In the present study, we used a moderately large sample size to investigate the clinical and molecular imaging characteristics of patients with RR-DTC and the ability of these characteristics to predict RR-DTC, with the overall aim of establishing an effective multivariable prediction model for RR-DTC; such a model may prove valuable in further optimizing the treatment strategy in the early stages of metastatic DTC. Our study found that nine predictors were significantly related to RR-DTC based on univariate analyses. In addition, four independent predictors of RR-DTC were confirmed in multivariate logistic regression analysis: age at diagnosis ≥ 48 years, recurrence between the operation and iodine-131 treatment, the uptake of 18F-FDG, and the site of metastasis. According to the ORs, different scores were assigned to predictors that were positively correlated with RR-DTC, and we then established a 52-point scoring system. Finally, we determined that 10 points was the optimal score for predicting RR-DTC, and the associated AUC was 0.898. The scoring system had a higher predictive value than any other single independent predictor. Its sensitivity, specificity, and Youden index values were 76.0%, 93.0%, and 0.69, respectively, at 10 points. RR-DTC and non-RR-DTC were determined with 10 cutoff values. Subsequently, 169 individuals were correctly classified as RR-DTC, 168 individuals were correctly classified as non-RR-DTC, 13 individuals were misclassified as RR-DTC, and 54 individuals were misclassified as non-RR-DTC, with an accuracy of 83.41%. Subsequently, the visual prediction RR-DTC nomogram model constructed in this study had a c-Index of 0.9. The first behavioral score scale calculates the corresponding score of each risk factor according to the situation of each patient, and then add the scores to obtain the total score. Then, the corresponding score point was found in the total score scale, and the corresponding probability scale coordinate below the vertical was the probability of suffering from RR-DTC.
There have been many studies on the prognostic factors associated with RR-DTC; however, the identification of predictors of RR-DTC rather than pure prognostic factors may be helpful in changing prognostic strategies and outcomes [13]. In a previous study, Li et al. explored RR-DTC predictors and found that certain factors were highly correlated with RR-DTC, including smoking, tumor type, extrathyroid extension, pN stage, and number and rate of lymph node metastasis [12]. However, in view of the latest advances in genetic analysis of thyroid tumors, including molecular methods, we have incorporated molecular imaging characteristics into our prediction model for RR-DTC.
In our study, 55.2% (223/404) of patients developed RR-DTC, and 28.7% (116/404) had distant metastasis, which was consistent with the literature reporting that 7–23% of patients with DTC had distant metastasis [14]. However, 77.6% (90/116) of patients with distant metastases developed RR-DTC in our study, which was higher than the corresponding rate of a previous work showing that 25–50% of patients with distant metastases developed RR-DTC [15]. One explanation is that our study only comprised patients with metastatic DTC who had undergone PET/CT imaging, the use of which depends on the judgment of their physician; meanwhile, patient decisions were also an important factor, which may not fully reflect the true clinical features of metastatic DTC. According to Schlumberger et al. [7], even after an adequate stimulation by thyroid-stimulating hormone and in the absence of excess iodine, only two-thirds of patients with metastases show substantial radioactive iodine uptake, and only 42% of them achieve a cure. According to the definition of RR-DTC, the remaining 58% of patients who are not cured would be classified as having RR-DTC, which was similar to the rate observed in our cohort (55.2%). The possible explanation for our high RR-DTC ratio is that lymph node metastasis accounts for the majority (70.5%); some metastatic lymph nodes take iodine the first time and do not take iodine the second time, but the lesions persist, while some metastatic lymph nodes do not take iodine the first time. In addition, there are also patients with multiple sites of metastasis; if one lesion does not receive iodine, patients are also judged to have RR-DTC.
