
記住我

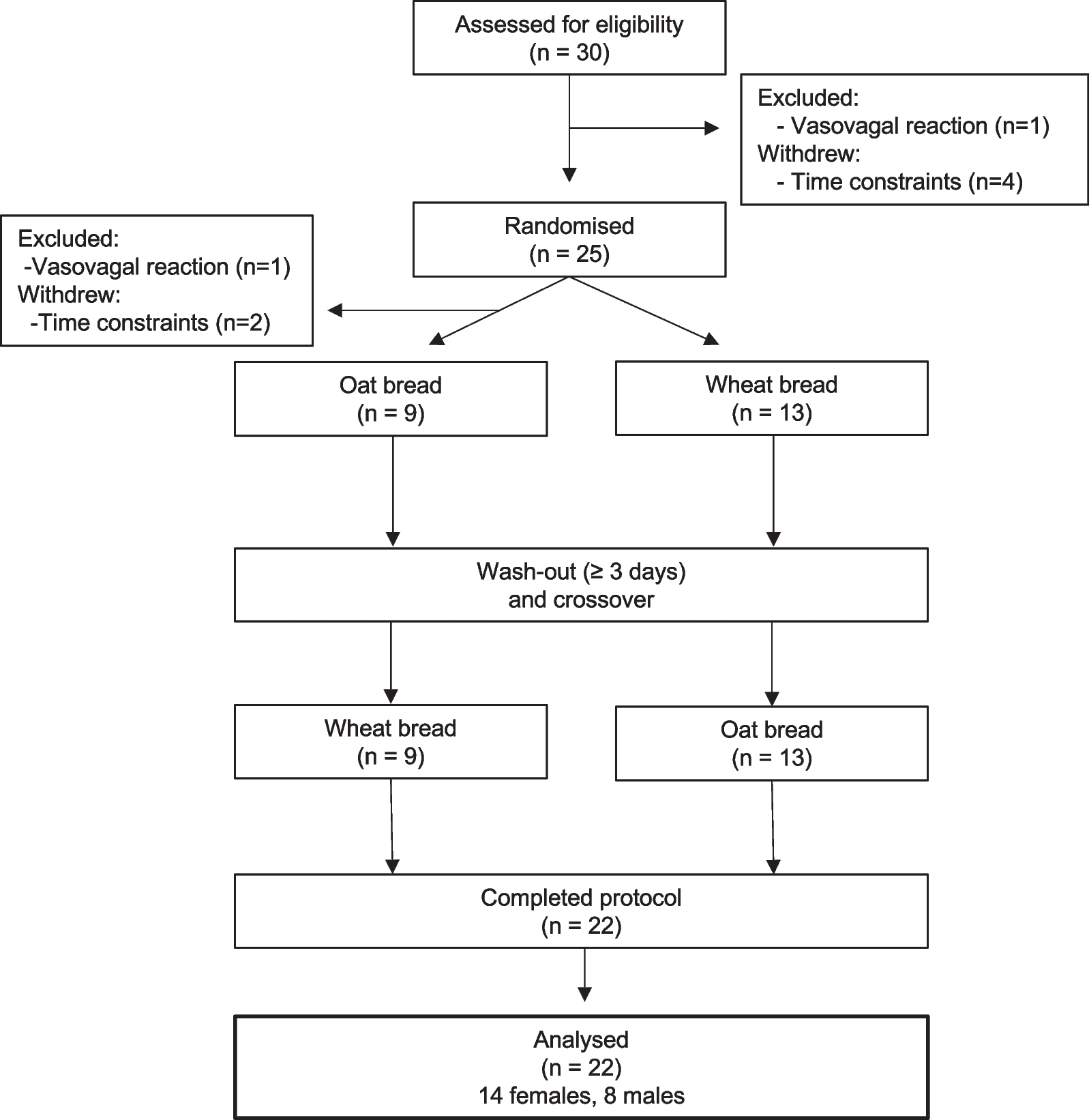

The process of literature screening is shown in Fig. 1. Two authors independently and systematically retrieved 323 articles respectively. Overall, 24 articles with 83 unique outcomes were included by eligibility criteria. A list of all the excluded articles and the reason for exclusion was provided in Additional file 2: Table S2.
