
記住我








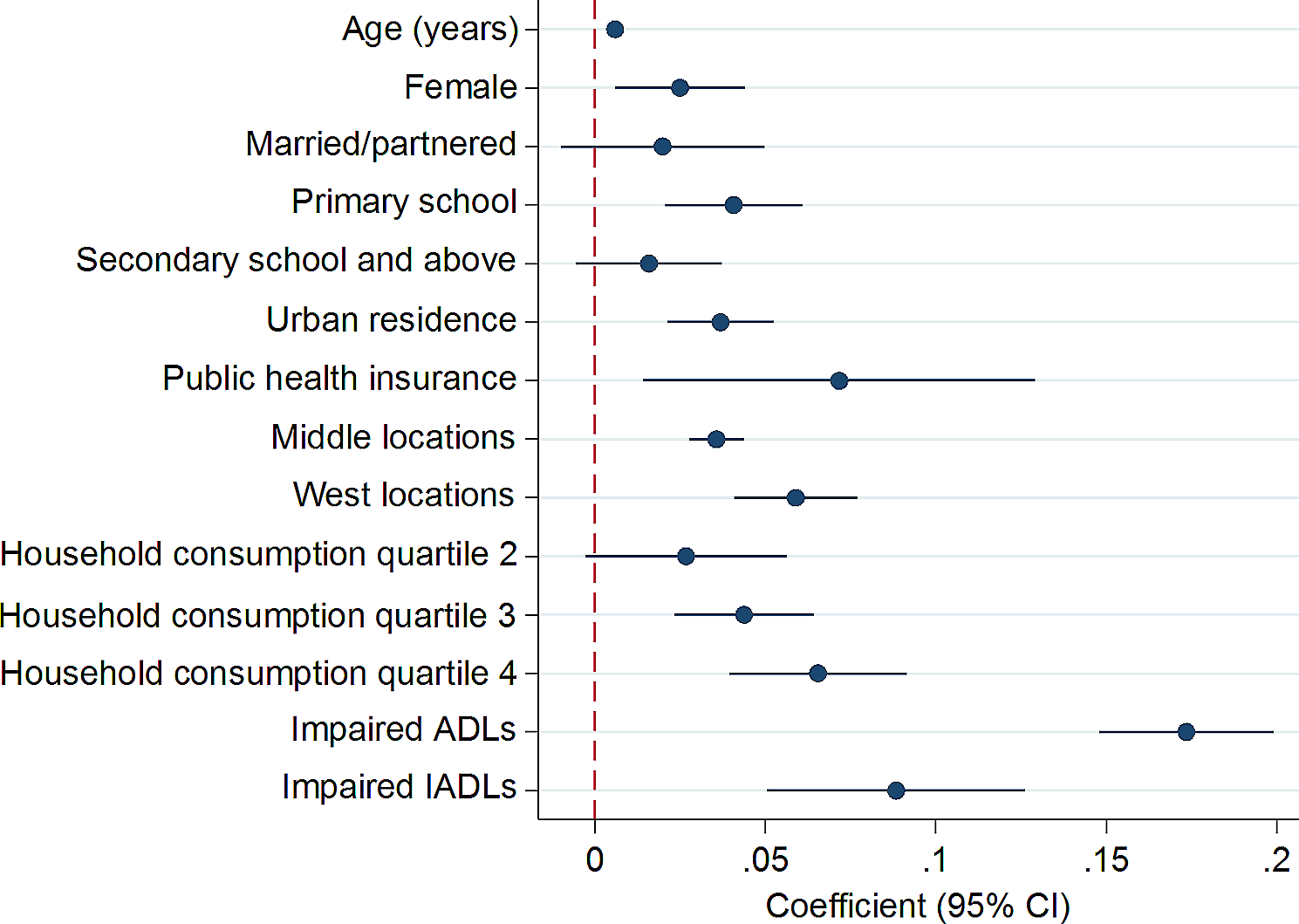
A total of 5 participants completed the qualitative interviews. Saturation was achieved. The interviews were conducted in English by an African research assistant at the participants’ home (as per request of the family). All the patients had Sickle Cell Disease Hg SS. The majority were male (80%), and born outside of Canada (80%). Please see Table 1 for demographics. Quality of life data from inventories is combined with interviews. Please see Fig. 2 for mean scores from the inventories between 6 months and 1 year.
