
記住我
Colorectal cancer is the fourth most common type of cancer in the United States with ~150,000 new cases in 2020.1 Because of the risk of pelvic recurrences, preoperative chemoradiation is an established standard of care for patients with locally advanced rectal cancer and has been shown to downstage tumors and improve rates of pathologic complete response and R0 resection, local control, and survival.2–7 In contrast, because of the lower risk of local recurrence for colon cancer and potential toxicities with radiation given the close proximity of the small bowel, radiotherapy is not routinely used as part of curative treatment, which consists mainly of surgical resection followed by adjuvant chemotherapy depending on stage.8
Approximately 10% of colorectal cancers are located at the rectosigmoid junction, and it is unclear whether to treat these cancers like a rectal cancer, with neoadjuvant radiotherapy, or like a colon cancer, with upfront surgery and possible adjuvant therapy. Inappropriately omitting neoadjuvant radiotherapy may lead to higher rates of local-regional recurrence, but at the same time, delivering unnecessary neoadjuvant therapy may subject patients to excess treatment-related toxicities.
Various definitions based on location have been used to try to guide management of rectosigmoid cancers including distance from anal verge (AV)2,4–7,9–11 and relationship to anatomic landmarks such as the sacral promontory and peritoneal reflection (PR).12–14 We aimed to determine the optimal treatment approach for locally advanced rectosigmoid cancers and to determine whether these various anatomic definitions can guide therapy.
MATERIALS AND METHODS Patient Cohort and VariablesIn this institutional review board-approved retrospective study, we identified patients with rectosigmoid cancers treated at our single academic center between 2006 and 2018. Patients were included if they had staging magnetic resonance imaging (MRI) or computed tomography (CT) of the pelvis and had nonmetastatic, clinical stage T3/T4, and/or N+ disease. The primary tumor had to be located between 9 and 20 cm from the AV either on imaging, colonoscopy, or sigmoidoscopy. We included patients who had definitive surgery (abdominoperineal resection, total or partial colectomy, or low anterior resection), with neoadjuvant or adjuvant therapy, and who underwent chemotherapy.
We collected available data from the medical chart on patient demographics, tumor characteristics, and treatment details. We classified the primary tumor location using distance from the AV as well as relationship to the PR and sacral promontory. If any part of the tumor was straddling the PR or sacral promontory, it was characterized as “straddle”. For tumors characterized as “above” or “below” the anatomic landmarks, the entire length of the tumor had to be above or below the PR or sacral promontory. The sacral promontory was defined as a plane drawn from the promontory to the pubic symphysis.15 The peritoneum was identified in the midsagittal plane as a thin, hypointense line along with the superior bladder in men or the uterus in women that extends inferiorly and posteriorly to approximately the tip of the seminal vesicles in men and the cul-de-sac in women, after which the posterior extension attaches to the rectal wall anteriorly.16 Board certified radiologists with an expertise in gastrointestinal malignancies reviewed the staging imaging for positive or close circumferential margins. High specificity of up to 92% for prediction of margins by MRI by radiologists with experience in gastrointestinal and MRI have been previously described in a prospective observational study.17
Margins were described as close or threatened if the tumor was <2 mm from the mesorectal fascia. We classified treatment into (1) neoadjuvant therapy followed by surgery±adjuvant therapy, and (2) upfront surgery with adjuvant therapy. The decision for different treatment approaches was made on a case-by-case basis and discussed at a multidisciplinary lower gastrointestinal tumor board.
Outcomes and Statistical AnalysisTime to overall survival (OS), was defined as the time from the start of any treatment to the date of death; patients who did not die were censored at the date of last clinical follow-up. Time to OS was summarized using Kaplan-Meier and groups were compared using log-rank tests. Time to locoregional failure (LRF), and time to distant metastasis were defined as the time from the start of any treatment until date of locoregional or distant failure, respectively, with death as a competing event. LRF was defined as recurrence in the region surrounding the tumor bed, anastomosis site, anterior pelvic organs, perineum, or pelvic nodal stations. These time to event outcomes were analyzed using competing risk methods and groups were compared using Gray test. Continuous variables and categorical variables were compared using Mann-Whitney U test, and Fisher exact test, respectively. All tests performed were 2-sided with an α level of 0.05. All analyses were performed in SAS (SAS Institute Inc., Cary, NC).