Using univariate analysis, our study found age to be an important factor. Prior studies have shown that the adverse effect of age on prognosis gradually increases with each decade, especially after 40–45 years [16, 17]. Different studies use different cutoff values; in this study, the cutoff age was 48 years. In the Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC) staging system, an age threshold of 45 years is one of the main criteria [13]. It is inferred from this that an older age results in a greater possibility of RR-DTC development, leading to an increased risk of death [18]. The cutoff point value of diagnostic age was changed from 45 to 55 years in the eighth edition of the AJCC TNM staging system. Wassermann et al. showed that age ≥ 60 years significantly affected a patient's cancer-specific survival after the detection of RR-DTC [19]. Studies have shown that some elderly men have more advanced disease, lower disease-free survival, and higher mortality than female patients [20, 21]. However, whether sex can predict the occurrence of RR-DTC remains unknown; our results showed that sex was not a statistically significant factor. Operation frequency was another predictive factor. Cervical scar adhesion, unclear anatomical level, recurrent external invasion of residual cancer after the initial operation, and the incidence of complications reduce the possibility of complete resection of the tumor, thus, increasing the risk of RR-DTC. Some studies have suggested that some pathological subtypes of thyroid cancer are more likely to develop into RR-DTC, such as follicular thyroid cancer, Hürthle cell carcinoma, and poorly differentiated thyroid cancer [22, 23]. One meta-analysis also confirmed that the pathological subtype was a predictor of RR-DTC [6]. However, our results showed that histological subtype was not a statistically significant factor, although there was a relatively low proportion of adverse pathological subtypes in our study, which may explain this finding.
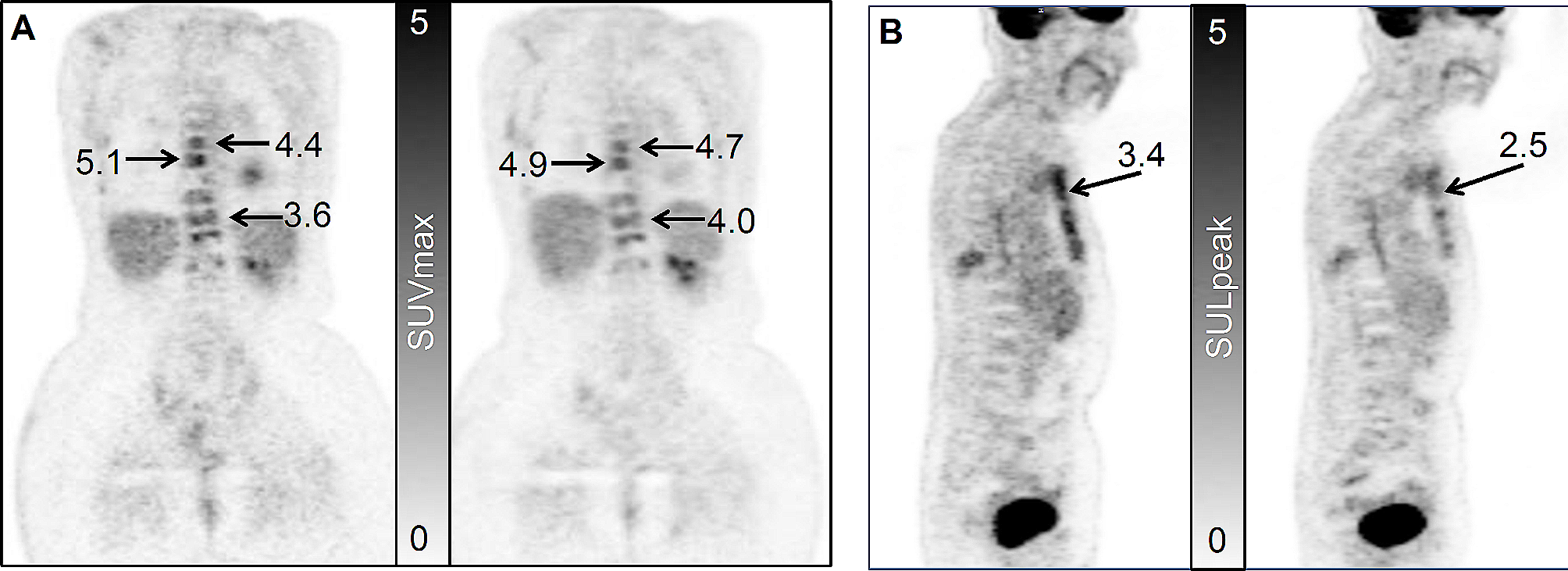
Next, we discuss the conclusions of the molecular imaging in RR-DTC. In our study, 18F-FDG uptake was a predictor for RR-DTC, whereas iodine uptake was not. This was surprising, as three out of five definitions of RR-DTC require lesions to be RAI negative, but RAI uptake was not a predictor. A possible reason is that although the definition of RR-DTC involves whether iodine is ingested or not, the definition of RR-DTC contains a wide range of contents, and it may become RR-DTC regardless of whether iodine is ingested or not. Therefore, this variable was not selected in the screening. This finding is consistent with the