Fig. 2
Parent and Adolescent QoL at six months and one year post HSCT as measured by PedsQL Inventories™
See Fig. 1 for study timelines.
Medical chart reviews pre-HCT revealed that all patients experienced sickle cell complications which are presented in Table 2.
Table 2 Pre-HCT complicationsMedical chart reviews post-HCT demonstrated that all 5 patients had successful donor engraftment, achieved donor HbS levels, and none had GVHD. There were no sickle related post-HCT acute events. Four of the six patients had viral infections that were resolved.
Two cases (Patient 1 and 2) are presented below as examples of the data.
Case onePatient 1 was born in Africa and diagnosed at one year of life. His pre-HCT life in Africa was characterized by intense physical pain, fevers, and frequent hospitalizations. He appeared physically pale and underweight, with jaundiced eyes and a protuberant stomach. His poor state of health contributed to insomnia, school absenteeism, and physical inactivity. Fear of premature death posed significant psychological stress, which was aggravated in the local community by rumours that portrayed him as “a child on death row.” Stigma from extended family and peers that misrepresented SCD as a contagion accentuated psychological stress, causing him to be socially isolated. During this time, a significant portion of the family income went to paying for healthcare, which brought economic and psychological stress on the family. For this reason, Patient 1 contemplated suicide because he began to view himself as a burden to his family. His parents decided to seek help in Canada, leaving behind their respective successful professional careers.
In Canada, the family experienced downward socioeconomic mobility but were hopeful for a better future for their son. He was hospitalized 5 times in 8 months, prompting consideration of HCT and subsequently transplanted at 17 years of age. While the transplantation went smoothly, the medical preparation was difficult. In the immediate post-HCT period, he experienced several health and social concerns, including hair loss, amnesia, and isolation. He described this as a difficult period that adversely affected his social life. The HCT and its immediate aftermath reactivated thoughts of premature death and doubts about the procedure’s long-term therapeutic benefits. His mother lost her job due to their stay in the hospital. Accordingly, patient 1 and his family described their QoL during the HCT and the period of isolation afterwards to be unsatisfactory.
Patient 1 and his family reported an improved QoL 6 months after HCT. He reported an ability to sleep, walk, and exercise without the usual pain that characterized his pre-HCT life. He described his memory as “weak but improving.” His experience of good health and happiness was greatly enhanced 12 months post-HCT, as his SCD crisis and hospitalizations had ceased. These post-HCT changes have brought about tremendous QoL improvements. When asked whether he would consider undergoing HCT a second time he stated, “Having the transplant is the best decision that my parents ever made.”
Case twoPatient 2 was born in Canada to African immigrant parents, and was 17 years old at the time of her transplant. As a single parent household, Patient 2’s frequent hospitalizations shifted parental attention away from her younger siblings. She experienced stigma and social exclusion from family in Africa, and was predicted to die prematurely, which resulted in intense sadness for her mother and siblings.
When doctors mentioned HCT during one of her hospitalizations, she resisted and even attempted to dissuade her sister from being the donor. She was frightened of transplant and its side effects, despite a detailed explanation from doctors. Her main concern was the possibility of infertility. Six months post-HCT, Patient 2 and her family reported improvements in her QoL. She could breathe better and perform physical tasks without pain; her eye colour changed; her hair grew back; and she started University. Unfortunately, her menstrual cycle was irregular. Her one-year post-HCT experience was characterized by a crisis-free life, which was capped off by a feeling of psychological relief. Her social life improved as her extended family in Africa initiated relationships with her. Overall, Patient 2 and her family expressed joy at the transplant outcomes, stating that “It was a good decision because my life is changed forever.”
