
記住我







Introduction: People with tuberculosis experience long-term health effects beyond cure, including chronic respiratory diseases. We investigated whether tuberculosis is a risk factor for subsequent lung cancer.
Methods: We searched PubMed, Scopus, Cochrane, Latin American and Caribbean Health Sciences Literature and the Scientific Electronic Library Online for cohort and case–control studies providing effect estimates for the association between tuberculosis and subsequent lung cancer. We pooled estimates through random-effects meta-analysis. The study was registered in PROSPERO (CDR42020178362).
Results: Out of 6240 records, we included 29 cohort and 44 case–control studies. Pooled estimates adjusted for age and smoking (assessed quantitatively) were hazard ratio (HR) 1.51 (95% CI 1.30–1.76, I2=81%; five studies) and OR 1.74 (95% CI 1.42–2.13, I2=59%; 19 studies). The occurrence of lung cancer was increased for 2 years after tuberculosis diagnosis (HR 5.01, 95% CI 3.64–6.89; two studies), but decreased thereafter. Most studies were retrospective, had moderate to high risk of bias, and did not control for passive smoking, environmental exposure and socioeconomic status. Heterogeneity was high.
Conclusion: We document an association between tuberculosis and lung cancer occurrence, particularly in, but not limited to, the first 2 years after tuberculosis diagnosis. Some cancer cases may have been present at the time of tuberculosis diagnosis and therefore causality cannot be ascertained. Prospective studies controlling for key confounding factors are needed to identify which tuberculosis patients are at the highest risk, as well as cost-effective approaches to mitigate such risk.
AbstractAfter an episode of tuberculosis, an individual is more likely to be diagnosed with lung cancer than a person in the general population. This is most marked within the first 2 years after a tuberculosis diagnosis, but a causal relation cannot be ascertained. https://bit.ly/38I4HMc
IntroductionTuberculosis is a major health problem worldwide. Although the incidence is slowly declining, an estimated 10 million cases and 1.5 million tuberculosis deaths occurred in 2020 [1]. Its morbidity burden extends beyond cure, since people successfully treated for tuberculosis experience health problems in the long term. Tuberculosis has been associated with subsequent lung function impairment and other respiratory conditions such as bronchiectasis and COPD [2, 3]. All-cause mortality is significantly higher in people treated for tuberculosis compared to the general population [4].
The association between tuberculosis and lung cancer has received special interest. There were 2.2 million new cases and 1.8 million deaths from lung cancer in 2020 [5]. Chronic inflammation can promote tumour growth in different types of cancer and chronic inflammation in the lung has been hypothesised to promote carcinogenesis [6]. Chronic bronchitis and emphysema have been associated with increased risk of lung cancer, independently of tobacco use [7]. Inflammation from pulmonary tuberculosis has also been suspected to contribute to lung cancer development, but studies on the association between an episode of tuberculosis and subsequent lung cancer have shown mixed results. Some found a positive association, while others did not [8, 9].
A 2009 systematic review of epidemiological studies on the subject found a significant increased risk of lung cancer among people with previous tuberculosis, especially for adenocarcinoma [10]. However, most included studies had a case–control design. During the past decade, several cohort studies assessing this relationship have been published. Still, establishing a causal relationship between tuberculosis and lung cancer is challenging, as it is difficult to control for cofounding due to shared risk factors, especially smoking [11]. It is also problematic to ascertain the absence of lung cancer upon tuberculosis diagnosis, at the start of the follow up. Therefore, reverse causation needs to be considered, the more so because lung cancer facilitates activation of latent tuberculosis infection [12].
We appraised in a systematic review the now available evidence that evaluates the association between tuberculosis and subsequent lung cancer occurrence and mortality.
MethodsWe conducted a systematic review and meta-analysis. The population, exposure, comparator, outcome framework was filled out as follows. Population: any population; exposure: tuberculosis; comparator: subjects without tuberculosis; outcomes: lung cancer diagnosis (the main outcome) and lung cancer mortality (the secondary outcome). The protocol was prospectively registered in PROSPERO (ID number: CDR420178362). We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 checklist to report our findings (appendix 1).
