
記住我
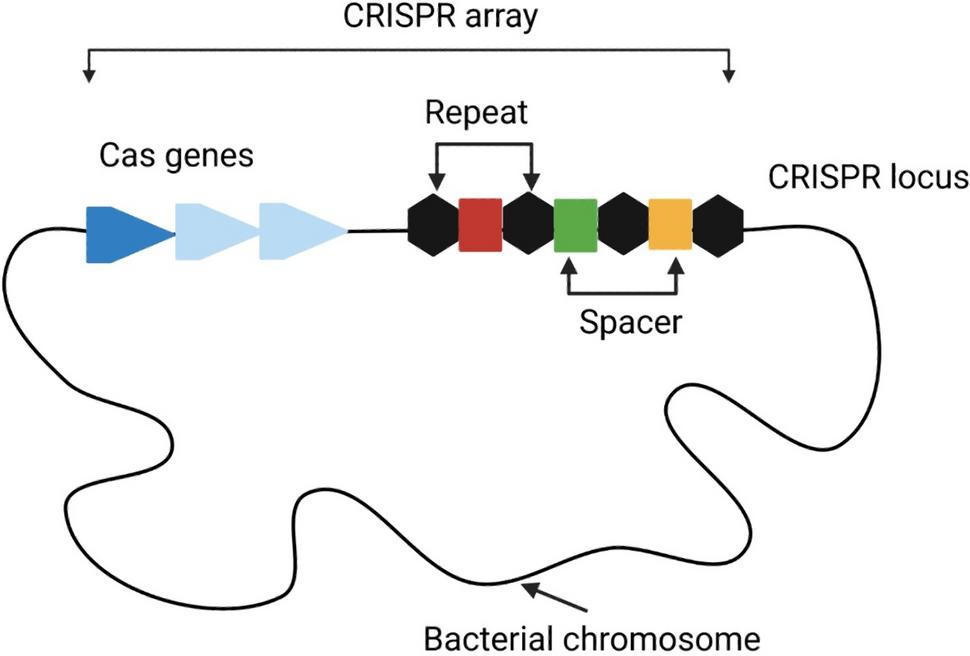
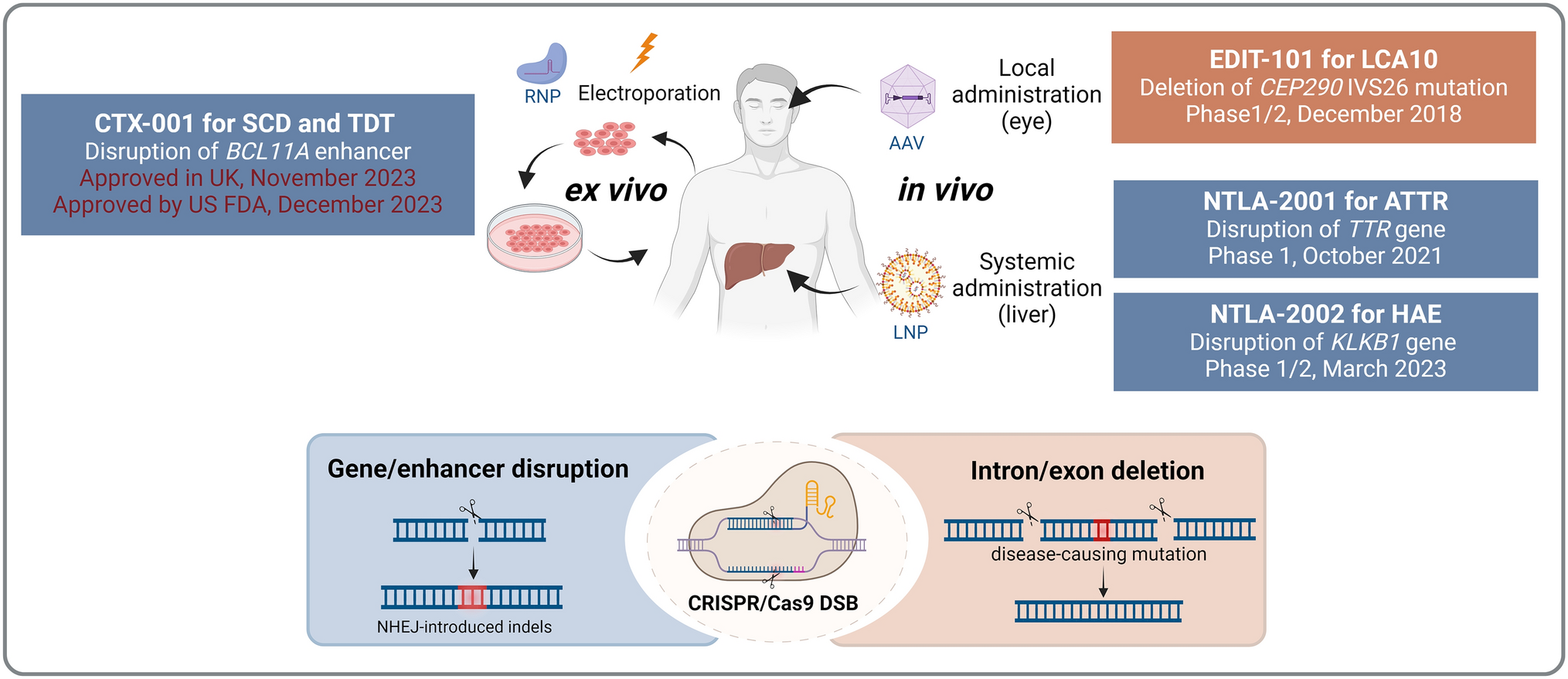


A systematic search yielded 982 citations. After eliminating duplicates, 626 citations remained for the initial title/abstract screening phase (Fig. 1). Following an initial screening, 240 records were chosen, and a more thorough examination yielded 35 citations. After assessing the selected citations, one expert (HC) (1) excluded 18 citations because, even though the prespecified terms were mentioned in the citations, they reported reference biologic-to-biosimilar transitions, and not biosimilar-to-biosimilar switches; (2) recommended exclusion of an abstract because it was subsequently published as a full article in a peer-reviewed journal; (3) recommended inclusion of six additional peer-reviewed publications based on his knowledge of the literature; and (4) recommended inclusion of three abstracts. The primary reason for inclusion of new citations that were not identified during the screening process was that the data provided within the citation described a biosimilar-to-biosimilar switching event, even though the pre-specified terms were not included within the text of the citation. Two other experts (SH and WB) reviewed and agreed with the recommendations of the first reviewer, except for the recommended deletion of one abstract, because the abstract contained some information that was not included in the subsequent peer-reviewed publication of the same study.
Fig. 1
Flow chart illustrating literature search outcomes
