
記住我









This is the case of a 26-year-old G3P2A1 female with a past medical history of polycystic ovarian syndrome (PCOS) status-post tubal ligation that presented with right lower quadrant pain that began 1 h prior to arrival. Stated that this had an acute onset and described it as a constant, stabbing pain that was worst when she moved. She stated that this felt like her past PCOS exacerbations and denied any other infectious symptoms or recent trauma. Her vital signs upon arrival were remarkable for a mild hypotension to 93/48 and tachycardia to 102, but she was afebrile and these both improved with administration of 1L of lactated ringers. On exam, she was found to have tenderness in her right lower quadrant with negative Rovsing and obturator signs. Her labs were grossly unremarkable with no leukocytosis and no electrolyte abnormalities. Her urine pregnancy test was also found to be negative, so the decision was made to pursue a computed tomography (CT) scan of the abdomen and pelvis with intravenous contrast instead of a pelvic ultrasound. By this point, her pain and nausea were beginning to increase so 4 mg of morphine was ordered along with 4 mg of ondansetron for her nausea. She underwent the CT scan which was remarkable for a mild, uncomplicated acute appendicitis without perforation or abscess formation. Surgery was consulted and the patient was consented for an appendectomy. At this time, the patient was requesting more pain medication as she felt that her pain was continuing to increase. After a discussion regarding risks and benefits of more opioid medication versus an erector spinae block, the patient elected to pursue an erector spinae block. The patient was consented for both a block and for research purposes and the procedure was prepared. The patient was situated in a sitting position, similar to a lumbar puncture, with her lumbar vertebrae exposed. While many patients are positioned in the prone position with the operator at the head of the bed facing caudally, our patient’s abdominal pain was exacerbated with the prone position so the decision was made to place her in a less ideal sitting position. One should note that when a patient is placed upright, this may lead to bradycardia or hypotension during the procedure. The operator was positioned behind her and the patient was prepped and draped. Using sterile technique and ultrasound guidance with a curvilinear probe (due to patient’s body habitus), the L1 vertebra was located in the parasagittal plane. The probe was then moved right approximately 2 cm lateral to the spinous process (Fig. 1) and a 21 g Pajunk single-shot 100-mm needle was inserted in a cranial-to-caudal distribution until contact was made with the posterior surface of the transverse process. Hydro-dissection with 10 mL of normal saline with direct visualization confirmed needle tip placement in the fascial plane. After negative aspiration, 20 mL of 0.2% ropivacaine (2 mg/mL) were injected in aliquots of 4–5 mL with repeat aspiration in between. The patient remained on the cardiac monitor for the duration of the block and was monitored for any signs and symptoms of local anesthetic systemic toxicity. Over the next 15 min, she was found to have a significant decrease in pain from a 6/10 to a 1/10 and did not require any more pain medication throughout her stay in the emergency department and initial stay on the floor. Surgery elected to provide an as needed pain regimen of acetaminophen with codeine (300 mg with 30 mg), ketorolac (15 mg), and methocarbamol (500 mg). The patient did not request her first dose of pain medication until 6 h after the block had been performed and required minimal repeat non-opioid doses throughout the night. She underwent an appendectomy the following morning and was discharged afterwards without any complications.
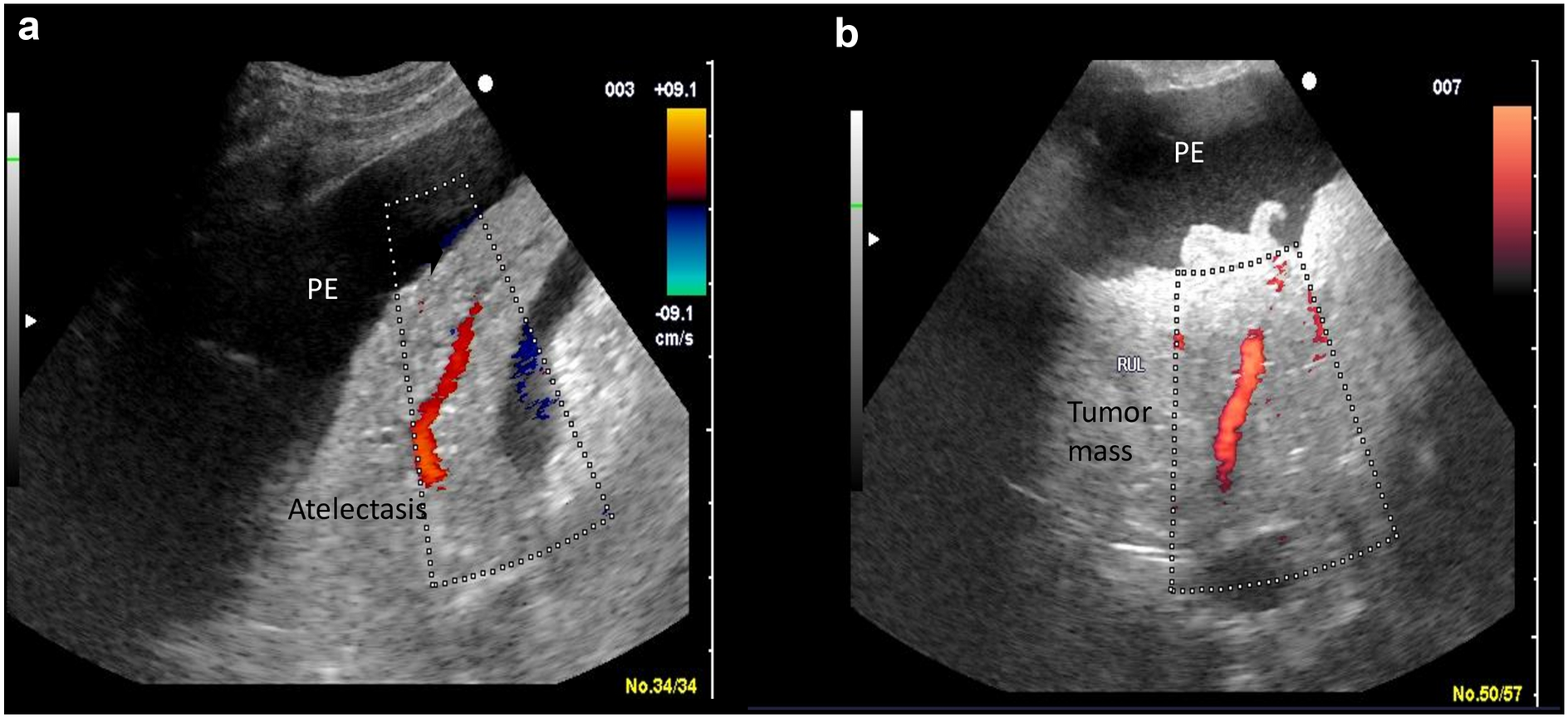
Fig. 1
Longitudinal needle guidance to the L1 transverse process
留言 (0)