Search strategy and selection criteriaWe searched the literature in PubMed, Scopus, Cochrane, Latin American and Caribbean Health Sciences Literature and the Scientific Electronic Library Online using terms related to “tuberculosis” and “lung cancer” (the full search strategy can be found in appendix 2). We manually searched the references cited in the papers included. Full-text peer-reviewed papers reporting on cohort and case–control studies written in English, French or Spanish and published between 1 January 1980 and 1 September 2021 were eligible for inclusion. We withheld studies with a comparator group reporting an effect estimate for the association between tuberculosis and lung cancer diagnosis or lung cancer mortality. Retrieved articles were uploaded to Covidence 2.0. Title and abstract screening as well as full-text reviews were performed in duplicate by two reviewers (J. Cabrera-Sanchez and V. Cuba). Discrepancies about the inclusion of a study were resolved by consensus or through discussion with a third reviewer (L. Otero).
Data extraction and risk-of-bias assessmentWe extracted data using a pilot-tested standardised form in Covidence. We extracted bibliographic information, study setting, population description, number of participants, methods to ascertain exposure (tuberculosis)/outcomes (lung cancer diagnosis and lung cancer mortality) and results, including number of events per exposure group and unadjusted and adjusted effect estimates of the association between tuberculosis and subsequent lung cancer diagnosis or mortality. We used the option “merge” in Covidence when data concerning the same study was reported in more than one paper, to treat multiple reports as one single study. In these cases, we extracted the effect estimate based on the larger study population. Authors were contacted by email when necessary to obtain relevant information.
To assess the risk of bias, we adapted the Newcastle–Ottawa scale for observational studies, maintaining three domains with a total of eight items: representativeness of the study population (four items), comparability of study groups (one item) and ascertainment of exposure (for cohorts), or outcome (for case–control studies) (three items). The full description of the adapted Newcastle–Ottawa scale, the rationale for adaptations and the rules used to reach the overall risk of bias judgment can be found in the supplementary material (appendices 3 and 4). Both the data extraction and the risk of bias assessment were accomplished independently by two reviewers and disagreements were solved with a third reviewer.
Statistical analysisWe performed a random-effects meta-analysis to pool unadjusted as well as adjusted estimates of the association between tuberculosis and subsequent lung cancer diagnosis or lung cancer mortality. We developed three models. In the first model, we pooled unadjusted estimates extracted from the included studies. In models two and three, we pooled adjusted estimates. Since the variables considered for adjustment varied widely between studies, we pre-defined (as proposed by Riley et al. [13]) a minimum set of variables for which studies had to adjust in order to be included in the latter models. These variables were age and smoking, for being associated with tuberculosis and constituting the strongest widespread risk factors for lung cancer. Smoking could be assessed either qualitatively by smoking status categories (never-, former or current smoker), or quantitatively, when measured by intensity, duration or cumulative amount. In the second model, we pooled studies’ estimates adjusted for at least age and any assessment of smoking. In the third model, we pooled estimates adjusted for at least age and any quantitative assessment of smoking. Estimates from studies restricted to never-smokers were considered to be quantitatively adjusted for smoking.
Thus, studies could contribute to more than one model depending on the estimates reported. If a study only reported results stratified by subgroups, we calculated a single pooled estimate. Studies that did not report unadjusted estimates nor estimates adjusted for at least age and smoking were not included in the meta-analyses, but are still part of the descriptive synthesis of the review, except when the data were available to calculate risk ratios or odds ratios for use in model 1. In view of their methodological differences, separate meta-analyses were performed for cohort and case–control studies. For cohort studies, risk ratios, incidence rate ratios and standardised ratios were pooled together with hazard ratios (HRs). We obtained estimates of pooled odds ratios for case–control studies.
To explore heterogeneity, we performed stratified meta-analyses. First, for all studies, stratified by overall risk of bias (as assessed by the review team) and then, conditional on data availability, by sex, smoking status and latency. Since effect estimates in never-smokers are free of residual confounding by active tobacco consumption, we did a subgroup analysis restricted to that subpopulation. We performed stratified analysis by time intervals between tuberculosis diagnosis and lung cancer detection (latency) aiming to decrease the possibility of lung cancer being present at time of tuberculosis diagnosis and deal with reverse causality bias. For this stratified analysis, we constructed categories accommodating the heterogeneity of the cut-offs reported.
We developed funnel plots and performed the Egger test to assess publication bias. Meta-analysis was done with the meta package version 4.16-2 using R Studio version 4.0.3. Effect measures were calculated with STATA 15.0 (Stata Corp, College Station, TX, USA) and OpenEpi (Centers for Disease Control and Prevention, Atlanta, GA, USA) when studies did not report them directly, but data to do so were available.