All citations chosen for inclusion were from published observational studies. Because of considerable inter-study variability of patient demographics, baseline characteristics, dosage regimens, and follow-up durations, it was not possible to conduct a meta-analysis. It was often difficult to perform and interpret a meaningful comparison of individual published observational biosimilar-to-biosimilar switch studies, especially when they evaluated different molecules. Because biosimilar-to-biosimilar switching is a relatively novel concept, all articles included in this study are from 2019 or later. The majority of studies investigated switches between one biosimilar infliximab (CT-P13) to another biosimilar infliximab (SB2). Other biosimilar-to-biosimilar switch scenarios discussed include adalimumab biosimilars (ABP 501 and SB5), etanercept biosimilars (SB4 and GP2015), and rituximab biosimilars (CT-P10 and GP2013). Of the 23 studies, 13 were published as full articles in peer-reviewed journals, the remainder were published as conference abstracts. A total of 3657 patients were included in these studies (Table 1). The studies were heterogeneous in size, design, and endpoints, providing data on safety, effectiveness, immunogenicity, pharmacokinetics, patient retention, patient and physician perceptions, and drug-use patterns (Fig. 2). An evidence table (see the Electronic Supplementary Material, supplemental Table S1) was developed based on the data synthesis and analysis that provides indications studied, number of patients, study design including endpoints, follow-up period, a summary of clinical outcomes, and the conclusions of the authors.