Fig. 1
Literature screening process of this study
Table 1 shows the characteristics of these 24 studies. Among all included articles, nine did not conduct methodological quality assessment for original studies [21,22,23,24,25,26,27,28], the remaining 15 articles used the Newcastle Ottawa Quality Assessment scale(NOS) for assessment. The included studies covered 43 significant associations between 83 diet, nutrition related indicators and biliary diseases risk. All systematic reviews and meta-analyses were published between 2008 and 2021. Among these articles, four included only case–control studies [1, 27, 29,30,31], six included only cohort studies [25, 26, 32,33,34,35], and the remaining thirteen included different types of original studies, encompassing case–control studies, cohort studies, nested case–control studies and cross-sectional studies. The number of original studies included in these articles ranged from 2 to 26. Except that only one article could not obtain the exact number of participants and cases [24], the number of participants in other studies were at least 435, at most 10,786,685, and the number of cases were at least 105, at most 61,071.
Table 1 The general characteristics of the 24 systematic reviews and meta-analysesTables 2, 3 and 4 respectively show the relationship between dietary factors, nutrition related indicators, alcohol and biliary diseases. Among the included articles, 4 focused on gallbladder cancer, 8 on cholangiocarcinoma, 9 on cholecystolithiasis/gallbladder diseases, and 3 on both gallbladder cancer and cholangiocarcinoma. Seventeen of twenty-four studies focused on fourteen food items, including alcohol, coffeee, high spicy food, tea, vegetable, fruit, raw fish, fermented fish, glutinous rice, meat, betel nut, fermented meats, high nitrate foods and rice. Seven studies focused on 11 nutrition related indicators, including overweight, obesity, diabetes mellitus, glycemic index rate, glycemic load rate, every 5 unit increment of BMI, every 10 cm increment of waist circumference, every 0.1 unit increment in waist-to-hip ratio, triglycerides, HDL cholesterol and Non-HDL cholesterol.
Table 2 The relationship between dietary factors and biliary diseasesTable 3 The relationship between nutrition related indicators and biliary diseasesTable 4 The relationship between alcohol consumption and biliary diseasesGallbladder cancerIn the studies we included, there were some dietary factors, such as all spicy food [29], chili pepper [29] and tea [22] intake, which were not related to the risk of gallbladder cancer.
Type two diabetes mellitus was associated with an increased risk of gallbladder cancer (RR = 1.56, 95% CI 1.36–1.79) [41]. Compared with normal subjects, T2DM increased the risk of gallbladder cancer by 56%. Overweight and obesity are also risk factors for gallbladder cancer. Being overweight increased the risk by 17% (RR = 1.17, 95% CI 1.07–1.28), while in obesity this figure rose to 62% (RR = 1.62, 95% CI 1.49–1.75) [42]. These results are in good agreement with the results of subgroup analyses of different study models (case control and cohort studies) in the meta-analysis.
Bile duct cancerThe consumption of tea was related to a reduced risk of bile duct cancer [36] (RR = 0.66,95% CI 0.48–0.85), although this was not apply to gallbladder cancer. According to dose–response analyses, the risk of bile duct cancer decreased by 4% with each additional cup of tea per day (RR = 0.96, 95% CI 0.93–0.98, p = 0.001). Due to the limited number of studies, no further study has investigated the effect of different types of tea intake on reducing the risk of bile duct cancer.
For fruit and vegetable consumption, we found that they have a significant effect on reducing the incidence of bile duct cancer [37]. In terms of vegetables consumption, the summary RR was 0.48 (95%CI 0.22–0.74). For dose–response analysis, every 100 g increment of vegetables consumed per day was associated with a 69 percent reduction in the risk of bile duct cancer (RR = 0.31, 95% CI 0.20–0.47, p < 0.001). In term of fruits consumption, the summary RR was 0.47 (95% CI 0.32–0.61) and the summary RR every 100 g increment a day was not statistically significant. Although the summary data show that vegetable and fruits consumption can reduce the risk of bile duct cancer, a cohort study in this meta-analysis showed that neither consumption were associated with a reduced risk of bile duct cancer. Therefore, the relationship between vegetable or fruit consumption and the risk of bile duct cancer remains to be further evaluated by larger and more comprehensive clinical studies.
In addition, some studies from Thailand have shown that eating raw fish [30] (RR = 2.54, 95% CI 1.94–3.35, p < 0.00001) and high-nitrate foods [23] (RR = 1.41, 95% CI 1.05–1.91, p = 0.024) increases the risk of bile duct cancer. Because these studies are meta-analyses of retrospective case–control studies and the sample size is small, the evidence they can provide is very limited. There was no obvious significant association of coffee [13], fermented fish [30], glutinous rice [30], meat [30], betel nut [30], fermented meats [23] and rice [23] consumption with bile duct cancer.