ResultsThe search yielded 6240 records, 5106 of which we screened after removing duplicates (figure 1). We excluded 4718 records and retained 127 for retrieving the full text. 62 reports fulfilled the inclusion criteria and were included. We identified 18 eligible records from citation searching. Hence, we included a total of 80 records and 73 unique studies. Lung cancer diagnosis was reported in 62 studies: 19 were cohort studies [8, 9, 14–30 ] and 43 were case–control studies [31–72]. Lung cancer mortality was reported in 13 studies: 12 were cohort studies [9, 26, 73–82] and one was a case–control study [83]. Two studies [9, 26] reported both outcomes. Appendix 5 indicates the number of studies included in the different meta-analysis models that pooled the estimates of associations of tuberculosis with subsequent lung cancer diagnosis or mortality. 46 studies originated from Asia, predominantly from China, Taiwan and South Korea (appendix 6); 16 came from North America (USA and Canada); 10 from Europe; and one from Africa. No studies were conducted in Oceania, Latin America or the Caribbean. Only 39 out of 62 and three out of 13 studies addressing diagnosis or mortality, respectively, adjusted somehow for smoking. 12, 25 and 25 studies had low, moderate and high risk of bias, respectively, for the main outcome. Four, one and eight studies were at low, moderate and high risk of bias, respectively, for the secondary outcome. A full description of the included studies and their risk of bias across different domains can be found in the supplementary material (appendices 7 and 8).
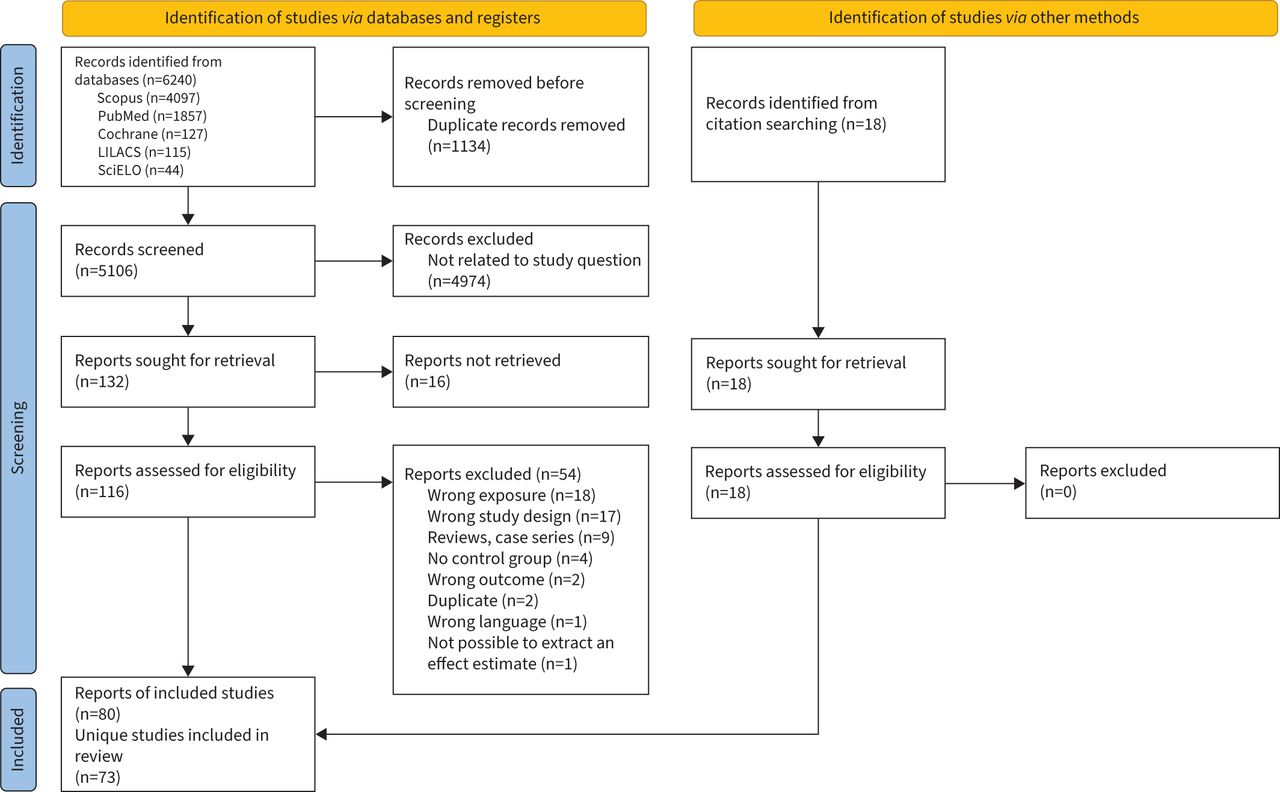 FIGURE 1
FIGURE 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flowchart. LILACS: Latin American and Caribbean Health Sciences Literature; SciELO: Scientific Electronic Library Online.