Table 1 Overview of biosimilar-to-biosimilar studiesFig. 2
Overview of type of information available from biosimilar-to-biosimilar studies. HCP healthcare professional, PK pharmacokinetics
Biosimilar-to-Biosimilar Switch Studies of Infliximab Biosimilars (CT-P13 to SB2 and CT-P13 to GP1111)Several studies evaluated patients who had switched from CT-P13 to SB2, from CT-P13 to GP1111, or from infliximab reference biologic to CT-P13 and subsequently to SB2. Infliximab biosimilar-to-biosimilar switch studies were most often conducted in the inflammatory bowel disease (IBD) indication; additional indications studied included psoriasis (PsO) and other immune-mediated inflammatory disorders.
Studies in Patients with Inflammatory Bowel DiseaseIn patients who switched from CT-P13 to SB2, Trystram et al. reported a drug persistence (SB2 discontinuation-free survival) of 94.9% after 54 weeks [26]. In total, 17 patients (10.8%) experienced a loss of response to SB2, including ten who had been managed through dose-optimization and continued treatment. In infliximab-treated patients with IBD, up to 20% of them lose their response to the drug every year after the primary response [27, 28]. No changes were observed in clinical activity scores, fatigue, biologic activity, or pharmacokinetic parameters after the single- or double-switch. Overall, the authors concluded that after 54 weeks of follow-up, switching from infliximab reference biologic to CT-P13 and subsequently to SB2 did not affect efficacy, immunogenicity, or safety of anti-tumor necrosis factor (anti-TNF) treatment. Additionally, the authors found no link between multiple switching and patient views regarding the need for (and concerns about) biosimilars [26].
In addition, studies with comparable follow-up periods (~12 months) [26, 29,30,31] found no loss in clinical responses at the middle [26, 30, 31] or conclusion of the studies [26, 29,30,31]. Mazza et al. [31] found that the loss of response rate was ~15% at the conclusion of the trial, with no statistically significant differences between patients who switched from infliximab reference biologic to CT-P13 (n = 66) and those who switched from infliximab reference biologic to CT-P13 then to SB2 (n = 52); the observed loss of response was consistent with response loss with any infliximab treatment in patients with IBD [27, 28]. The double-switch group from infliximab reference biologic to CT-P13 to SB2 had no statistically significant changes in AEs compared with the single biosimilar-to-biosimilar switch group [31]. Additionally, in 186 patients who switched from CT-P13 to SB2 (of whom 99 had previously switched from infliximab reference biologic to CT-P13 to SB2), no adverse impact was observed on infliximab trough levels and clinical and biochemical disease activity, regardless of whether switching for the first or second time [30]. De novo antidrug antibodies (ADAs) were found in < 4% of patients in either the single- or double-switch group [32].
The French prospective/retrospective non-interventional cohort PERFUSE study analyzed data of patients (n = 1374) receiving the SB2 biosimilar for a period of 12 months [33]. Findings from the study suggested that patients with IBD can be successfully transitioned from reference or biosimilar infliximab to SB2 with no loss of disease control or safety concerns, and over 92% of patients who transitioned from reference infliximab or another biosimilar infliximab continued SB2 treatment at 12 months post-initiation [33]. A study with a follow-up period of < 1 year (6 months) showed similar clinical remission rates (58.3%) and normal C-reactive protein (CRP) values (94.4% and 91.7% of patients) prior to 6 months and after 3 months of treatment in 36 patients who switched from CT-P13 to SB2 (12 of them switched from reference infliximab to CT-P13 to SB2) [34]. Furthermore, in another study with a follow-up period of < 1 year (8 months, safety events in single-switch (n = 43; CT-P13 to SB2) and double-switch (n = 24, infliximab reference biologic to CT-P13 to SB2) groups did not differ from those of the reference-to-biologic switch group [35]. Similarly, a single-center study in the Edinburgh IBD unit examined IBD patients (n = 246) who were switched from CT-P13 to GP1111 (57/246, double-switch) [36]. No significant differences were observed between the Harvey-Bradshaw Index, Mayo Score, CRP, fecal calprotectin, and trough infliximab levels comparing before and 6 months after GP1111 switch in either CT-P13 to GP1111 (single biosimilar-to-biosimilar switch) or infliximab reference to CT-P13 to GP1111 groups (double switch) [36].
A study in a large teaching hospital reported findings from patients (n = 227) with IBD who switched from CT-P13 to SB2 using the same standard of care [37]. Overall, the switch was well received, patients were satisfied with the process, and 99.2% of patients did not report any AEs. Of minor note, two reports of AEs were attributable to changes in the rate of drug administration [37].