corresponding of a study by Kang et al., who showed that RAI uptake of metastasis was not correlated with RR-DTC, but FDG uptake was negatively correlated with RR-DTC [10]. Previous studies have shown that despite repeated RAI treatment, more than 50% of patients eventually show disease progression and are ultimately considered refractory to RAI [24]. Moreover, more courses of prior TSH stimulation before iodine-131 administration, as well as more administration of probably overused iodine-131, may lead to a higher tumor burden [25,26,27]. Therefore, they may be of great value in the early identification of patients with RR-DTC and in combination with other therapeutic modalities [27, 28]. Early 18F-FDG imaging can predict the occurrence of RR-DTC and help make an accurate prognosis because RR-DTC is closely related to iodine treatment response. When FDG PET is used in conjunction with RAI whole-body scan (WBS), we can obtain the metabolic information of the two radioactive tracers and infer the differentiation status of thyroid carcinoma at the same time. Many studies have shown that regardless of the affinity of iodine-131, FDG uptake is an adverse prognostic factor [10, 29, 30]. Incidentally, thyroglobulin response can also predict RR-DTC [18], but it lags behind molecular imaging, so it was not included in our prediction model. However, the advantage of 18F-FDG PET/CT lies in its ability to identify and locate tumor lesions. Furthermore, an SUVmax of 2.5 points was selected as the threshold value for positive PET/CT results in this study. This value was used because it is generally believed that the SUV is more likely to indicate malignant lesions above 2.5–3.0 points, while benign lesions < 2.0 points are likely larger. Between these two values, the benign and malignant nature of the lesion cannot be determined, and the lesion is classified as a suspicious lesion [31]. Therefore, this standard has been selected in many studies in the literature [32,33,34], and we did the same in our study. In one research [35], it was found that the mean SUVmax of the suspected lesions after performing PET/CT in patients with differentiated thyroid cancer with elevated thyroglobulin levels and negative 131I whole-body scan findings was 2.9 ± 4.5 points.
In univariate analysis, some variables could not be used as independent factors of the disease. Therefore, multivariate analysis was conducted, and several scoring systems for predicting disease-specific mortality based on clinical and pathological prognostic factors were developed [13]. This research may help establish a predictive scoring system for RR-DTC that incorporates molecular imaging.