Sample sizes ranged from 6699 to 15 219 024 (median 29 641, interquartile range (IQR) 304 977) in cohort studies and from 144 to 91 301 (median 1212, IQR 1983) in case–control studies reporting the main outcome. Sample size in studies reporting the secondary outcome ranged from 515 to 1 607 710 (median 19 497, IQR 39 782) in cohort studies and was 1046 in one case–control study. For lung cancer diagnosis, the minimum length of follow-up in cohort studies was 3.8 years and the maximum was 18.5 years (median 8 years, IQR 4 years); for lung cancer mortality, the minimum was 2 years and the maximum 25 years (median 10 years, IQR 7 years). In most cohort studies, lung cancer was detected under routine medical care and coupled to tuberculosis diagnosis through record linkage or by using registries, except in one study [25], where chest radiography was performed systematically as part of the study's follow-up.
Individual results reported in the included studies are tabulated in appendix 9. Results from the meta-analysis are summarised in table 1. For lung cancer diagnosis, among cohort studies, the pooled adjusted hazard ratio for persons with a tuberculosis history versus nonexposed individuals was 1.87 (95% CI 1.29–2.70, I2=94%; figure 2) in model 2 and 1.57 (95% CI 1.20–2.07, I2=74%; figure 3) in model 3. There exists heterogeneity, but six out of seven studies that controlled for smoking documented a positive association. Among case–control studies, the pooled adjusted odds ratio was 1.76 (95% CI 1.41–2.19, I2=79%; figure 2) in model 2 and 1.74 (95% CI 1.42–2.13, I2=59%; figure 3) in model 3. Moderate heterogeneity was found, with 20 out of 23 studies included in model 2 documenting a positive association between tuberculosis and subsequent lung cancer diagnosis. The pooled model 2 estimate for lung cancer mortality subsequent to tuberculosis was significant in cohort studies (HR 1.62, 95% CI 1.18–2.21; I2=68%; appendix 10). The pooled estimates of the associations between tuberculosis and specific lung cancer subtypes (table 1) are generally in line with the overall results above, but lack precision.