Similarly, some nutritional indicators are also associated with the risk of bile duct cancer. Both overweight and obesity increase the risk of eCCA [42]. Overweight increased the risk of eCCA by 26% (RR = 1.26, 95% CI 1.14–1.39), while obesity increased the risk by 48% (RR = 1.48, 95% CI 1.21–1.81). Although subgroup analysis of case–control studies showed that overweight was not associated with the risk of eCCA, we had more reason to believe the evidence provided by cohort studies. Obesity and diabetes are also risk factors for iCCA [24], in obese and diabetic subjects, the RR values of iCCA were 1.49 (95%CI 1.32–1.70, p < 0.001) and 1.53 (95%CI 1.31–1.78, p < 0.001) respectively.
Cholecystolithiasis/gallbladder diseasesSince many studies did not separate cholecystolithiasis from other gallbladder diseases such as acute cholecystitis, some of the studies we included may not be limited to cholecystolithiasis.
Although studies have confirmed that coffee consumption has no obvious relationship with the incidence of biliary cancers, coffee consumption is a protective factor in the formation of gallstones [39]. Overall, the combined RR was 0.83 (95% CI 0.76–0.89), and each additional cup of coffee consumed per day was associated with a 5% (RR = 0.95, 95% CI 0.91–1.00, p = 0.049) reduction in cholecystolithiasis risk. As for the relationship between vegetable and fruit consumption and cholecystolithiasis, current evidence suggests that vegetable consumption is associated with a 17% (RR = 0.83, 95% CI 0.74–0.94) lower risk and fruit with a 12% (RR = 0.83, 95% CI 0.83–0.92) lower risk [40]. Moreover, there is a dose–response relationship between the intake of vegetables and fruits and the risk of disease, that is, for each additional 200 g per day, the corresponding risk of disease will be reduced by 4% (RR = 0.96, 95% CI 0.93–0.98, p = 0.001) and 3% (RR = 0.97, 95% CI 0.96–0.98, p = 0.001).
In addition, some nutritional indicators may be related to the occurrence of gallstone, such as Glycemic index rate [25] (RR = 1.26, 95% CI 1.13–1.40, p < 0.0001), Glycemic load rate [25] (RR = 1.41, 95% CI 1.25–1.60, p < 0.0001), diabetes mellitus [33] (RR = 1.41, 95% CI 1.56, 1.26–1.93), every 5 unit increment of BMI [34] (RR = 1.63, 95% CI 1.49–1.78), every 10 cm increment of waist circumference [34] (RR = 1.46, 95% CI 1.24–1.72), every 0.1 unit increment in waist-to-hip ratio [34] (RR = 1.44, 95% CI 1.26–1.64) and non-HDL cholesterol [26] (RR = 1.19, 95% CI 1.07–1.32).
Alcohol consumption and biliary tract diseasesOur study included eight meta-analyses that discussed the relationship between alcohol consumption and biliary diseases.
In these studies, three meta-analyses reported the relationship between alcohol consumption and gallbladder cancer [21, 27, 31]. Bagnardi et al. [21] defined daily alcohol intake ≦12.5 g, ≦50 g and ≧50 g as light, moderate, and heavy alcohol consumption, respectively. Their meta analysis found that heavy drinking was associated with a marked increased risk of gallbladder cancer (RR = 2.64, 95% CI 1.62–4.30). The association between alcohol consumption and gallbladder cancer risk was not statistically significant for light (RR = 1.23, 95% CI 0.84–1.83) to moderate (RR = 0.88, 95% CI 0.68–1.13) drinkers. In a meta-analysis based on cohort studies, Emma E. McGee et al. [27] further divided the aggregated cohort studies into 6 subgroups (0,0–0.5,0.5–1,1–3,3–5, > 5 drink/d), based on drink/d (14 g of ethanol/d). The subgroups were compared with the 0 drink/d group and no statistical association was found between alcohol consumption and the risk of gallbladder cancer. There was no dose–response effect between alcohol consumption and gallbladder cancer, either. In another meta-analysis, Li et al. [31]. found a 30% reduction in gallbladder cancer among drinkers compared to non-drinkers (OR = 0.7, 99%CI 0.49–1.00, p = 0.009).
In the study of intrahepatic cholangiocarcinoma, Emma E. McGee et al. [27] found that the risk of iCCA was reduced in patients with > 0–0.5 drink/d compared with non-drinkers (HR = 0.79, 95%CI 0.62–1.00). When drinking > 5 drink/d, The risk of iCCA was 1.35 times higher than that of non-alcohol consumption (HR = 2.35, 95%CI 1.46–3.78), and there was a dose–response effect between the risk of iCCA and the amount of alcohol consumed (every 1drink/d increment, HR = 1.03, 95%CI 1.01–1.06, p = 0.04).Similarly, in the meta-analysis conducted by Clements et al. [1]., drinkers had an approximately 2.15-fold increased risk for iCCA (OR = 3.35, 95%CI 2.24–4.41) and a approximately 0.75-fold increased risk for eCCA (OR = 1.75, 95%CI 1.20–2.55) compared to non-drinkers.
