
記住我

Recent studies on the clinical fitting and application of large-diameter contact lenses (CLs) have shown that the use of large-diameter rigid gas-permeable CLs is on the rise.1,2 Large-diameter rigid gas-permeable CLs, which are commonly referred to as “scleral lenses,”, “corneoscleral lenses,” and “limbal-rigid CLs,”3,4 are used for the refractive correction of corneal irregularities (e.g., keratoconus), as well as after penetrating keratoplasty or trauma, and for the management of ocular surface disorders (OSDs) such as limbal stem-cell deficiency, Sjögren syndrome, and graft-vs-host disease.5–9 Reportedly, the primary purpose of prescribing large-diameter rigid gas-permeable CLs is to improve visual acuity through the correction of optical aberrations and the added benefit of helping to manage dry eye.3,5
Scleral lenses provide several therapeutic effects for patients afflicted with OSDs, such as the masking of irregular astigmatism, the reduction of higher-order aberrations, and the establishment of a precorneal fluid reservoir for the prevention of tear evaporation and corneal dehydration. When scleral lenses are worn in cases with severe dry eye or incomplete closure of the eyelid, the patients commonly complain of cloudy vision and lens fogging, which requires the lenses to be removed and cleaned multiple times per day. Moreover, it has been reported that patients with fornix shortening can experience difficulty when using scleral lenses.7,10,11 Thus, to address those problems, in 2014, we developed and introduced a 13.0- to 14.0-mm diameter limbal-rigid CL. The peripheral edge of the CL rests on the limbus and is specially designed with multistep curves for easy tear exchange beneath the lens during blinking, thus helping to remove debris, prevent lens clouding or fogging, and allow patients to enjoy a longer daily duration of CL wear. Moreover, the lens is specifically designed to fit on eyes with fornix shortening or symblepharon.11
The purpose of this review was to describe the indications, fitting properties and procedures, adverse events, and the overall experience of using a limbal-rigid CL for the treatment of patients with OSDs.