Findings from a study that measured outcomes of transitioning a cohort (n = 133) of IBD patients from CT-P13 to SB2 in a real-world setting showed that there was no detrimental effect on patient outcomes as assessed by disease activity scores, patient-reported outcome (PRO) measures, and drug persistence for at least 4 months [38].
A multicenter real-life IBD cohort study reported findings from switching between infliximab biosimilars in two IBD centers in the UK [39]. A total of 289 patients with IBD switched from biosimilar CT-P13 to GP1111. Outcomes reported included patient acceptability, infusion reactions, and quantity of ‘best value’ (brand with the lowest acquisition cost) infliximab administered over a 6-month period. The study concluded that switching between infliximab biosimilars was acceptable to patients and was associated with a low rate of infusion reactions. The proportion of patients who discontinued treatment due to loss of response over a 6-month period was consistent with the published loss-of-response rates [39].
Studies in Other IndicationsGisondi et al. reported the effectiveness and safety of switching from CT-P13 to SB2 in patients (n = 96) with chronic plaque PsO who had been regularly followed in an outpatient PsO clinic in Italy [40]. Findings showed stable PsO severity, as determined by Psoriasis Area and Severity Index (PASI), during 6 months of observation. Treatment was withdrawn in ten of 96 patients (10%) because of loss of response (n = 7) or acute infusion reactions (n = 3). The authors highlighted the reduction in healthcare costs with biosimilars and the need for controlled studies to build robust evidence to support biosimilar-to-biosimilar switching [40].
In a 3-year observational study, Lauret et al. assessed whether successive switches from innovator infliximab to an infliximab biosimilar (CT-P13), followed by a switch to a second infliximab biosimilar (SB2), increased the risk of immunogenicity in patients (n = 140) with chronic inflammatory diseases [41]. The study demonstrated that immunogenicity was low (3 per 100 patient-years), and that immunogenicity levels did not increase after the switch to infliximab biosimilars in treatment of chronic inflammatory diseases [41].
Fautrel et al. presented data of 496 rheumatic patients (ankylosing spondylitis [AxSpA], RA, and psoriatic arthritis [PsA]) receiving the SB2 infliximab biosimilar from the aforementioned French non-interventional PERFUSE study [42]. This 12-month analysis indicated that patients with AxSpA, RA, or PsA can be successfully treated with SB2 as initial infliximab therapy or transitioned from the reference biologic or another infliximab biosimilar without loss of disease control and without a dose penalty. At least 75% of patients who transitioned from a prior infliximab remained on SB2 at 12 months after initiation of treatment with SB2 [42].
A study analyzed biosimilar switching patterns in US Veterans Affairs (VA) patients using a real‐time infliximab safety dashboard comprising prescription, diagnosis, and switching-pattern data [43]. Overall, 607 patients switched from one biosimilar to another. A total of 138 patients had one or more adverse drug event; 22 had one or more hospitalization. The authors concluded that biosimilar-to-biosimilar switches did not lead to increased AEs or hospitalizations [43].
An observational cohort study analyzed a nationwide switch from originator infliximab to biosimilar CT-P13, and subsequently to biosimilar GP1111, in real-world patients with inflammatory arthritis followed in the Danish DANBIO registry [44]. Patients with RA, PsA, or AxSpA were studied. In 2015, a total of 780 patients completed the first switch; patients were treated with reference biologic for a median of 7 years. At 1 year, 83% maintained CT-P13 treatment. In 2019, 52% of CT-P13-treated patients were still on treatment and performed a second, biosimilar-to-biosimilar switch to GP1111. At 1 year after the biosimilar-to-biosimilar switch, 91% maintained GP1111 treatment. For both rounds of switching, withdrawals were associated with worse baseline PROs, worse health assessment questionnaire scores, and less frequent patient acceptable symptom state (PASS), whereas objective markers (CRP, physician global assessment) were similar [44].