TABLE 1Pooled estimates of the association between tuberculosis and subsequent lung cancer diagnosis or mortality
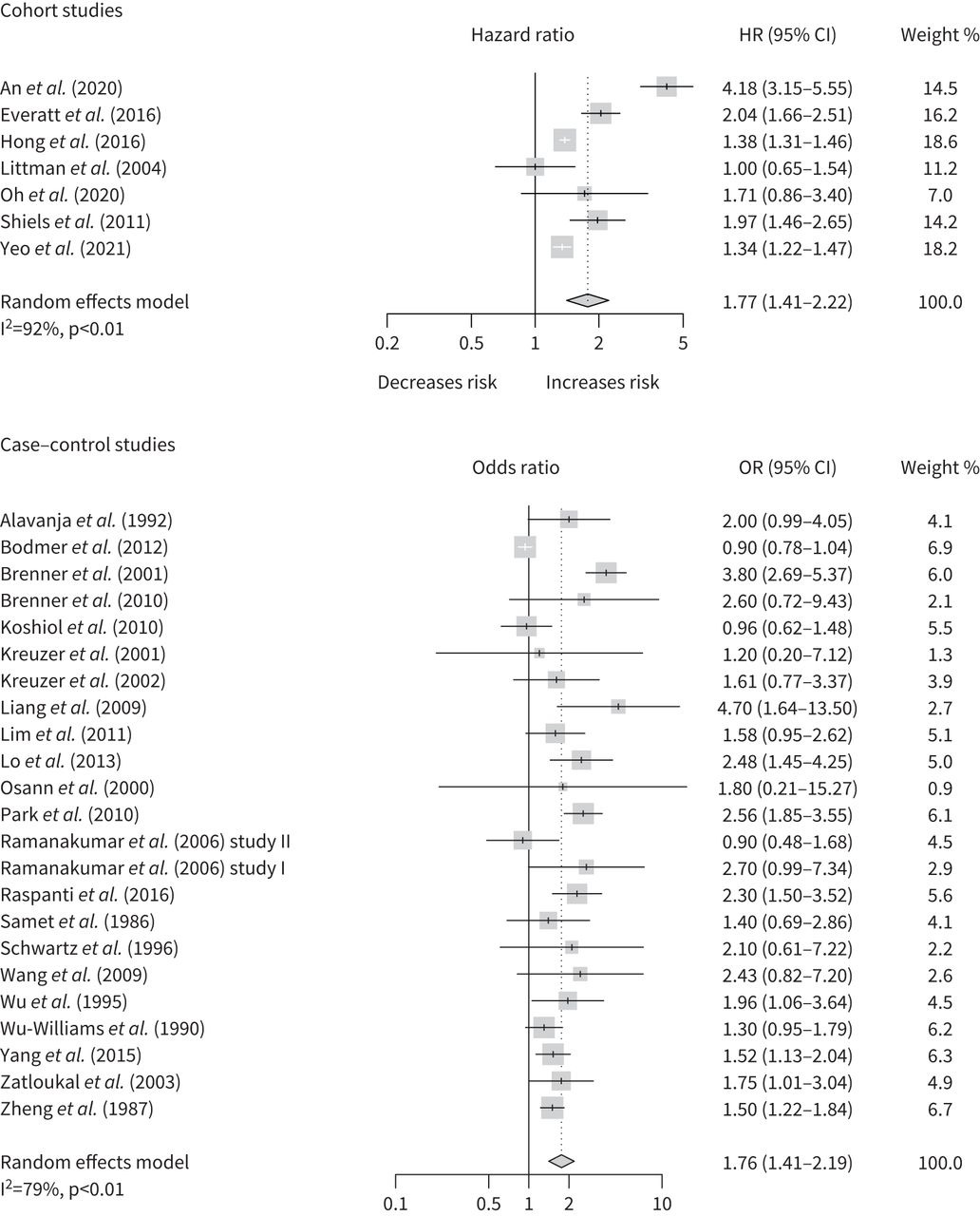 FIGURE 2
FIGURE 2 Forest plots showing the association between tuberculosis and subsequent lung cancer diagnosis in studies with adjustment for age and any assessment of smoking (model 2). HR: hazard ratio.
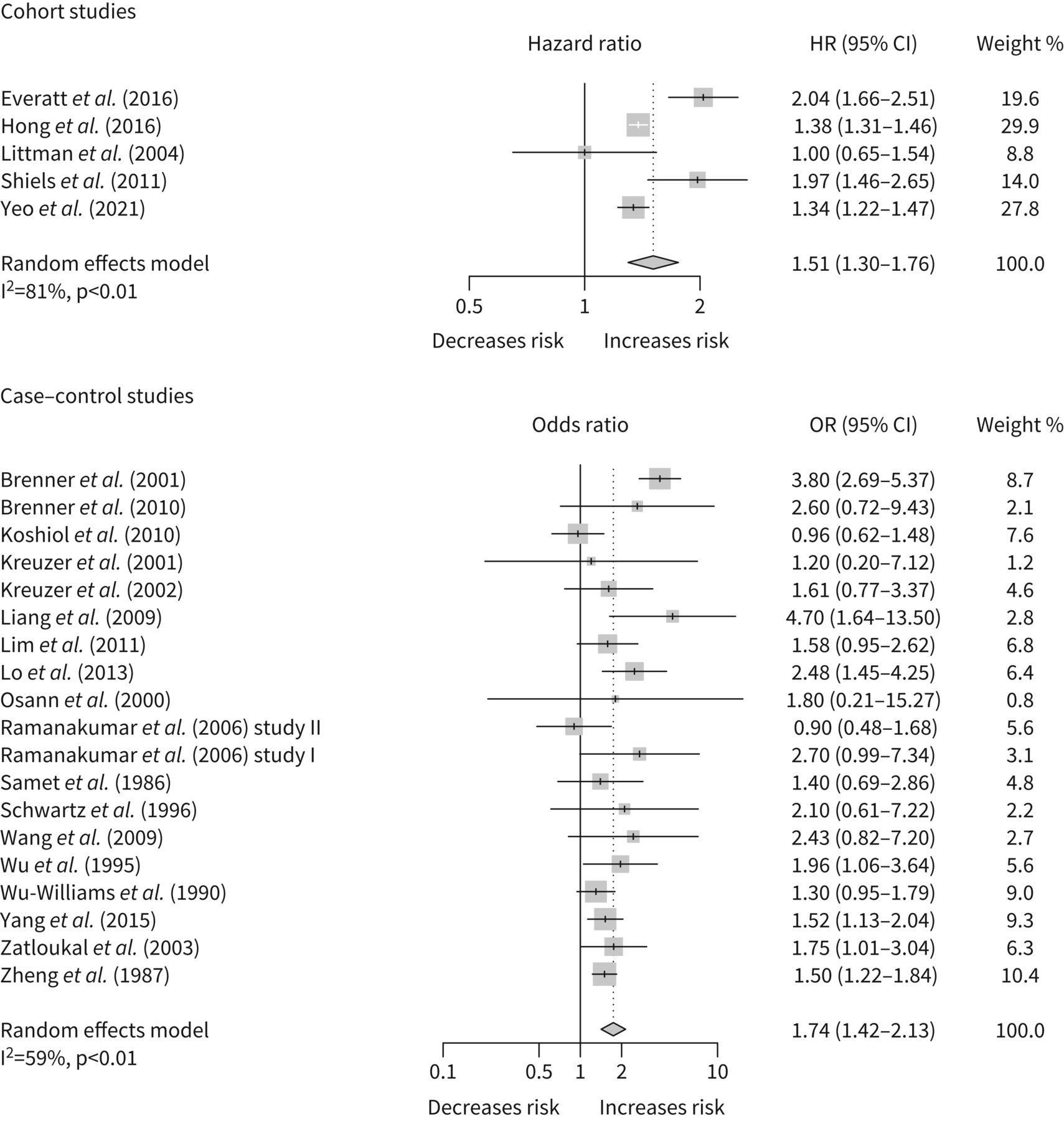 FIGURE 3
FIGURE 3 Forest plots showing the association between tuberculosis and subsequent lung cancer diagnosis in studies with adjustment for age and quantitatively assessed smoking (model 3). HR: hazard ratio.
We restricted stratified analyses (table 2) to the main outcome, lung cancer diagnosis, due to the small number of studies (n=2) eligible for inclusion in adjusted models of the secondary outcome. The estimates in the risk of bias strata differ between themselves, but still remain broadly in line with the nonstratified results reported earlier. Results by sex were comparable for men and women. The estimates in never-smokers were significant in both cohort and case–control studies and close to the earlier-obtained estimates in the models including studies that adjusted for smoking. We observed that the risk of lung cancer diagnosis was high in the first years after tuberculosis diagnosis (table 2 and appendix 11), but decreased and became moderate-to-weak over time.
TABLE 2Stratified pooled analysis of the association between tuberculosis and subsequent lung cancer diagnosis
Out of the 19 cohort studies reporting the main outcome, 10 did not perform stratified analysis according to the interval between tuberculosis diagnosis and detection of lung cancer nor exclude lung cancer cases detected in the first years of follow-up. Those that did so used variable cut-off points, which constrained our stratified pooled analysis by latency. The pooled hazard ratio adjusted for smoking and age for patients that developed cancer beyond 2 years of tuberculosis diagnosis from the only two studies reporting such effect estimate [17, 25] was 1.44 (95% CI 1.06–1.96; table 2). When we pooled study estimates