In this report, we present a rare case of MFS of the thyroid gland. To our knowledge, only 4 cases of primary thyroid MFS have been reported in the literature so far [6,7,8,9]. Only one case report described the preoperative use of fine-needle aspiration cytology (FNAC), in which cytology revealed no evidence of MFS but anaplastic thyroid carcinoma [7]. However, considering the rapidly growing tumor with a new onset of hoarseness, we would have chosen our therapeutic strategy even without FNAC, except that we would have performed preoperative imaging to rule out distant metastasis or a primary tumor elsewhere.
MFS represents approximately 5% of all soft tissue sarcomas [3]. The term MFS was first introduced by Angervall et al. in 1977 who described a group of tumors with histiocyte- and/or fibroblast-like cells, nodular and myxoid appearance, plexiform pattern of capillary-like vessels, pleomorphism of the nucleus and a large variation in cellularity, polymorphism and mitotic activity [2]. Until the working group of the WHO's Classification of Tumors of Soft Tissue and Bones found a consensus in 2002, MFS were considered as a part of the group of malignant fibrous histiocytoma (MFH). However, with the introduction of new molecular studies and the progress of immunohistochemistry they became a distinct pathological entity [3]. Based on the degree of cellularity, pleomorphism of the nucleus and mitotic activity, MFS are classified from low- to high-grade differentiated tumors [2]. Several grading systems have been proposed, such as the Brodie and FNCLCC systems, which use four and three grades, respectively, but until today there is no uniformly accepted standard grading system that explicitly applies to MFS [1, 3].
Diagnosis of MFS is based on microscopic characteristics, such as the presence of alternating hypocellular myxoid areas and hypercellular fibrous areas with curvilinear vessels [2, 3]. Although there are no specific immunohistochemical markers for MFS, they may stain positively for vimentin, acid mucins and sometimes SMA or CD34 and are negative for S-100 [2, 10].
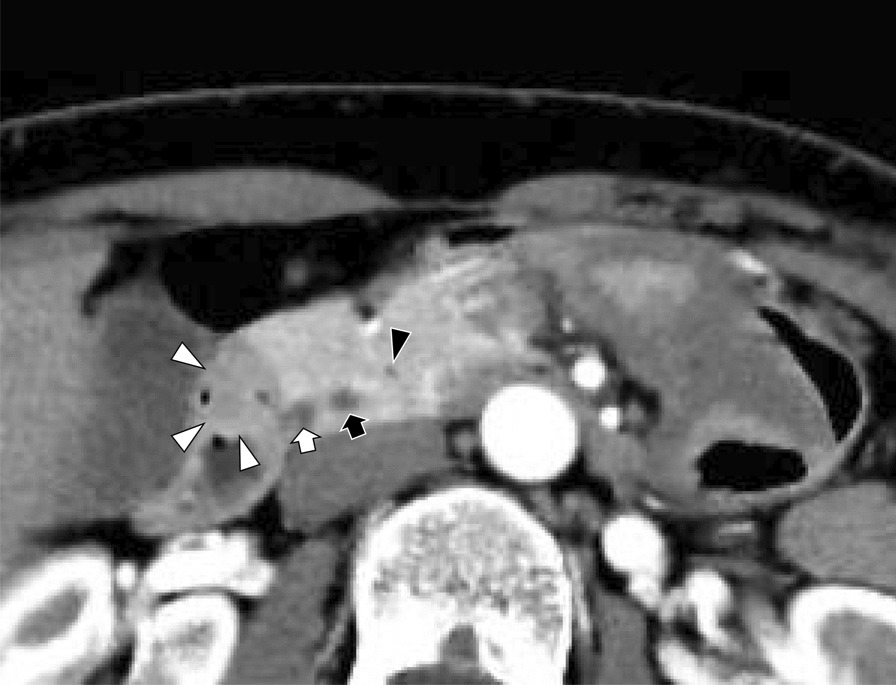
Importantly, radiological findings by imaging techniques such as CT scan and magnetic resonance imaging (MRI) may misdiagnose MFS. For example, in CT-scan low-grade MFS may be misinterpreted as a benign tumor and in MRI T2-weight signal MFS may appear as a cystic formation [10]. Moreover, the tail sign, often used for the diagnosis of MFS in MRI, seems to have neither high sensitivity nor high specificity for the differential diagnosis of MFS from other myxoid tumors [11]. Nevertheless, MRI remains currently the imaging method of choice for patients with MFS. Of note, the use of FDG-PET/CT in the diagnosis of MFS is still under debate. Whereas a number of studies demonstrated comparable results between MRI and PET/CT in the identification of locoregional recurrences, its use in the initial diagnosis of a MFS has yet to be determined [12,13,14].
Irrespective of the grade, MFS shows with up to 61% a high tendency towards locoregional recurrences. Therefore, surgical resection with tumor-free margins, is the standard of care and remains the only chance for cure [15]. Although lymph node metastases are rarely seen at the initial presentation of patients with MFS [16], recent studies demonstrated a frequency up to 31% for lymph node metastases among patients with recurrent distant metastasis [17]. Of note, the study by Sanfilippo et al. [18] reported that 20% of patients who progressed to metastatic disease had previously positive regional lymph nodes. In this respect, the oncologic approach should include prophylactic dissection of the locoregional lymph nodes in addition to resection of the affected thyroid lobe. In our opinion, a total thyroidectomy is not necessary because, in contrast to differentiated thyroid carcinoma, postoperative radioiodine therapy is not indicated.
However, the use of radiotherapy in MFS is still controversial. The existing case series, retrospective studies, and case reports regarding the use of radiotherapy in the treatment of MFS, mostly in an adjuvant setting, show conflicting results [1, 3, 15, 18, 19].
The role of chemotherapy in the treatment of MFS remains unclear [3]. Until today, a randomized clinical trial evaluating the use of chemotherapy specifically in MFS is missing [3]. However, there are a few case series in which chemotherapy is used for the treatment of MFS [5, 18,19,20,21].







留言 (0)