As for cholecystolithiasis or gallbladder disease, although drinking is a risk factor for biliary cancers, Byung et al. [38]. found that drinking can reduce the risk of cholecystolithiasis by 16% (RR = 0.84, 95% CI = 0.79–0.89). At the same time, compared with non-drinkers, the risk of cholecystolithiasis decreased gradually with the increase of alcohol consumption. In mild, moderate and severe drinkers, the risk decreased by 4% (RR = 0.96, 95% CI = 0.94–0.99), 20% (RR = 0.80, 95% CI = 0.75–0.85) and 34% (RR = 0.66, 95% CI = 0.56–0.79) respectively. Similarly, we also found the same conclusion in the study of Jiantao Wang et al. [28] (Alcohol consumption highest vs. lowest, RR = 0.62, 95%CI 0.49–0.78). In addition, they also studied the consumption of different types of alcoholic beverages and the risk of cholecystolithiasis. The results showed that increased consumption of beer (RR = 0.64, 95%CI 0.52–0.78), wine (RR = 0.72, 95%CI 0.54–0.96), and liquor (RR = 0.71, 95%CI 0.64–0.85) tended to reduce the risk of gallstones.
Heterogeneity, publication bias and small study effectOf all the items we summarized (all items in Tables 2, 3 and 4), 52 items presented low heterogeneity (I2 < 25%); 36 items had moderate-to-high heterogeneity (25% < I2 < 75%), and 19 items had very high levels heterogeneity (I2 > 75%). In addition, there were 7 items that did not report heterogeneity. For evidence with significant heterogeneity (p < 0.05), the quality of evidence will be degraded in the evaluation of evidence quality.
This umbrella review used Egger’s test to summarize publication bias and small study effects in meta-analyses. Of the 24 meta-analyses, 7 studies did not measure publication bias, 3 reported significant publication bias, and the remaining did not report significant publication bias (Table 1).
AMSTAR2 and GRADE classificationThe methodological quality of the meta-analyses included in our study were assessed using AMSTAR2 scale, and the results of the review were rated as high, moderate, low, and critically low. Overall, the vast majority (21 studies, 87.5%) of methodological qualities of the meta-analyses were assessed as “critically low” by AMSTAR2 scale (Table 5). The remaining three meta-analyses were assessed as “low” and no one was assessed “moderate” or “high”.
Table 5 Methodological quality of the systematic review and meta-analyses were assessed using the AMSTAR2 scaleSince the studies we included were all meta-analyses based on retrospective studies, all evidence was first lowered by two grades, from high level to low level during GRADE evaluation. Next, we decided whether to continue to downgrade the evidence according to whether there was risk of bias, indirectness, inconsistency, imprecision and publication bias. After checking whether there were large effects, dose–response gradients and plausible confounding of evidence, whether to upgrade the level of evidence and finally determine the strength of each evidence level was decided.
In this umbrella review, we summarized 83 independent outcomes (Table 5). Regarding the risk of bias, 44 outcomes were downgraded due to inadequate control for confounding factors (including inaccuracy in measuring all known prognostic factors; Prognostic factors were not matched and/or not adjusted in the statistical analysis). We judged the imprecision of evidence by the 95% confidence interval of each evidence and the optimal information size (OIS). If the sample size of evidence was lower than the OIS standard, the confidence intervals contained invalid values, or the confidence intervals did not exclude significant benefits or harms (95%CI contained 1, with lower limit < 0.75, upper limit > 1.25), the quality level of evidence would be reduced. We found a total of 38 outcomes of Imprecision and downgraded one level. The inconsistency and publication bias were mainly evaluated according to the I2 and Egger’s test of meta-analyses included in our study. In our study, 35 outcomes were downgraded due to inconsistencies and 45 outcomes were downgraded due to suspected publication bias. None of the outcomes was downgraded due to indirectness. In terms of upgrading factors, seven of the outcomes were upgraded due to large effect (Relative effect > 2 or < 0.5), 14 due to dose response gradient, and 0 due to plausible confounding.
In short, among 83 independent outcomes, 5 were rated as moderate, 16 as low, and the rest as very low (Table 6).
Table 6 AMSTAR2 and GRADE classification of the evidence
留言 (0)