that excluded lung cancer cases detected within 1 [15] or 2 years [17, 25] of tuberculosis diagnosis the pooled hazard ratio was 1.47 (95% CI 1.10–1.97) (appendix 12). Among the two cohort studies [18, 79] that reported adjusted results for the secondary outcome (lung cancer mortality), one [79] excluded patients who died within the first 2 years of follow-up alongside patients with unconfirmed suspected malignancy (or with recent weight loss) at enrolment. Its adjusted hazard ratio for tuberculosis and death from lung cancer was 2.01 (95% CI 1.40–2.89).
Funnel plots of the main outcome do not indicate small-study effects (appendix 13). Egger test was not significant for the main outcome in cohort (p=0.61) and case–control studies (p=0.37). These analyses were not performed for the secondary outcome due to the small number of included studies. The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) assessment of the evidence (appendix 14) reveals overall low certainty for cohort studies and very low certainty for case–control studies.
DiscussionThis systematic review and meta-analysis found moderate pooled effect estimates for being diagnosed with lung cancer after a tuberculosis episode: adjusted for age and smoking, a hazard ratio of 1.51 (95% CI 1.30–1.76) in cohort studies and an odds ratio of 1.74 (95% CI 1.42–2.13) in case–control studies. In addition, we found a compatible pooled hazard ratio of 1.62 (95% CI 1.18–2.21) of dying from lung cancer. The pooled hazard ratios and odds ratios for lung cancer occurrence remained consistent with the overall result in a stratified meta-analysis by risk of study bias and sex, and when restricted to never-smokers. The hazard ratio was positive for incidence of adenocarcinoma and squamous cell carcinoma diagnosis but not of small cell carcinoma. Importantly, in cohort studies we found, adjusted for age and smoking, a substantially increased occurrence of being diagnosed with lung cancer within the first 2 years after tuberculosis diagnosis (HR 5.01, 95% CI 3.64–6.89) that waned after year two (HR 1.44, 95% CI 1.06–1.96) and disappeared after 4 years.