RESULTS Patient, Tumor, and Treatment CharacteristicsA total of 161 patients were identified and included in the analyses. Ninety-nine patients had staging MRI, and 62 patients had staging CT imaging. 149 patients had tumors that were 9 to 20 cm from the AV on imaging, and 148 patients had tumors that were 9 to 20 cm from the AV on colonoscopy or sigmoidoscopy. Of the entire cohort, 97 patients had neoadjuvant therapy and 64 patients had upfront surgery. In the neoadjuvant group, 11 (11.3%) patients received short-course radiation, and 86 (88.7%) patients received long-course radiation. One patient (1%) did not complete radiation therapy and stopped after 8 fractions. Six (6.2%) patients received total neoadjuvant therapy (2 with short-course radiation and 4 with long-course radiation). In the upfront surgery group, 4 (6.3%) patients received adjuvant radiation therapy.
Patients who had neoadjuvant therapy were significantly younger (53 vs. 58.3 y, P=0.03), had primary tumors that were closer to the AV on colonoscopy (10.0 vs. 15.0 cm, P<0.01), closer to the AV on imaging (10.5 vs. 13.5 cm, P<0.01), and more likely below the PR (74.2% vs. 60.9%, P<0.01). Patients in the neoadjuvant group also had higher clinical T stage tumors (Table 2) and more tumors that had a positive or close circumferential resection margin seen on imaging (28.9% vs. 1.6%, P=0.015). Patients in the adjuvant group had more cycles of adjuvant chemotherapy (median 6 vs. 8 cycles, P<0.01, Table 1) and higher pathologic T stage and N stage, likely due to the lack of downstaging effect from neoadjuvant therapy (Table 2). A combination of capecitabine and oxaliplatin was the most used chemotherapy regimen, followed by a combination of leucovorin, 5-FU, and oxaliplatin.
TABLE 1 - Patient and Treatment Characteristics Neoadjuvant Treatment (n=97) n (%) Adjuvant Treatment (n=64) n (%) P Age (years, median) 53.0 58.5 0.03 Sex 0.73 Female 54 (55.7) 38 (59.4) Male 43 (44.3) 26 (40.6) Smoking status 0.55 Current 5 (5.2) 2 (3.1) Former 26 (26.8) 22 (34.4) Never 66 (68) 40 (62.5) ECOG 0.12 0 36 (37.1) 24 (37.5) 1 50 (51.5) 17 (26.6) 2 2 (2.1) 2 (3.1) Unknown 9 (9.3) 21 (32.8) Ethnicity 0.19 White 52 (53.6) 25 (39.1) Hispanic 14 (14.4) 11 (17.1) Other 31 (32) 28 (43.8) Adjuvant chemotherapy (number of cycles, median) 6 8 <0.01 Neoadjuvant short-course radiation 11 (11.3) — Neoadjuvant long-course radiation 86 (88.7) — TNT 6 (6.2) — Postoperative radiation 0 (0) 4 (6.3)ECOG indicates Eastern Cooperative Oncology Group; TNT total neoadjuvant therapy.
Sex, smoking status, Eastern Cooperative Oncology Group score, and ethnicity were not significantly different between the 2 groups (Table 1). There were no significant differences between the 2 groups in the primary tumor’s relationship to the sacral promontory, and the number of tumors with a positive circumferential resection margin on the surgical specimen (Table 2).
