. *A total of 122 (93.8%) with acute concussions symptoms, 85 (95.5%) with persistent concussion symptoms, and 148 uninjured completed PCSI. †One with acute concussion symptoms and one with persistent concussion symptoms did not report prior history of concussion. IQR = interquartile range; PCSI = Post-Concussion Symptom Inventory.
Of the 256 metrics, there were significant differences among uninjured participants and those with acute or persistent concussion symptoms after Bonferroni correction for multiple comparisons, in 13 metrics, 11 of which were related to pupillary dynamics. Table 2 includes definitions of these 13 metrics. All pupil size metrics represent the area of the pupil as calculated by the number of pixels the pupil occupies in the camera image. Participants with acute or persistent concussion symptoms had significantly larger left and right mean, median, and minimum and maximum pupil size (acute vs. uninjured, P < .001; persistent vs. uninjured, P < .001). Those with acute or persistent concussion symptoms also had significantly greater pupil asymmetry, with greater mean, median, and variance differences in left and right pupil size (mean: acute vs. uninjured, P < .001; persistent vs. uninjured, P < .001; median: acute vs. uninjured, P < .001; persistent vs. uninjured, P = .003; variance: acute vs. uninjured, P < .001; persistent vs. uninjured, P < .001). Two eye position metrics were significantly different among groups—conj.varYbot, defined as the variance between the left and right eyes in the y direction along the bottom of the screen (acute vs. uninjured, P = .003; persistent vs. uninjured, P < .001; acute vs. persistent, P = .04), and conj.varYtopbotRatio, defined as the total variance between the left and right eyes in the y axis around forced average of zero for the ratio of the segment where the visual stimulus moves across the top of the screen to the segment where the visual stimulus moves across the bottom of the screen (acute vs. uninjured, P < .001; persistent vs. uninjured, P = .001). Median and interquartile range values for each metric for each group are presented in Table 3. Violin plots of uninjured adolescents, acute cases, and persistent cases for the 13 metrics can be found in Appendix Figures A1 to A13, available at https://links.lww.com/OPX/A573. Area under the ROC curve, sensitivity, specificity, and effect sizes for the 13 metrics can be found in Appendix Tables A1 to A3, available at https://links.lww.com/OPX/A572.
TABLE 2 - Definitions of eye tracking metrics significantly different between groups Metric Definition left.pupilsizemean The average pupil size (area) of the left eye left.pupilsizemedian The median pupil size (area) of the left eye right.pupilsizemean The average pupil size (area) of the right eye right.pupilsizemedian The median pupil size (area) of the right eye left.pupilsizemaxabs The maximum pupil size (area) of the left eye right.pupilsizemaxabs The maximum pupil size (area) of the right eye left.pupilsizeminabs The minimum pupil size (area) of the left eye right.pupilsizeminabs The minimum pupil size (area) of the right eye conj.pupilsizediffmean The average difference in pupil size between the left and right eyes, a measure of pupil asymmetry conj.pupilsizediffmedian The median difference in pupil size between the left and right eyes, a measure of pupil asymmetry conj.pupilsizediffvar The variance of the differences in pupil size between the left and right eyes, a measure of pupil asymmetry conj.varYbot The total variance between the left and right eyes in the y direction around forced average of zero when the video moves along the bottom of the screen conj.varYtopbotRatio The total variance between the left and right eyes in the y axis around forced average of zero for the ratio of the segment where the visual stimulus moves across the top of the screen to the segment where the visual stimulus moves across the bottom of the screenAdjusted P values are reported by multiplying the actual P value by the number of comparisons. Bold values are significant. IQR = interquartile range.
To explore changes in eye position, saccadic movement, and pupillary dynamic metric post-injury by sex, eye tracking metrics were compared between uninjured adolescents and those with acute or persistent concussion symptoms among female and male subjects separately. Demographic and clinical characteristics of male and female participants can be found in Appendix Tables A4 and A5, available at https://links.lww.com/OPX/A572. After Bonferroni correction, 12 of 13 metrics found to be significantly different between uninjured participants and those with acute or persistent concussion symptoms in the overall sample were also significantly different among female subjects according to status (uninjured, acute or persistent concussion symptoms) (Table 4). In contrast, only four eye tracking metrics were significantly associated with concussion status (Table 5).
TABLE 4 - Eye tracking metrics median and IQR values in female subjects Acute concussions symptoms (n = 62) Persistent concussion symptoms (n = 62) Uninjured (n = 95) Adjusted P Post hoc test P left.pupilsizemean 2087.13 (1830.50–2449.87) 2247.83 (1673.73–2601.17) 1327.01 (1057.57–1660.14) <.001 Acute vs. persistent: >.99Adjusted P values are reported by multiplying the actual P value by the number of comparisons. Bold values are significant. IQR = interquartile range.
留言 (0)