Our crude results are comparable with the overall risk ratio adjusted for smoking (1.74, 95% CI 1.48–2.03) found in a previous review [10], which included 37 case–control and four cohort studies published between 1966 and 2008. However, that review concluded that, while declining much in the first 5 years, lung cancer risk ratio remained at ∼2 for >20 years after a diagnosis of tuberculosis. The overall certainty of evidence provided by the 43 case–control studies included in our review is very low, but most of the 19 cohort studies have moderate risk of bias, good precision and consistent effect estimates. However, the certainty of their accumulated evidence is rated low in the GRADE framework due to their observational nature. While almost all studies included in our review report effect estimates of the association between tuberculosis and subsequent lung cancer greater than one, there exists quite some heterogeneity that is possibly explained by the presence of (residual) confounding. It is of note that 31 out of the 73 studies did not even control for smoking status, while tobacco consumption increases the risk of developing lung cancer >10-fold [84]. However, when limiting our meta-analysis to the studies that controlled at least for smoking and age, or that selected never-smokers, we still found significant, moderately positive pooled hazard ratios and odds ratios.
The increased risk of lung cancer thus seems to be independent of active tobacco consumption, but we cannot exclude residual confounding by passive smoking, which has a weaker association to tuberculosis [85]. Furthermore, the studies did generally not adjust for socioeconomic status and environmental pollution, which have also been associated with tuberculosis and lung cancer [11]. Low socioeconomic status is a risk factor for tuberculosis [86] and may be associated with higher exposure to environmental pollution or occupational carcinogens. A meta-analysis found low socioeconomic status to mildly increase the risk of developing lung cancer after adjustment for smoking [87], and the authors hypothesised that both aforementioned exposures were overrepresented among people with lower socioeconomic status. Unfortunately, only two studies included in our review [26, 51] adjusted jointly for the three key confounders: age, smoking and socioeconomic status. Another limitation is that most studies did not conclusively rule out lung cancer upon tuberculosis diagnosis. Not surprisingly, since there are no effective screening methods to detect early or occult lung cancer, with chest radiographs lacking sensitivity and low-dose computed tomography being plagued by false positives [88]. Notwithstanding, the likelihood that occult cancer is present before the tuberculosis diagnoses can be high in retrospective designs and only two included studies were prospective. Furthermore, few studies reported estimates by latency to cancer diagnosis and among those that did, the time category cut-off points used were heterogeneous. This limited our scope for stratified meta-analysis by latency.
The substantially higher occurrence of lung cancer we uncovered in the first year (HR 8.50) and first 2 years (HR 5.0) following tuberculosis diagnosis, which fades out thereafter, raises the question whether cancer latency can be that short. The results could be explained by different mechanisms. Firstly, due to shared clinical and radiological characteristics lung cancer can initially be misdiagnosed as tuberculosis, as illustrated by a study in Taiwan [89] that found 1% of such misclassifications. Studies that include tuberculosis cases without bacteriological confirmation may be more prone to this error and most cohort studies in our review selected the exposed comparison group from large national databases or tuberculosis registries but do not clarify what percentage had bacteriological confirmation. Secondly, it is conceivable that occult cancer triggers active tuberculosis occurrence. A recent systematic review found that lung cancer patients are at nine-fold increased risk of developing active tuberculosis [12] and attributed most of the excess risk to the immunosuppressive cancer treatment. Still, people with undiagnosed lung cancer might be at increased risk of active tuberculosis due to cancer by itself having immunomodulatory effects. Excluding lung cancer cases diagnosed within the first 2 years of tuberculosis decreases, but not totally excludes the possibility of lung cancer prevalent cases being already present at the time of tuberculosis diagnosis. In our pooled analysis by latency (table 2), the adjusted hazard ratio for lung cancer diagnosis after ≥2 years of tuberculosis was 1.44 (95% CI 1.06–1.96). However, it was not significant at ≥7 years and ≥10 years. In the three cohort studies [15, 17, 25] that report adjusted stratified analysis according to latency for lung cancer diagnosis, the risk decreased as latency increases (appendix 11).
