
記住我
During Panama’s COVID-19 social distancing measures, we found a decrease in sexual activity among some individuals, especially casual sex encounters among cis-men and participants of Afro-descendant ethnicity.
Virtual sex (sexting and cybersex) use was common before COVID-19 social distancing measures, and reported changes in this practice were associated with a decrease in casual sex.
Condom access, STI and HIV testing, and HIV care were seriously interrupted during COVID-19 social distancing measures in Panama.
IntroductionHIV and other STIs have been on the rise in Panama for the past several years,1 and groups including young adults2 and Indigenous youth who live in comarcas (administratively semiautonomous Indigenous regions)3 are particularly affected. As of 2019, HIV prevalence nationwide was estimated at 0.6%, belying significant concentrated epidemics among men who have sex with men (MSM) (6.9%) and transwomen (29.6%) populations.1 Correspondingly, STI prevalence is more concentrated among MSM, female sex workers and adolescents.3–6 The higher prevalence of HIV and STI in Panama is associated with engaging in sexual activity with new and casual partners due to increased access to connected sexual networks and condomless sex soon after partnership initiation.1
The COVID-19 pandemic has brought several important changes relevant to sexual health and also created challenges for inperson data collection. Many population health surveys and other sexual health research were initially paused. A small number of published studies from North America and Europe have examined the impact of COVID-19 measures on sexual behaviours.7–9 However, there is a research gap in Latin America, especially among more isolated rural and Indigenous populations. There is also little information in the region about how COVID-19 measures have affected HIV/STI testing and care services.
Given the relatively high prevalence of HIV and STIs in Panama and the potential for COVID-19 measures to affect both behaviours and access to medical care, the objective of this study was to examine reported changes in sexual behaviours and access to key sexual health services during COVID-19 measures using an online survey. Based on the association of new and casual partnerships with HIV and STIs, we focused on identifying factors associated with decreased casual sex during COVID-19 measures.
MethodsThis study was an online cross-sectional survey conducted as part of the first round of the International Sexual Health And REproductive Health (I-SHARE), a series of surveys conducted in 34 countries to study sexual and reproductive health during COVID-19 measures.10 I-SHARE Panama was conducted from 8 August to 12 September 2020 at the end of the strictest COVID-19 lockdown measures (figure 1). Participants reported behaviours from the 3-month period before lockdown measures (from 17 December 2019 to 17 March 2020) and during the strictest COVID-19 lockdown measures (from 18 March to 12 September 2020). The survey was advertised on the website and social media (Facebook and Twitter) of the national public health research institute, Instituto Conmemorativo Gorgas de Estudios de la Salud; on the social media of non-profit organisations; and through SMS (short message service) and direct messages sent to individuals and groups who had previously interacted with partner organisations. Targeted invitation was included in provincial and comarcal social media platforms to increase participation in these regions to better match census population estimates (online supplemental table 1). Promotion messages asked adults to fill out the survey and/or share the survey link. No IP (internet protocol) address restrictions were included (more than one result can be recorded on the same device) as mobile phones are commonly shared within households and among community members.