Between the two patients, significant improvements in the physical and psychosocial domains of quality life are apparent. However, these improvements did not fully materialize until a year post HCT.
Quality of Life by domainPhysical QoLParticipants reported a remarkable improvement in their physical QoL, one-year post-HCT.
Prior to undergoing HCT, all the patients experienced pain, fatigue, insomnia, and fevers, which participants termed “SCD crisis.” A parent explained her son’s experiences of physical pain prior to his HCT:
He had pain in his leg, and in his back…all the time, he had pain, pain, pain. And he can’t play.—Mother, Patient 3.
A patient revealed the frequency and severity of her pre-HCT pain:
…it was pretty bad. I would have crisis at least four times a year. Those are crises that I [would] need to go to the hospital for, and not ones that I could control with codeine and stuff at home. I just had a lot more pain.—Patient 2.
The SCD crises often led to hospitalizations. For some patients and their families, these hospital stays were frequent and stressful. A parent explained how her child’s recurrent pre-HCT crises placed their family in a cyclical movement between home and hospital:
As a parent, I saw how he was suffering. We went through a lot of struggle having sickle cell anemia. So it was very hard as a parent…We would have been staying two weeks in the hospital and one week at home—just like that, in and out of the hospital.—Mother, Patient 3.
The fragile nature of the patients’ physical health meant that their ability to perform physical tasks were constrained. Sports activities, such as swimming, and soccer were out of bounds to our participants, although they had the desire to participate.
…because I had sickle cell, there were things like swimming, for example, that I had to get taken out of…All of the time when I would swim in cold water, I would have a crisis.—Patient 2.
A year after the procedure, the experience of pain and fatigue had given way to a crisis-free life, and the patients had the capacity to take up sports.
…when I had sickle cell, I couldn’t play sports. So sometimes when I played sports I get tired quick. Sometimes I will feel pain. But after the transplant, it is okay. I can now play sports with my friends, like soccer, basketball. I don’t really feel that pain [and] all the tiredness [and] all the fatigue.—Patient 1.
All 5 patients physical QoL improved one-year post-transplant as per their interviews.
Social QoLThe pre-HCT social QoL of the patients and their families was poor, and typically characterized by stigma, social isolation, and parental absenteeism from work. All patients experienced stigma prior to undergoing HCT. A parent revealed how such perceptions caused her daughter to struggle with gaining acceptance and a sense of belonging in their extended family:
Back in Nigeria they just think that if you have sickle cell you don’t live long. Your life span is very short. So, people don’t even count them among the children, because they feel that maybe this child will die soon…my mother-in-law [said] F. is not a child. I shouldn’t count F. as a child because she has sickle cell.—Mother, Patient 2.
Another parent revealed how her son’s SCD status was stigmatized each time his illness was revealed to members of their community.
When I tell them oh he has sickle cell, they look at him differently, as if to say, “don’t go close to my daughter…I don’t want you liking my daughter for marriage.” And all that. And they look at him as if it is a disease that is transferrable.—Mother, Patient 1.
Pre-HCT social activities with peers were significantly curtailed by the SCD. All patients revealed how fatigue and the potential for a pain crisis caused them to refrain from activities, leaving them socially isolated and disconnected. Patient 4 revealed how the disease affected his social activities and interactions.
Like before I would go so tired before with my friends. I can’t hang out with them. I can’t play with them, anything, I can’t go with them. Sometimes at class I can’t go at lunch or play.—Patient 4.
The HCT process, the stay in hospital, and the need to isolate post-HCT at home (a period ranging from 3 to 6 months was necessary to avoid opportunistic infections) were equally isolating. Patients described this isolation as a difficult period.
I was bored every time. Because I was stuck inside [the hospital] mostly…because during that time, my immune system was low, so I was like very easily get infected.—Patient 3.
Academic studies were interrupted and described as negatively affecting social QoL.