Thirdly, surveillance bias exists if tuberculosis patients are offered, or demand, more medical imaging after diagnosis and further lung conditions may be more likely to be diagnosed. However, regular chest radiography does not seem to increase the diagnostic yield when screening the general population [90]. In the prospective study by Shiels et al. [25] included in our review, a thorough medical examination with chest radiography was performed at baseline and all participants underwent regular repeat examinations and chest radiography at the same interval during 5–8 years’ follow-up [91]. The overall hazard ratio for lung cancer adjusted for age and smoking in this study was significant and decreased with time after tuberculosis diagnosis. Temporal ambiguity in retrospective designs coupled to the scarcity of prospective studies demonstrating a decreasing relative risk over time has been interpreted as absence of genuine relationship between tuberculosis and lung cancer [18]. However, a credible alternative hypothesis would be that the risk dwindles after tuberculosis is cured, analogous to lung cancer hazard progressively decreasing after smoking cessation.
We document a modestly increased risk of developing lung cancer after a tuberculosis episode and observe consistency: hazard ratio and odds ratio between 1.5 and 2 in our overall and stratified analyses. Methodological limitations of the reviewed studies warrant a plea for cautious interpretation and preclude a causal reading, but tuberculosis being a risk factor for lung cancer is plausible and coherent. Chronic inflammation in the lung promotes carcinogenesis, in which macrophages may play a role by producing inflammatory cytokines and nitrogen reactive species [92]. This is illustrated by the carcinogenesis in mycobacterium-infected rats depending on the activity of macrophages [93]. Chronic inflammation may also damage DNA and increase mutation rates in key genes that promote malignant cell proliferation and angiogenesis. A study in South Korean patients with pulmonary adenocarcinoma found that the presence of pre-existing tuberculosis lesions was associated with significantly more epidermal growth factor receptor gene mutations [94]. The fragile histidine triad diadenoside triphosphate gene, a tumour suppressor gene, has also been found to be more frequently affected in lung cancer patients with a tuberculosis infection [95].
Evidence is growing on the long-term health consequences of having tuberculosis [96]. This review suggests a potential higher risk of developing lung cancer, which tuberculosis program managers and clinicians ought to be aware of. However, the finding of increased occurrence of lung cancer in the first 2 years after tuberculosis diagnosis could also indicate that some lung cancer cases may have been present at the time of tuberculosis diagnosis, and therefore it is not possible to ascertain causality. Yet, no concrete hard recommendations can be made relating to the programme's organisation for routine post-cure follow-up, screening and early detection. Notwithstanding, in particular in patients with other risk factors for lung cancer, our result prompt sharpening up clinical suspicion during fortuitous re-encounters and reinforcing the possible ensuing diagnostic work-up.
Questions for future researchFurther basic research is recommended to better understand the biological mechanisms behind the tuberculosis-subsequent lung cancer association. Linking routine tuberculosis programme databases and cancer registers in countries with reliable health information systems, as well as setting up methodologically rigorous longitudinal clinical–epidemiological studies that permit adequate control of potential confounding factors, could enable the identification of which tuberculosis patients (if any) are at the highest risk and for how long. Eventually, operational research will be needed to sort out how health services can cost-effectively contribute to mitigating that risk.
Supplementary materialSupplementary MaterialPlease note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0025-2022.SUPPLEMENT
FootnotesProvenance: Submitted article, peer reviewed.
Author contributors: J. Cabrera-Sanchez, V. Cuba and L. Otero conceived the study idea. J. Cabrera-Sanchez, V. Cuba, P. Van der Stuyft and L. Otero designed the protocol. J. Cabrera-Sanchez and V. Cuba did the literature search, extracted data and assessed the risk of bias. J. Cabrera-Sanchez and V. Cuba performed the statistical analysis with support from V. Vega and P. Van der Stuyft. J. Cabrera-Sanchez wrote the initial draft of the manuscript. All authors critically revised, provided important conceptual input, and approved the final version of the manuscript. All authors had access to the data.
Data sharing: The data supporting this meta-analysis are from previously reported studies and datasets, which have been cited. The extracted data are available in the supplementary material.
Conflict of interest: The authors have nothing to disclose.
Support statement: The study received financial support from the Institutional Collaboration Framework Agreement lV between the Institute of Tropical Medicine Antwerp, Belgium and Instituto de Medicina Tropical Alexander von Humboldt, Universidad Peruana Cayetano Heredia, Peru. L. Otero is supported by an Emerging Global Leader Award from the Fogarty International Center at the National Institutes of Health (K43TW011137). Role of the funding source: The funding source had no role in the design, interpretation, or decision to submit this manuscript. Funding information for this article has been deposited with the Crossref Funder Registry.
Received February 4, 2022.Accepted May 16, 2022.Copyright ©The authors 2022http://creativecommons.org/licenses/by-nc/4.0/This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissionsersnet.org
留言 (0)