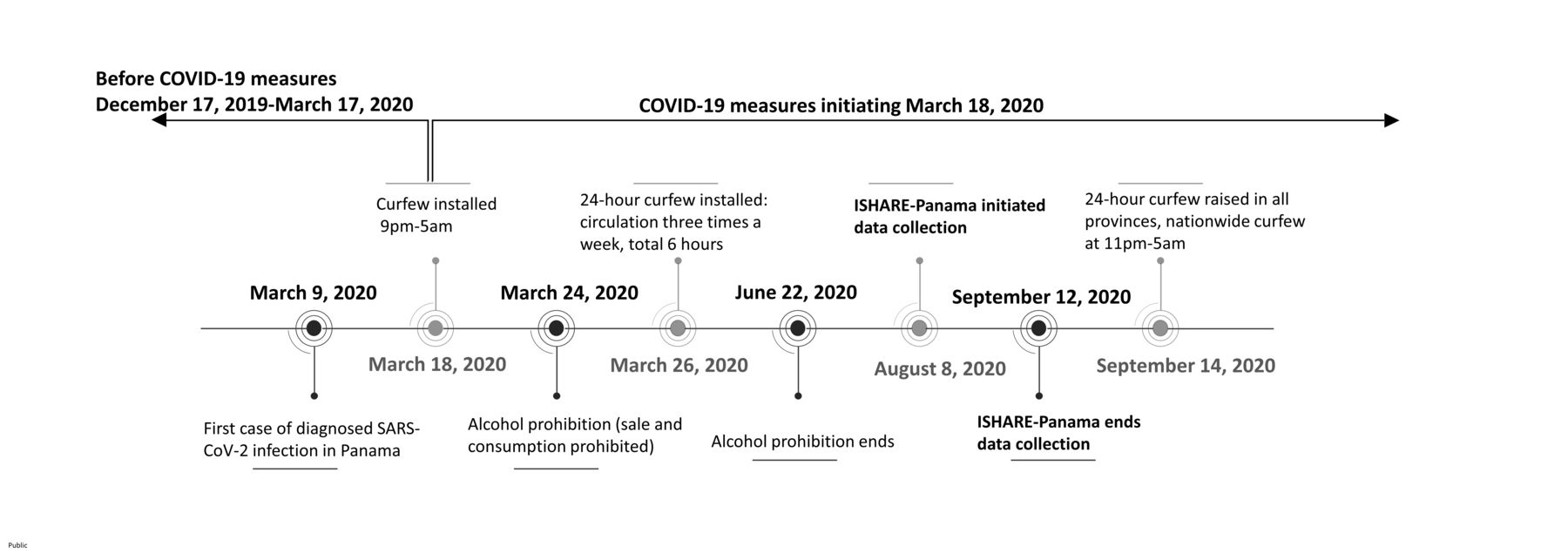 Figure 1
Figure 1 Timeline before COVID-19 social distancing measures and COVID-19 social distancing measures in Panama. I-SHARE, International Sexual Health And REproductive Health.
Study design and populationsWe used convenience sampling. All adults aged ≥18 years who saw the social media/website/messages and lived in Panama were invited to participate.
Questionnaire creation and study proceduresThe questionnaire was collaboratively developed with the I-SHARE consortium.10 Questions were based on existing survey items and multi-item scales, with some new items developed to address the COVID-19 context.11 The Panama instrument was translated from the consortium English to Spanish, programmed into Open Data Kit (University of Washington, USA) and pilot-tested with 15 individuals for understanding and acceptability. Participants completed the online questionnaire in 10–30 min. Only items associated with skip patterns were obligatory.
Key variables of interest occurring over the 3 months before and during COVID-19 measures included sexual intercourse with a casual (new or non-long-term) partner, sexual intercourse with a long-term partner, virtual sex (including ‘sexting’ and ‘cybersex’), and use of sexual health services such as HIV/STI testing (‘Did COVID-19 measures stop/hinder testing access?’) and HIV care (‘Had HIV treatment appointments been cancelled?’). Other influencing variables included age, sex, gender, number of children, ethnic group, urban/rural residence, household and personal income, sexual orientation, general sexual satisfaction, practice of masturbation, long-term partner variables (cohabitation, tensions, emotional support, cuddling), and condom use with casual and/or long-term partners during the specified time.
Statistical analysesWe conducted univariable analyses to describe demographic characteristics. We used χ2 test to evaluate differences by participants’ sex and other influencing variables and the differences between urban/rural residence, casual sex and sexual activity with their long-term partner 3 months before and during COVID-19 measures. All participants with valid data were included; due to non-response to some questions, sample sizes varied.
In addition, we examined factors related to reported decreased casual sex during COVID-19 measures. We undertook a series of three multivariable analyses comparing participants who reported the frequency of casual sex to have stayed the same over the two periods versus those who reported a decrease during COVID-19 measures, having excluded from analysis individuals who reported an increase in casual sex (n=21). The three models focused on different sets of variables: (1) participant sociodemographic variables, (2) individual, casual partner variables and (3) long-term partners’ behaviours. We first used logistic regression to calculate unadjusted bivariable OR and 95% CI. Variables associated with decreased casual sex outcome at p<0.2 level in the bivariable analyses were included in the multivariable models. As the duration of COVID-19 measures differed between urban and rural regions, we adjusted for residence (urban/rural) in the multivariable analyses. Variables independently associated with decreased casual sex at p<0.1 were included in the final model to provide adjusted OR (AOR) and 95% CI, controlling for participant gender and urban/rural residence. Associations with p<0.05 were considered statistically significant.
Only participants who gave online informed consent by ticking a box could participate. No monetary incentive was provided to participants. The survey did not collect WhatsApp phone numbers, telephone numbers, IP addresses or any other identifying information.
