
記住我






An institution based unmatched case–control study was conducted among antiretroviral therapy users in WCUNEMMCSH and HHC, Hossana, Hadiya zone, Southern Nations, Nationalities and Peoples’ Region (SNNPR). The study was conducted from February 2021 to May 2021.
Source populationThe number of people living with HIV recorded and enrolled in ART were 1587. According to institutional data, out of 1587, 867 HIV positive sexually active women were on antiretroviral therapy. The source population consisted of sexually active HIV positive women in the age group of 18–49 years attending chronic HIV/AIDS care clinic.
Study populationCaseSexually active HIV positive women in the age group of 18–49 years used dual contraceptives (barrier methods, i.e., male and female condoms) during the study period and attended ART follow-up clinics in WCUNEMMCSH and HHC, Hossana.
ControlSexually active HIV positive women in the age group of 18–49 years did not use dual contraceptives (used either one barrier condom or any other contraceptive method) during the study period but attended ART follow-up clinics in WCUNEMMCSH and HHC, Hossana.
Inclusion criteriaCaseAll sexually active HIV positive women in the age group of 18–49 years used dual contraceptives (barrier methods, i.e., male and female condoms) during the study period and attended ART follow-up clinics in WCUNEMMCSH and HHC, Hossana.
ControlAll sexually active HIV positive women in the age group of 18–49 years did not use dual contraceptives (used either one barrier condom or any other contraceptive method) during the study period but attended ART follow-up clinics in WCUNEMMCSH and HHC, Hossana.
Exclusion criteriaIndividuals unable to communicate verbally/seriously ill at the time of data collection.
Sample size determination and sampling techniquesSample size determinationThe sample size was calculated using Epi info 7.0 considering control to case ratio of 3:1, expected percentage of controls exposed 31%, expected percentage of cases exposed 50.2%, 95% level of confidence, 80% of the power and 10% of non-responders [16]. Finally, a total sample size of 321 individuals (80 cases and 241 controls) was calculated. The calculated sample size was in line with reference to a previous study of determinants of dual contraceptive utilization among HIV positive women [17].
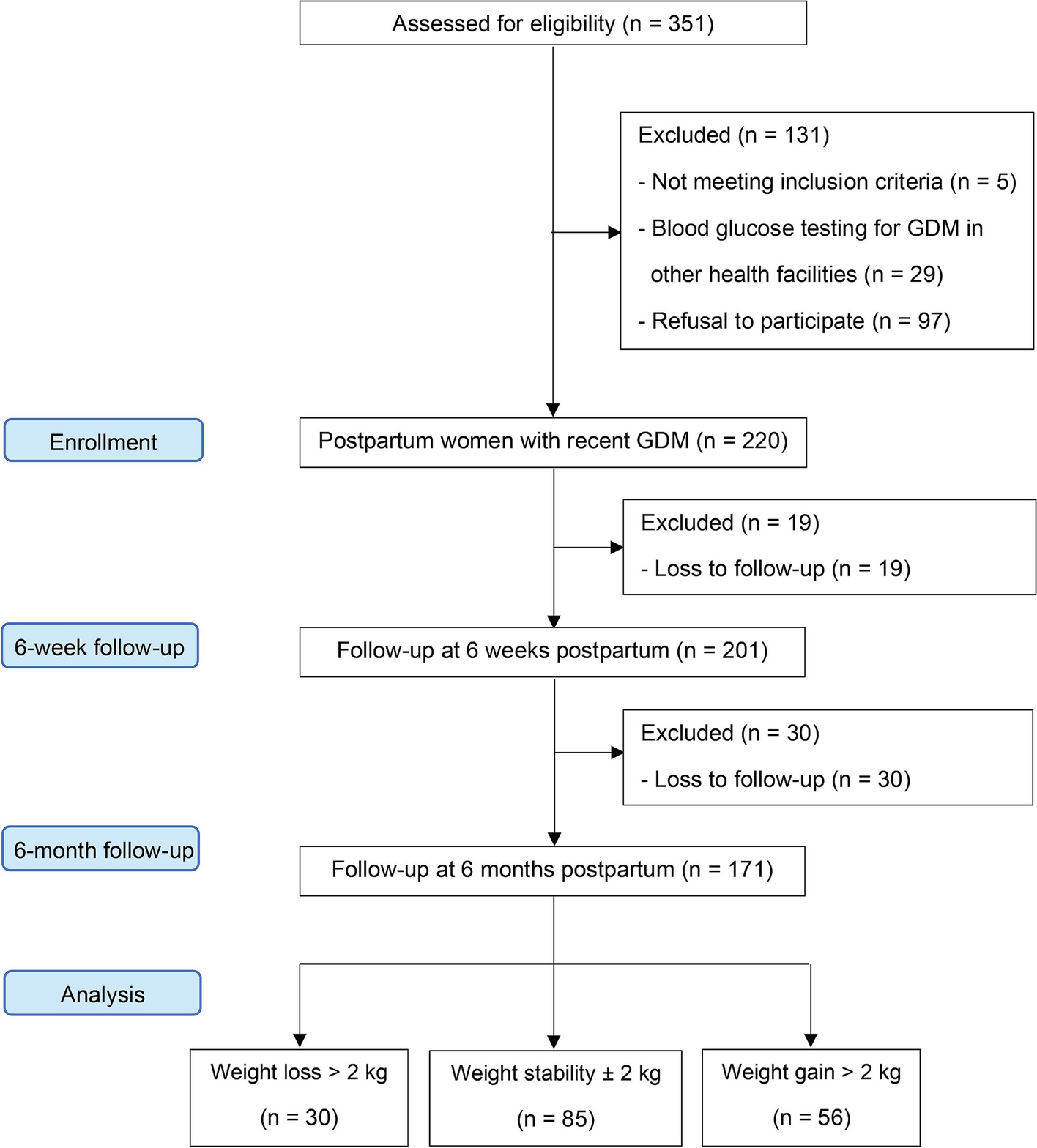
Sampling procedures/techniquesHossana town has two public health facilities: i) Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital and ii) Hossana Health Centre. The sampling frame for cases and controls from selected public health center or hospital was obtained from ART registration records. The sample size was proportionally distributed to each health facility based on Health Management Information System (HMIS) and reported existing case and control flow in the previous three months (Fig. 1). Considering pre-specified sample size in each arm (cases and controls), we selected the cases purposefully from ART registration records and controls were selected using random sampling techniques until the required sample size was achieved.