I was missing school. I was kind of thinking like how I could catch up and like what the problem would be if I come late, because I know that I will have a pile of work coming to me…Because the school is like very serious. And they have a lot of things going on like, tests, quizzes.—Patient 5.
In one single parent family with multiple children, parental absence from home during pre-HCT periods of hospitalization affected the fulfilment of the emotional and material needs of the other children. A sibling explained how frequent pre-HCT hospitalizations affected their wellbeing:
It was hard for us, like you know, when we needed things at home. Mom wasn’t there because she would be with my sister in the hospital…For school I would need my mom to sign something, and then she wasn’t there to do that. Sister, Patient 2.
The absence of parents from work and its financial consequence during times of hospitalization constituted a source of socioeconomic disadvantage. A sibling of Patient 2 stated, “[Mom] had to take leave off work…My brother couldn’t always get the things he needed because my mom wasn’t getting pay.”
Although unintended, such parental absence can have negative consequences for social relationships within families, more so when parental absence is frequent, extensive, and sustained at the expense of the emotional development and material wellbeing of other family members.
Post-HCT, the adolescents gained social acceptance in their larger families and communities that once stigmatized and excluded them. One patient explained how the transplant has helped to mend her relationship with her extended family:
Some of my family members didn’t really accept me having sickle cell and stuff like that. And so like now that I don’t have sickle cell, some of those family members have tried to come in contact with me and talk to me now.—Patient 2.
A year after undergoing HCT, all patients experienced improvements in their social relations from all sources of data collected.
Psychological QoLThe pre-HCT life experiences of the patients were overshadowed by sadness, dissatisfaction with life, and psychological stress. The majority of patients commented that their future was bleak and may lead to premature death. Patient 1 revealed how his pre-HCT health conditions affected his thoughts:
I thought I would maybe die someday. That is something I would always think in my head. In Nigeria I always thought I was going to die, because I was always sick. So I thought the future was going to be very bad.
Negative thoughts and the pain experienced during SCD crises created despair, some patients had cried frequently at the thought of knowing that their illness was a lifetime condition. The feeling of sadness and despair often extended to the entire family. A parent explained how the pre-HCT experience created an atmosphere of sadness in the household:
I think that another challenge with the kids, you know, if one of them is not feeling well, so you see all of them look like they are sad. That affects also parents, when you see your kids sad, [and] they are not happy as you want them to be. So, it affects yourself too. Father, Patient 3.
Fear of the unknown was a constant part of the life of parents with children ailing from SCD. Parents felt a need physically be with the patient. The mother of patient 4 recollected that “his dad [was] always thinking [at work – what happens with my son?” The thought of having a permanently ailing child was a source of psychological burden to parents.
Although most patients and their families were relieved after learning about HCT, anticipation of HCT and the potential negative outcomes, including death and infertility, produced additional psychological stress. Information sessions provided included reference to the possibility of adverse outcomes and for some were a source fear and anxiety.
I did not know what to expect. I was dreaming even that E. died. Sometimes I would dream that he died during the program. So I was always afraid until that day. Mother, Patient 1
Patient 5 added, “I was kind of having second thoughts. Because I kind of thought that was a lot to handle.”
The patients and their families called for pre-transplantation information and counselling sessions that are encouraging and accurate.
A year after the transplant, the psychological stress diminished and for some families was eliminated. All 5 patients and their families expressed a feeling of relief, happiness, and hope for the future. The father of Patient 3 explained how HCT has brought happiness and a sense of psychological relief to his entire family:
When we started seeing the outcome…I can say our mind changed. We saw that our mind can be cooled down, compared to before the transplant…because there is no more crisis… He is doing sports.
Patient 4 added to this general sense of relief, “I am happy now. I don’t know how to say, but it is very good.” These narratives together convey a general sense that HCT has yielded positive psychological outcomes for both patients and their families (Table 3).
Table 3 Coding summary: changes in experiences and QoL
留言 (0)