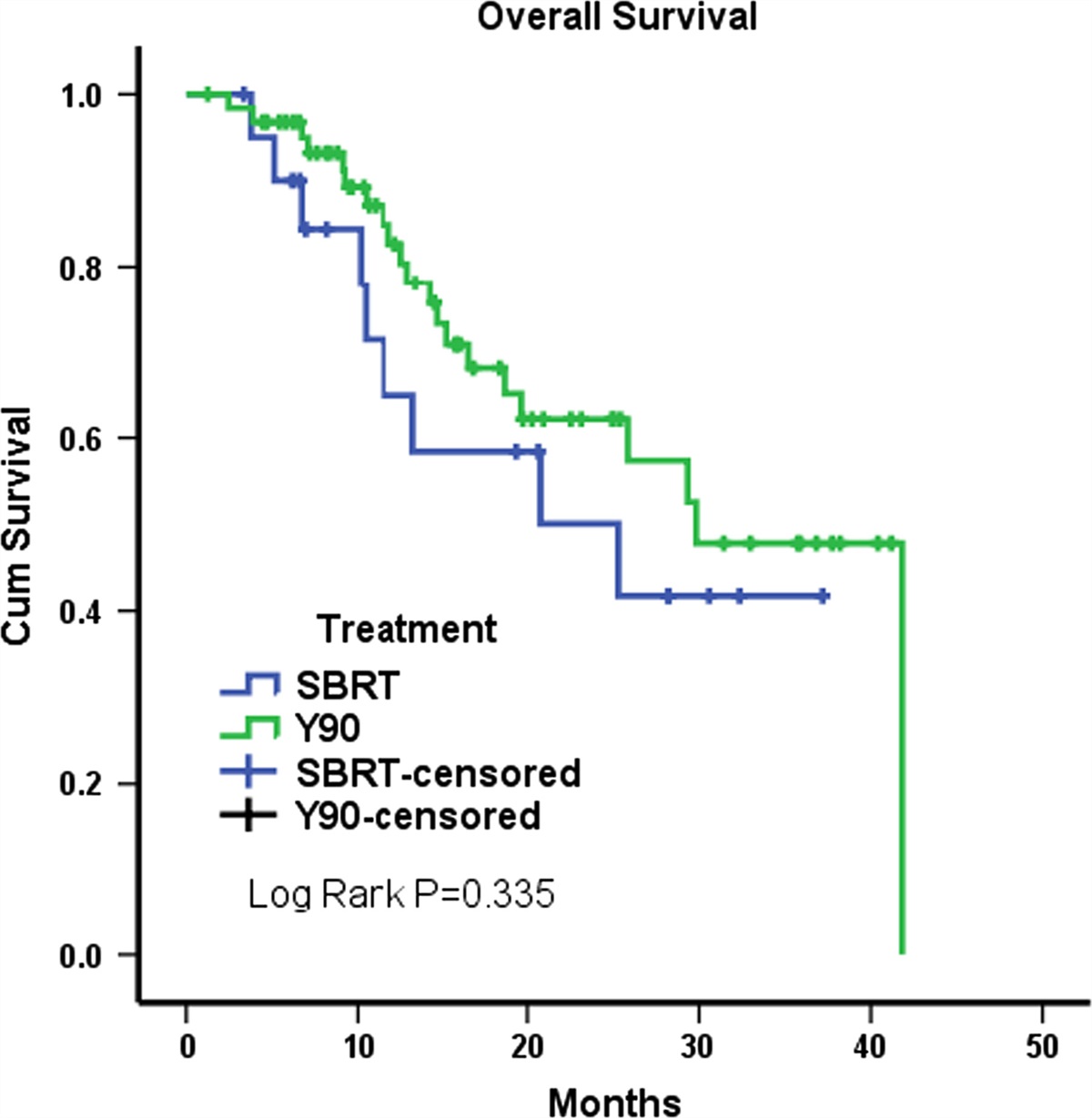
LRF, Distant Metastases, and SurvivalThe median follow-up time was 45.1 months. The 2-year cumulative incidence ofLRF was 5.2% in the neoadjuvant group versus 5.6% in the upfront surgery group (P=0.91, Fig. 1).
 FIGURE 1:
FIGURE 1: Locoregional failure (LRF). This figure shows the cumulative incidence of LRF in the neoadjuvant treatment group versus the upfront surgery treatment group. RT indicates radiation therapy.
Of the 9 patients who experienced LRF, 8 (89%) occurred in patients with tumors above or straddling the PR and 1 (11%) occurred in patients with tumors below the PR. None of the 15 patients with tumors below the peritoneal reflection treated with neoadjuvant therapy had LRF, but 1 (25%) of the 4 patients with tumors below the peritoneal reflection treated with adjuvant therapy experienced a LRF (P=0.05; Table 3). In contrast, for patients with tumors above and straddling the PR, 8 of the 80 (10.0%) patients treated with neoadjuvant therapy had LRF whereas 2 of 54 (3.7%) patients who underwent adjuvant therapy experienced LRF.
TABLE 3 - Local-regional Failures Based on Primary Tumor’s Location Neoadjuvant n (%) Adjuvant n (%) P Above/straddle PR 6/80 (7.5) 2/54 (3.7) 0.41 Below PR 0/15 (0) 1/4 (25) 0.05 ≤10 cm from AV on colonoscopy 1/38 (2.6) 2/34 (5.9) 0.52 >10 cm from AV on colonoscopy 4/56 (7.1) 1/14 (7.1) 0.85 ≤10 cm from AV on imaging 2/51 (3.9) 1/52 (1.9) 0.54 >10 cm from AV on imaging 4/43 (9.3) 2/6 (33) 0.07 Above/straddle SP 0/3 (0) 1/9 (11.1) 0.26 Below SP 5/72 (6.9) 3/34 (8.8) 0.76AV indicates anal verge; PR, peritoneal reflection; SP, sacral promontory.