Fig. 1
Schematic representation of sample size distribution in WCUNEMMCSH and HHC
Study variablesDependent variableDual contraceptive utilizationThis refers to the sexually active HIV positive women who used two contraceptives simultaneously [i.e.., barrier method (male and female condom)] used in every sexual encounter in the last six months preceding the study.
Independent variablesSocio-demographic characteristicsThese include age, educational status, marital status, place of residence, ethnicity, religion, occupation, and wealth index.
Service-related variablesThese include counselling about contraceptive use, accessibility of family planning services, satisfaction and duration of ART, discussion with their partners, CD4 count, time of HIV diagnosed, side effects, HAART users & knowledge of contraceptive use as well as knowledge scores.
Social and cultural variablesThese variables include religious influence, peer support and support of the partner.
Reproductive health variablesThese include parity, gravidity, number of live children, discussion with husband, discussion with health care providers, family planning counselling, pregnancy initiation and experience of contraceptives.
Risky sexual behaviour variablesThese include sexual intercourse in past 6 months without using condom and having multiple sexual partners.
Data collection procedures and quality controlA structured questionnaire [17,18,19] was used to collect data and modified according to local study settings. The questionnaire consisted of sociodemographic and economic characteristics (age, women’s and husbands’ education level, marital status, wealth index and place of residence), reproductive variables (parity, gravidity, number of live children, discussion with husband, discussion with health care providers, family planning counselling, intention for pregnancy, knowledge of contraceptives), risky sexual behavior patterns (sexual intercourse in the past six months without condom usage and having multiple sexual partners) and factors related to HIV and STIs (clinical WHO staging, disclosure of HIV status, CD4 count, time of HIV diagnosed and HAART user). The data were collected through face-to-face interviews using structured and pre-tested questionnaire. The questionnaire was initially prepared in English and translated to Amharic and local language i.e., Hadiyissa and back to English to ensure consistency of the content. Five nurses and one public health officer (PHO) were recruited as data collectors and supervisor, respectively. Two day’s training was provided to data collectors towards interviewing techniques and ethical concerns. A pre-test was conducted on questionnaire on 5% of the total sample size in similar settings (Gimbichu district hospital). An alpha value of 0.67 was observed and minor modifications were done in the questionnaire. The data collection was closely supervised by a supervisor and principal investigator daily.
Operational definitionsCasesSexually active HIV positive women in the age group of 18–49 years used dual contraceptives (barrier methods, i.e., male and female condoms) for ≥ 6 months and attended ART follow-up clinics.
ControlsSexually active HIV positive women in the age group of 18–49 did not use dual contraceptives (barrier methods, i.e., male and female condoms) in past 6 months but attended ART follow up clinics.
Accessibility of family planning servicesThis refers to the distance from patients’ residence to the health institution (i.e., 5 km or ≤ 30 min walking time was considered as accessible) [20].
Knowledge of contraceptive useThis belongs to a total of five dichotomized questions; 1 an incorrect answer and 2 for correct answer about contraceptive use. Women who answered and scored median or above were considered to have good knowledge and below median score were considered to have poor knowledge [21].
Data processing and analysisThe data were entered, sorted, edited, and cleaned for missed values. The data were analyzed using SPSS version 20.0 for further analysis. The correlation between dependent and independent variables was primarily analyzed by bivariate analysis to find any significant association. A P-value < 0.25 observed during bivariate analysis were further processed for multivariate analysis to check the probable effect of confounders. A P-value < 0.05 was considered statistically significant.
Ethical considerationThe ethical clearance was obtained from an ethical review committee of College of Medicine and Health Sciences. Written permissions were obtained from higher authorities of WCUNEMMCSH and Hossana Health Center. A verbal and written informed consent for participation was obtained from each study participant. Before enrolling any of the eligible study participants, the purpose, benefits, and confidential nature of the study was described. The discussions between the data collectors and the respondents solely took place in a separate room. The confidentiality of study individuals was maintained, and all the data were de-identified before analysis.
留言 (0)