ResultsIn total, participants from 11 out of 12 Panamanian provinces responded to the survey; provincial distribution was similar to the 2020 census projection12 (online supplemental table 1). Of 960 participants who completed the online questionnaire, 526 (54.8%) identified as cis-women, 366 (38.1%) cis-men and 68 (7.1%) non-binary or of another gender. The median age was 28 years (IQR: 23–37 years). Mixed ethnicity (mixed Indigenous/European/Afro-descendant ancestry) was reported by 55.5% (531 of 957), Afro-descendant 10.6% (101 of 957), white 22.2% (212 of 531), Asian 1.7% (16 of 957) and Indigenous 10.1% (97 of 957). Overall, 72.4% (679 of 938) identified as heterosexual, 7.8% (73 of 938) as bisexual, 9.6% (90 of 938) as gay or lesbian, and 10.2% (96 of 938) as asexual, pansexual, queer, questioning or another orientation (table 1).
Table 1Sociodemographic characteristics of the study population in Panama, 2020
Sexual behavioursPrevious sexual experience was reported by 88.8% (852 of 960) of the participants. Before COVID-19 measures, casual sex among sexually experienced participants was reported by 18.2% (85 of 466) of cis-women, 32.4% (101 of 312) of cis-men and 23.7% (14 of 59) of non-binary participants (online supplemental table 2). Of those who reported casual sex, always using a condom in such encounters was reported by 50.6% (43 of 85) of cis-women, 61.2% (63 of 103) of cis-men and 53.9% (7 of 13) of non-binary participants (online supplemental table 2). Of all participants, compared with before COVID-19, during COVID-19 measures 68.6% (549 of 800) reported no change, 28.8% (230 of 800) reported a decrease and 2.6% (21 of 800) reported an increase in casual sex (table 2A).
Table 2Sexual behaviours during COVID-19 social distancing measures in Panama, 2020
Of the participants with a long-term partner, sex with the long-term partner and casual sex encounter at least monthly before COVID-19 measures were reported by 18.2% (80 of 440) of cis-women, 33.5% (93 of 278) of cis-men and 25.5% (14 of 55) of non-binary participants.
Overall, before COVID-19 measures, 47.1% (394 of 837) of the participants reported being sexually satisfied (online supplemental table 2). Of those not satisfied before COVID-19 measures, 33.9% (150 of 442) reported increased satisfaction during COVID-19 (table 2A).
Before COVID-19 measures, 46.4% (392 of 845) of the participants reported using virtual sex at least once a month, including sexting in 44.1% (369 of 837) and cybersex in 20.4% (172 of 842). Use of virtual sex had increased during COVID-19 measures for 19.9% (159 of 800) of the participants, decreased for 11.8% (94 of 800) and remained unchanged for 68.4% (547 of 800) (table 2A).
Long-term partner relationship and sexual behavioursOverall, 66.4% (637 of 960) of the participants reported having a long-term relationship before COVID-19 measures; 504 (79.1%) of whom reported to still be in their long-term relationship during COVID-19 measures. Sexual intercourse at least monthly with their long-term partner was reported by 92.7% (332 of 358) of cis-women, 82.5% (160 of 194) of cis-men and 90.9% (40 of 44) of non-binary participants. Decrease in sex with their long-term partner during COVID-19 measures was reported by 50.2% (153 of 305) of cis-women, 52.2% (82 of 157) of cis-men and 48.3% (14 of 29) of non-binary participants (table 2B).
Access to HIV/STI testing and HIV care servicesOverall, 45.6% (375 of 823) of the participants reported that condoms were more difficult to find during COVID-19 measures. This percentage did not differ between urban and rural areas (44.2% (273 of 299) in urban compared with 49.5% (101 of 204) in rural, p=0.38).
Of the 10.4% (100 of 960) who reported needing an STI or HIV test, 58.0% (58 of 100) reported they could not receive it due to COVID-19 measures. This percentage was higher in urban areas; however, the difference was not significant (62.0% (44 of 71) in urban compared with 48.3% (14 of 29) rural, p=0.20).
Few (15 of 960, 1.6%) participants reported to be living with HIV, 8 of whom reported to have had an HIV care appointment cancelled or postponed due to COVID-19 measures. Of the 15 respondents living with HIV, 13 were in urban areas, and all participants living with HIV reported worrying about antiretroviral therapy shortages.