There were no significant differences in LRF between those who received neoadjuvant versus adjuvant therapy based on whether tumor was ≤10 cm from the AV on imaging or colonoscopy, or where the tumor was in relationship to the sacral promontory (Table 3).
Among those who received neoadjuvant therapy, neither distance from AV on colonoscopy (hazard ratio [HR] 1.065, 95% confidence interval [CI] 0.746-1.520) or on imaging (HR 1.205, 95% CI 0.816-1.78) was associated with LRF. However, among those who received adjuvant therapy, larger distance from AV was associated with lower risk of LRF (colonoscopy: HR 0.866, 95% CI 0.735-1.020; imaging: HR 0.487, 95% CI 0.243-0.977).
The 2-year OS was 97.5% in the neoadjuvant therapy group versus 93.7% for the upfront surgery group (P=0.33). The 2-year cumulative incidence of distant metastasis was 9.2% in the neoadjuvant group versus 10.4% in the upfront surgery group (P=0.54). The primary tumor’s relationship to the PR and sacral promontory, and distance from the AV on colonoscopy or imaging, were not associated with OS or distant metastases.
DISCUSSIONWe report the outcomes of our single-institution experience with treating patients with locally advanced rectosigmoid adenocarcinoma and found that patients who were treated with neoadjuvant radiotherapy had similar cancer control outcomes as those patients treated with upfront surgery, despite having cancers with more adverse prognostic features. In addition, we found that tumors below the PR may derive more benefit in terms of locoregional control from neoadjuvant therapy.
The role of neoadjuvant therapy in the management of locally advanced rectosigmoid adenocarcinoma is controversial. Our institutional practice for the management of tumors in this location includes a multidisciplinary discussion with medical oncologists, radiation oncologists, radiologists, and surgical oncologists, taking into consideration clinical prognostic features and relationship to anatomic landmarks, and shared decision-making between the providers and the patient. The patterns of recurrence after resection for rectal cancer is significantly different from that after resection for colon cancer18–21; thus colon cancers are treated with upfront surgery whereas locally advanced rectal cancers are treated with neoadjuvant therapy to reduce risk of locoregional recurrence. Classifying colorectal cancers as rectal versus colon cancers has in large part been guided by trials that have included tumors within 15 to 16 cm from the AV and/or below the sacral promontory as rectal cancers.2,4–7,9 However, higher rectal tumors have a lower risk of locoregional recurrence, calling into question the relative benefit of neoadjuvant radiotherapy and its associated side effects. Furthermore, in the Dutch rectal cancer study, a subgroup analysis showed that patients with upper tumors, defined as 10.1 to 15 cm from the AV, did not benefit in terms of local control with the addition of neoadjuvant radiotherapy.9
Our study found that cancer control outcomes were similar for rectosigmoid cancers managed with upfront surgery versus neoadjuvant therapy. This was despite the neoadjuvant group having tumors that were higher stage and more often with a close or positive circumferential margin on imaging, suggesting that neoadjuvant therapy overcame these known negative prognostic factors. Similar to our findings, the medical research council-07 (MRC-07) study showed a reduction in local recurrence rates with neoadjuvant as opposed to postoperative therapy for upper rectal tumors, defined as >10 to 15 cm from the AV measured by rigid sigmoidoscopy.7 A National Cancer Database study that included 9313 patients reported that in patients with clinical stage 2 or 3 rectosigmoid cancer, the use of neoadjuvant chemoradiation resulted in significantly fewer positive circumferential resection margins. In their propensity score-matched analysis, the use of neoadjuvant therapy was associated with an improved OS compared with upfront surgery with a 5-year estimated OS of 77% versus 72%, respectively.4Table 4 summarizes the above studies describing outcomes in rectosigmoid cancers.