Biosimilar-to-Biosimilar Switch Studies of Adalimumab Biosimilars (ABP 501 and SB5)Ribaldone and colleagues enrolled 61 patients with Crohn's disease who had switched from the adalimumab biosimilar ABP 501 to adalimumab biosimilar SB5, of whom 43 (70.5%) were initially treated with the reference biologic (a multiple switch from adalimumab reference to ABP 501 then SB5) [45]. After 6 months, 88.5% (54/61) of patients remained on SB5. The switch was successful in 82.0% (50/61) of patients (no systemic corticosteroids for 6 months, no cessation of SB5, no dosage increase). Seven patients (11.5%) had AEs compared with one (1.6%) in the 6 months before the switch (P = 0.03). The increase in AEs was notable. Nonetheless, the authors concluded that switching between adalimumab biosimilars was not associated with new safety or effectiveness concerns beyond those previously documented for adalimumab [45].
An observational cohort study in a tertiary IBD referral center examined patients (n = 35) with IBD who underwent a double-switch from the adalimumab reference biologic to adalimumab SB5 and subsequently to adalimumab biosimilar ABP 501. Patients were treated for a median of 30 months [interquartile range (IQR) 18–50] with the reference biologic. After a median of 28 weeks [IQR 15–43], patients were either switched from SB5 to ABP 501 (n = 31) or back to the reference biologic (n = 4). During ABP 501 treatment, no patients developed new detectable antibodies. None of the 35 patients who switched from SB5 to ABP 501 discontinued ADAs; trough levels remained stable over time [46].
The PERCEPTION study investigated outcomes of mono- and multi-switching scenarios in real-world settings in terms of patient attitudes towards switching from one adalimumab biosimilar to another [47]. Patients (n = 90) with chronic inflammatory rheumatic diseases, including RA, AxSpA, and PsA, were categorized into either mono-switch (reference biologic to biosimilar; n = 42) or multi-switch (reference biologic to first biosimilar and a second; n = 48) groups. The study showed that multi-switching did not result in decreased patient satisfaction in patients receiving biosimilar therapy. The number of switches, in particular, had no effect on patient satisfaction [47].
Biosimilar-to-Biosimilar Switch Studies of Etanercept Biosimilars (SB4 and GP2015)Two studies were included in the current systematic review that investigated switching between etanercept biosimilars with a follow-up of 12 months [48] and 21.1 months, respectively [49]. In the study with the 12-month follow-up [48], patients (n = 76) with PsO switched from reference etanercept to etanercept biosimilar SB4 and subsequently to biosimilar etanercept GP2015. In terms of efficacy, median PASI was 1 (0–2) after 3 months and 0.5 (0–1) after 12 months of therapy. Two patients experienced psoriatic flares during the study. No treatment-emergent serious AEs were reported. Efficacy and safety were maintained after switching between etanercept biosimilars [48]. Kiltz et al. studied 100 patients (54 RA, 27 AxSpA, 19 PsA) who had switched etanercept biosimilar SB4 to etanercept biosimilar GP2015 with a mean follow-up of 21.1 ± 7.4 months [49]. The authors concluded that after multiple switches from the original etanercept to SB4 and then to GP2015, the retention rate was close to 90% 6 months after the final switch [49]. No changes in disease activity or function were found in any indication.
Biosimilar-to-Biosimilar Switch Study of Rituximab Biosimilars (CT-P10 and GP2013)Urru and colleagues assessed the safety of switching between rituximab biosimilars (CT-P10 and GP2013) in a prospective observational study in patients with non-Hodgkin’s lymphoma (NHL) and chronic lymphocytic leukemia (CLL) [50]. Overall, 83 (NHL, n = 72; CLL, n = 11) patients were included in the study; 60% experienced one or more switch (reference biologic to biosimilar or biosimilar to biosimilar); 32% were switched from one biosimilar to another; the median follow-up was 10.5 months. Disease activity was assessed after the third cycle and at the end-of-treatment period; 93.1% (67 of 72) and 36.4% (4 of 11) of patients with NHL and CLL, respectively, achieved complete or partial responses. AEs were reported in 71 patients (85.5%) and were similar in patients who had received one or two biosimilar formulations (32/33 in the no-switch group vs 25/26 with one of the switches during the study period, P = 0.86). Findings from this publication support the position that switching between rituximab biosimilars is safe and does not lead to loss of efficacy. No safety signals emerged in association with the use of a specific biosimilar or with the practice of switching [50].
留言 (0)