Currently, the diagnosis of RR-DTC takes a long time because it relies on the trend of thyroglobulin (Tg) and WBS after multiple RAI treatments, combined with relevant imaging examination results. If the development of RR-DTC was determined according to the normal procedures, it would require 4–77 months in our study, with a median of 6 months. This study contributes to the literature as, to our knowledge, it is the first to show that the occurrence probability of RR-DTC can be predicted at an early stage, without waiting for ≥ 6 months. After obtaining the patient's history and completing the relevant examination before the first treatment of RAI, the prediction of RR-DTC can be made using our scoring system and nomogram. Several prognostic scoring systems have been developed for predicting disease-specific mortality based on the following clinical and pathological prognostic factors: AGES (Age, tumor Grade, Extent, and Size) [36], AMES (Age, distant Metastases, Extent, and Size of primary tumor) [37], MACIS (distant Metastases, Age, Completeness of surgery, Invasion of extrathyroidal tissues, and Size of the primary tumor) [38], De Groot's Clinical Classification [39], and National Thyroid Cancer Treatment Cooperative Study Classification [40]. Studies on the use of nomograms for thyroid cancer include those determining the prognostic factors of death because of specific and other causes in patients with DTC and those assessing the preoperative diagnosis of sonographically indeterminate/suspicious lymph node metastasis in such patients by ultrasound [41, 42]. However, only a few studies have reported the prediction of RR-DTC by nomogram. We believe that early FDG PET/CT examination can be beneficial to patients with metastatic DTC. First, we can identify as many metastatic lesions as possible. Second, if the patient shows FDG-positive results, we suggest comprehensive intervention as soon as possible. In our study, one patient with multiple site metastasis showed FDG PET/CT-positive findings, as well as positive findings observed on post-RAI WB therapy scintigraphy after iodine treatment. After two sessions of iodine treatment, good outcomes were noted, the solid metastasis tumor was reduced, and the biochemical improvement was obvious. After 2 years, progress began to appear, and treatment with specific drugs was initiated. Unfortunately, this patient has a poor prognosis. If FDG PET/CT results are positive, research will be conducted to ascertain whether early intervention can prolong the time of disease progression. We hope to show that early PET/CT examination can be beneficial for patients in clinical practice. Details of the other three factors (i.e., age at diagnosis, recurrence between the operation and iodine-131 treatment, and the site of metastasis) can be obtained from patient history data and associated imaging evaluation (ultrasound scan of the neck, chest CT, and other conventional imaging) if the patient did not undergo PET/CT examination prior to treatment. These factors also have some clinical significance in predicting RR-DTC in some patients. For example, a postoperative differentiated thyroid cancer patient older than 48 years who had a recurrence of the tumor before the first iodine-131 treatment has > 90% probability of developing RR-DTC in the future. If the current examination also found more than two sites of metastasis, his probability of developing RR-DTC in the future would be > 99%.
Given its retrospective design, this study is inherent to selection bias. Although this was a retrospective study, our patients were actually divided into two categories. Our team recommended PET/CT examination for patients with multiple metastases and significantly elevated Tg levels from 2014 to 2018. In total, 44 out of 404 (10.9%) patients were enrolled in this stage. With improvements in clinical experience and professional knowledge, we recommended PET/CT examination for the following patients since 2019: patients with structural metastases indicated by imaging before RAI treatment; those with unexplained Tg level elevation > 10 ng/mL after DTC and before RAI treatment; or those in whom pre-RAI imaging examination and stimulating Tg did not indicate metastatic tendency, but the RAI suggested the presence of metastatic lesions. Thus, these patients were advised to complete PET/CT within 1 week to determine the prognosis. At this stage, 360 out of 404 (89.1%) patients were enrolled, indicating that our data represent 89% of the patient cohort with metastatic DTC. Therefore, the selection bias offset had limited influence on our results.
This study had some limitations. First, few metastases could be confirmed pathologically because of the clinical limitations; this needs to be addressed when we study tumor metastasis. In this study, approximately 11% of our patients' metastases were pathologically obtained, including lymph node, lung, and bone metastases. Other metastases were diagnosed by comprehensive imaging, serological indicators, clinical symptoms, and follow-up examinations. At future follow-up examinations, we should try our best to obtain the pathology of the metastatic lesions of the patients, and at the same time, to perform genetic testing of the metastatic lesions to guide the comprehensive treatment plan in the future. Second, the findings have not been verified at other hospitals. In this study, the sample curve is based on random sampling of the full sample using the bootstrap method (100 interactions). There is a 90% chance that the prediction will be correct. Patients from other centers can be selected for validation in the future. Thus, further studies should be conducted to examine the extrapolation of the model. Finally, the genetic status was not included at the very beginning of the research. Approximately 52% of the patients in this study underwent genetic testing. As not all patients underwent genetic testing, statistical factors were not included in this experiment. Some studies have shown that molecular markers provide a useful insight into the role of predicting the occurrence of RR-DTC, and this is an area for making future research efforts. In the future, we will conduct a prospective study of molecular markers to predict RR-DTC.




留言 (0)