TABLE 4 - Select Studies of Radiation for Rectosigmoid Cancers Study NCDB Dutch Rectal Cancer Trial MRC-07 Eligibility Stage 2 or 3 rectosigmoid cancer Rectal cancer ≤15 cm from the AV based on flexible endoscopy and below the level of S1-2 Rectal cancer <15 cm from the AV measured by rigid sigmoidoscopy Subgroup analysis of tumors 10.1-15 cm from the AV Subgroup analysis of tumors >10-15 cm from the AV Treatment Neoadjuvant CRT (A) or upfront surgery±adjuvant therapy (B) Preoperative RT followed by TME (A) or TME alone (B) Preoperative RT (A) or upfront surgery with postoperative CRT RT Any fractionation scheme 25 Gy in 5 fractions 25 Gy in 5 fractions (A) or 45 Gy in 25 fractions (B) Overall survival 77.0% (A) vs. 72.0% (B); P<0.01 NA NA Local control Data not available in NCDB 2-year LR: 1.3% (A) vs. 3.8% (B; P=0.17) 3-year LR: 1.2% (A) vs. 6.2% (B; P=0.19) Other key Findings Positive CRM: 8% (A) vs. 11% (B) NA NA pCR was 18.7% (A)AV indicates anal verge; CRM, circumferential resection margin; CRT, chemoradiation; LR, local recurrence; MRC-07, medical research council-07; NA, not applicable; NCDB, national cancer database; pCR, pathologic complete response; RT, radiation therapy; TME, total mesorectal excision.
Interestingly, there were no LRF among 15 patients with primary tumors below the PR treated with neoadjuvant therapy compared with 1 of 4 patients with tumors below the PR having had a LRF treated with adjuvant therapy. In contrast, we found that outcomes with neoadjuvant therapy did not differ based the primary tumor’s distance from the AV seen on colonoscopy or imaging. This may in part be due to inconsistencies and inaccuracies in measuring distance from AV. A retrospective study by Alasari et al compared the rectal tumor distance from AV on MRI and sigmoidoscopy and found that there was a difference of 2 cm or greater in this measurement for 20% of patients. Anatomic landmarks on MRI, like the PR, may be more a more reproducible and accurate way to localize rectal tumors. This study then used anatomic landmarks seen on MRI, such as the PR, to define tumor location and found almost perfect concordance between MRI landmarks and intraoperative location.14 Another study that compared the surgical and radiologic findings of 54 patients found that the accuracy of predicting tumor location relative to the PR by rectal MRI using surgical findings was 90.7%.22 Thus, the PR may be a better landmark than distance from AV to guide treatment selection. Furthermore, studies have found that the PR is easily depictable on MRI in 82% to 90% of patients.16,22 Although soft tissue resolution is lower quality on CT, the rectal cancer location with regard to the PR may still be identified by using the location of the bladder in men or the uterus in women.16
Arguably, a limitation of all the large rectal cancer trials discussed above is reliance of colonoscopy or sigmoidoscopy only for defining rectal tumors to guide treatment management. For example, in the Dutch rectal cancer study that showed that upper rectal tumors did not benefit from neoadjuvant radiotherapy,9 patients were not required to have staging imaging and the definition of rectal tumors was based on the use of flexible endoscopy. With the advances in imaging, MRI is now widely adopted as part of initial staging for locally advanced rectal cancer. There has been an increasing body of literature describing the successful utilization of MRI in identifying patients at higher risk for recurrences, such as those with a close CRM, less depth of invasion, and extramural venous invasion.23–25 However, the specific use of various anatomic landmarks such as the PR to help to optimize the treatment of rectosigmoid cancers has not been widely described and may also aid in limiting unnecessary treatment toxicities for those who may not benefit from neoadjuvant therapy, while simultaneously improving outcomes for patients who may derive the most benefit from neoadjuvant therapy. Although we did not find a benefit with neoadjuvant therapy in tumors above and straddling the PR, this result should be interpreted with caution given small numbers and confounding by indication. Those higher rectal tumors may have received neoadjuvant therapy because of more adverse features.
There are several limitations to this study, including the aforementioned biases inherent to its retrospective design. We tried to limit the impact of these biases by controlling for observable confounders that may have impacted therapeutic decision-making and outcomes in multivariable analyses. In addition, any tumors were found to straddle the PR, and we did not further classify these tumors in terms of extent of tumor below the PR. Although we recognize that a tumor’s relationship to the PR perhaps represents more of a continuum rather than a specific cut point, we did find that no patients with tumors completely below the PR who underwent neoadjuvant therapy experienced a local recurrence. Jung et al22 also similarly found that as the tumor size increased, it became more difficult to determine the exact tumor location in relationship to the PR. Furthermore, some patients in our study had only a staging CT pelvis scan, rather than MRI pelvis, due to these patients treated in previous years when the standard of care did not include a staging MRI pelvis. In patients who underwent a CT scan, we were unable to assess certain characteristics such as the circumferential resection margin.26 Other techniques including positron emission tomography/CT (PET/CT) that may aid in clinical decision-making were not explored. In addition, we assessed only the primary tumor’s relationship to the various anatomic landmarks and did not consider location of involved pelvic lymph nodes. This method is consistent with other published studies detailing the significance of rectal cancers to the fixed parameters seen on MRI12–14,22,27–29; however, nodal location may also influence treatment selection and outcomes. Finally, the subset analysis on outcomes based on the primary tumor’s relationship to PR and sacral promontory may be underpowered to detect differences between the 2 treatments due to the small number of patients within each group.