Factors related to decreased casual sex during COVID-19Participant characteristicsAfter adjusting for urban/rural residence, cis-men were more likely to report decrease in casual sex during COVID-19 measures (39.2%) compared with cis-women (22.9%) (AOR=2.17, 95% CI 1.57 to 3.01) (table 3A).
Table 3Demographic, social and sexual factors associated with a reported decrease in casual sex partners during COVID-19 measures in Panama, 2020
After adjusting for participant gender and urban/rural residence, several factors were associated with decreased casual sex during COVID-19 measures. Individuals of Afro-descendant ethnicity reported a larger decrease in sex with casual partners (40.0% compared with 29.8% among mixed ethnicity, AOR=1.78, 95% CI 1.07 to 2.94). There was a weak association between sexual orientation and decreased sex with casual partners (43.2% among gay or lesbian participants vs 26.5% of heterosexual participants, AOR=1.58, 95% CI 0.86 to 2.91) (table 3B).
Participants who reported the same or increased levels of alcohol use during COVID-19 measures were less likely to report decreased casual sex compared with those who decreased their alcohol use during COVID-19 measures (19.5% and 23.7% vs 40.4%, AOR=0.38, 95% CI 0.26 to 0.55 and AOR=0.53, 95% CI 0.32 to 0.85, respectively).
Individual sexual behaviours and virtual sex useAfter adjusting for participant gender and urban/rural residence, an increase in sexual satisfaction was associated with a decrease in casual sex: 45.3% of those reporting an increase in sexual satisfaction also reported decreased casual sex compared with 19.8% among those reporting decreased sexual satisfaction (AOR=2.99, 95% CI 1.85 to 4.84).
Reported changes in virtual sex during COVID-19 measures were also associated with decrease in casual sex in adjusted models. Compared with no change in virtual sex (16.8%), an increase in virtual sex (38.5%) was associated with decreased casual sex (AOR=1.78, 95% CI 1.10 to 2.88), and decreased virtual sex (86.7%, AOR=16.53, 95% CI 7.74 to 35.27) was associated with decreased casual sex.
DiscussionThis study examined reported changes in sexual behaviours, use of virtual sex, and access to HIV/STI testing and HIV care during the implementation of COVID-19 measures in Panama. Our results among a diverse convenience sample of urban and rural dwellers across 11 of 12 provinces expand the literature about sexual behaviours during COVID-19 measures in Latin America. We found that overall sexual activity may have decreased among some individuals. Casual sex, widely practised by 18.2% of cis-women, 32.4% of cis-men and 23.7% of non-binary participants pre-COVID-19, decreased for 22.9% of cis-women, 39.1% of cis-men and 29.6% of non-binary participants. On the other hand, virtual sex, also widely practised by 20%–40% of respondents pre-COVID-19, increased for 20% of the respondents. Finally, participants reported COVID-19 measures interrupted access to condoms, HIV/STI testing and, worryingly, HIV care for those who needed the services.
A large proportion of participants reported decreased sexual activity during COVID-19 measures, findings that differ from the Latvian I-SHARE study, which found most individuals did not have a change in sexual frequency during COVID-19 measures.13 Half of Panama participants reported decreased sex with a long-term partner. This may have been due to extended periods together and increased time with children or other housemates.7 14 Sex with a casual partner decreased among more than a quarter of individuals. Sex with casual partners has also shown to have decreased in the USA and Australia early in the pandemic.7 9 15 A decrease in casual sex partners may provide a unique opportunity for a reduction in behavioural risk, but further research is needed.