In conclusion, patients with locally advanced rectosigmoid tumors with adverse prognostic features such as more advanced stage and threatened circumferential resection margin and those below the PR may derive more benefit from neoadjuvant therapy. The PR on imaging may be a reliable landmark used in addition to the tumor distance from the AV to facilitate determination of the most appropriate treatment option. Overall, patient preferences and quality of life concerns may ultimately influence decisions regarding the management of their disease—including consideration of omission of radiation therapy to avoid bowel and sexual dysfunction.30
REFERENCES 1. Surveillance, Epidemiology, and End Results (SEER) Program. Cancer Stat Facts: Colorectal Cancer. 1. Available at: https://seer.cancer.gov/statfacts/html/colorect.html. Accessed April 1, 2022. 2. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. 3. van Gijn W, Marijnen CAM, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011;12:575–582. 4. Venigalla S, Chowdhry AK, Wojcieszynski AP, et al. Comparative effectiveness of neoadjuvant chemoradiation versus upfront surgery in the management of recto-sigmoid junction cancer. Clin Colorectal Cancer. 2018;17:e557–e568. 5. Bosset JF, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355:1114–1123. 6. Cedermark B, Dahlberg M, Glimelius B, et al. Improved survival with preoperative radiotherapy in resectable rectal cancer. N Engl J Med. 1997;336:980–987. 7. Sebag-Montefiore D, Stephens RJ, Steele R, et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. The Lancet. 2009;373:811–820. 8. Martenson JA, Willett CG, Sargent DJ, et al. Phase III study of adjuvant chemotherapy and radiation therapy compared with chemotherapy alone in the surgical adjuvant treatment of colon cancer: results of intergroup protocol 0130. J Clin Oncol Off J Am Soc Clin Oncol. 2004;22:3277–3283. 9. Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638–646. 10. Al Benson B, Venook AP, Al-Hawary MM, et al. NCCN Clinical Practice Guidelines in Oncology Rectal Cancer. Available at: https://www.nccn.org/professionals/physician_gls/PDF/rectal.pdf. Accessed May 23, 2021. 11. Wittekind C. TNM Classification of Malignant Tumors, 6th ed. Chichester, West Sussex, UK; Hoboken, NJ: John Wiley & Sons; 2002. 12. Massalou D, Moszkowicz D, Mariage D, et al. Is it possible to give a single definition of the rectosigmoid junction? Surg Radiol Anat SRA. 2018;40:431–438. 13. D’Souza N, Balyasnikova S, Tudyka V, et al. Variation in landmarks for the rectum: an MRI study. Colorectal Dis Off J Assoc Coloproctology G B Irel. 2018;20:O304–O309. 14. Alasari S, Lim D, Kim NK. Magnetic resonance imaging based rectal cancer classification: Landmarks and technical standardization. World J Gastroenterol WJG. 2015;21:423–431. 15. Bordoni B, Sugumar K, Leslie SW Abai B. Anatomy, Abdomen and Pelvispelvis, Pelvic Floor. StatPearls. Treasure Island, FL: StatPearls Publishing; 2021. 16. Gollub MJ, Maas M, Weiser M, et al. Recognition of the anterior peritoneal reflection at rectal MRI. AJR Am J Roentgenol. 2013;200:97–101. 17. MERCURY Study Group. Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study. BMJ. 2006;333:1–6. 18. Pilipshen SJ, Heilweil M, Quan SH, et al. Patterns of pelvic recurrence following definitive resections of rectal cancer. Cancer. 1984;53:1354–1362. 19. Thomas PR, Lindblad AS. Adjuvant postoperative radiotherapy and chemotherapy in rectal carcinoma: a review of the Gastrointestinal Tumor Study Group experience. Radiother Oncol J Eur Soc Ther Radiol Oncol. 1988;13:245–252.
留言 (0)