Nearly half of our participants reported engaging in virtual sex before COVID-19 measures; 20% used cybersex and 40% used sexting at least monthly, including in very rural provinces. Of the participants, 20% reported increased virtual sex during COVID-19 measures. Before COVID-19 measures, cybersex use in Sweden (32%) was found to be slightly higher than what was found in Panama.16 Some researchers and media outlets hypothesised that virtual sex might increase during COVID-19 due to fewer inperson sexual encounters. However, the first analyses from North America did not demonstrate this.8 9 Interestingly, we found that participants who reported to have either increased or decreased virtual sex use were more likely to report a decrease in casual sex, compared with those who did not change their virtual sex use. Our findings indicate that virtual sex use in Panama may serve both as a substitute and a preamble to inperson sex. A pre-COVID-19 meta-analysis found positive correlations between sexting, number of sex partners and condomless sex.17 As virtual sex practices emerge as normalised, sex-positive tools of sexual behaviour in Panama, privacy and potential extorsion warnings should be addressed within the applications themselves. Additionally, community-wide campaigns could educate on privacy laws and recommend use of encrypted applications.18
The HIV epidemic is concentrated among specific populations, particularly MSM and transwomen; STI prevalence is high among adolescents and unregistered female sex workers.4–6 19 Regular testing of HIV/STI in these populations is considered to aid in controlling transmission. Interruption of HIV/STI services may lead to decreased diagnoses and treatment, thereby increasing continued transmission and increase in sequelae. During COVID-19 measures in Panama, access to key services was interrupted, with over 50% of those needing HIV/STI testing not getting it. This is supported by an overall decrease of 71% of new HIV diagnoses reported by the Panama government during that period.20 An Australian study also found a substantial decrease in HIV tests during 2020.21 HIV testing services elsewhere, including Latin America, have been significantly interrupted during the pandemic.22–25 Respondents also reported disrupted access to STI and HIV prevention (condoms) and HIV care commodities. Such difficulties in accessing HIV/STI testing and care in Panama during the COVID-19 measures may have been related to limited transportation, testing facility closures or the covidisation of health services. Panama does not have policies supporting HIV self-testing and STI sample self-collection, as can be found elsewhere globally. Therefore, our findings suggest the need for patient self-testing approaches26 27 that would help maintain continuity of services during national medical crises.
Our study has several limitations. First, online questionnaires are likely to suffer selection bias as they are only able to include participants who have seen the announcement and are both motivated and able to use online tools. However, given the health emergency context, there was no feasible way to organise a population-representative survey. Additionally, there are no guidelines for online surveys in the EQUATOR (Enhancing the QUAlity and Transparency Of Health Research) network.28 However our study used best practices for the conduct of online research during COVID-19 as outlined in a publication authored by some of our coauthors.29 These recommendations include using an online panel for the study design, implementing the survey with partner organisations, designing the survey for the end-user experience and having a prespecified analysis plan.29 We found that our sample had a similar structure to the 2020 census data in terms of ethnicity, urban/rural residence and province of residence (online supplemental table 1), except that our sample had more female participants compared with the census data. This finding is common in sexual and reproductive health surveys.30 Third, casual sexual encounters may be under-reported as over half of our participants were in long-term partnerships; additionally, memory bias may have enhanced or impaired recall of behaviours from before and during COVID-19 measures. Fourth, comparisons between sexual orientation and gender groups should be interpreted with caution given the relatively smaller sample of non-cisgender respondents. Fifth, this paper focused on casual sexual encounters and sexual behaviours in general. Other related sexual health topics including intimate partner violence, access to reproductive health services and mental health will be reported elsewhere. Sixth, this is a single behavioural cross-sectional study and the capacity for collecting biological samples was limited during this time; therefore, there should be caution when making any causal inferences from the data. Lastly, this analysis is unable to correlate behaviour with biological outcomes and therefore we do not know the impact of behavioural changes on rates of HIV or STI.
Our study has implications for STI and HIV research and policy. Our data suggest the need and usefulness of more rigorous behavioural research during national medical crises that have the capacity to disturb normal services. While we were able to recruit a convenience sample during the pandemic, national panels or other methods can be used to obtain less biased observations.29 These data will be important as lockdown conditions are relaxed and reinforced. From a policy perspective, our data underline the importance of maintaining the continuity of HIV/STI testing and care services even during emergency responses.
ConclusionsOur findings add to the sexual behaviour literature in Panama during COVID-19. We found a decrease in sexual activity among some individuals for casual encounters, paralleled with a rise in the use of virtual sex. STI and HIV prevention and care services were significantly disrupted during COVID-19 measures, suggesting the need for decentralised services.
Abstract translationThis web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statementData are available upon reasonable request to the corresponding author.
Ethics statementsPatient consent for publicationEthics approvalEthical approval was obtained from the Comité Nacional de Bioética de Panama (EC-CNBI-2020-06-73), Ghent University (BC-07988) and the University of North Carolina at Chapel Hill for secondary data analysis.
AcknowledgmentsWe are thankful to all the participants of this study and to all who shared the study links on social media. JMP is a distinguished member of the National Research System that is supported by the National Secretariat of Science, Technology and Innovation. This study was conducted under the umbrella of the I-SHARE study (International Sexual Health and REproductive Health), which examines the impact of the COVID-19 crisis on sexual and reproductive health in diverse low-income, middle-income and high-income countries. The full list of consortium members and their roles can be found at https://ishare.web.unc.edu.
留言 (0)