Limbal-Rigid Contact Lens DesignThe limbal-rigid CL (Suncon Kyoto-CS; Sun Contact Lens Co., Ltd. Kyoto, Japan) is a large-diameter rigid CL composed of hexafocon A, a rigid gas-permeable material (oxygen permeability coefficient: 100 Dk). The diameter of this lens ranges between 13.0 and 14.0 mm, with an associated optical zone diameter ranging from 8.50 to 9.00 mm, which is designed to completely cover the cornea and limbus with multistep curves at the peripheral edge that allow tear exchange underneath the lens during blinking (Fig. 1A, B). The tears spontaneously flow under the CL during blinking through a projecting edge of the lens, which is similar to a hat brim. Tears insert beneath the lens from lens edge while lens moves up and down at every blink, creating a thin tear layer on the entire corneal surface (Fig. 1C). This tear movement mechanism was reported by Sotozono et al. in 2014.11 The base curve and power (diopters [D]) ranges from 7.00 to 8.50 mm and −20.00 D to +5.00 D, respectively, and there are 2 specific types of design for the peripheral edge, flat or normal (N) and tight (T) design.11,12
 FIG. 1.:
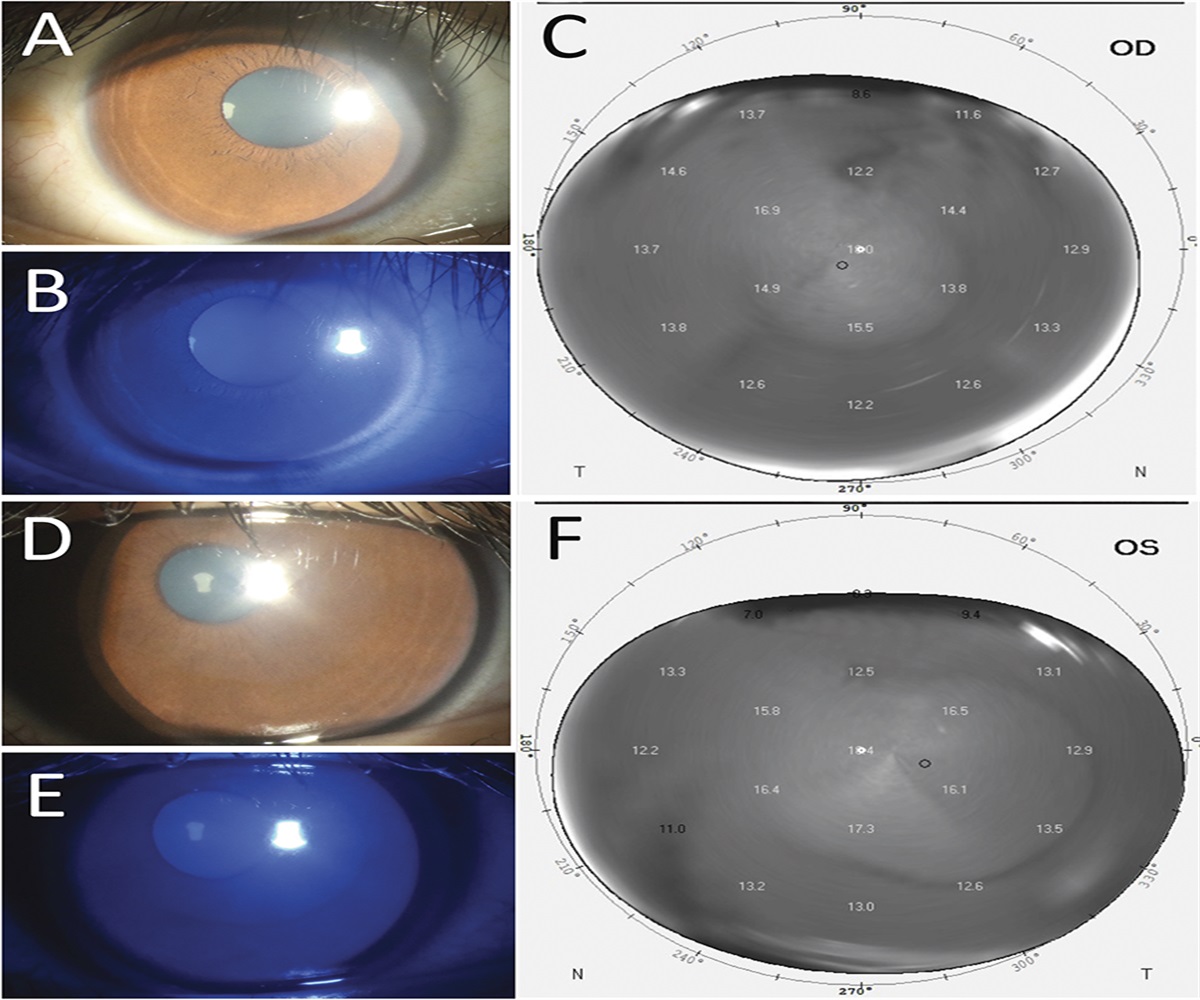
FIG. 1.: Limbal-rigid contact lens (CL) design. (A) Schema illustrating the lens design. (B) Schema illustrating the multicurve design of the peripheral edge of the lens. (C) Anterior-segment optical coherence tomography (AS-OCT) image of the limbal-rigid CL. Moderate OSD case: a. clinical finding image without a CL; b. fluorescein staining evaluation; c. AS-OCT image with the tear layer shown by arrow. Severe OSD case: d. clinical finding image without a CL; e. fluorescein staining evaluation; f. AS-OCT image with the tear layer shown by arrow. BC, base curve; IC, intermediate curve; PC, peripheral curve.
When wearing the limbal-rigid CL, the patient's tears naturally enter the space between the fitted lens and the cornea, resulting in the correction of corneal surface irregularities and the improvement of visual acuity. Moreover, the design of the lens reduces tear evaporation, thus working to alleviate symptoms associated with dry eye.11,13 The comparison between limbal-rigid CL and scleral lens is provided in Table 1.
TABLE 1. - Comparison of Limbal-Rigid Contact Lens (CL) and Scleral Lens Descriptions Limbal-Rigid CL Scleral Lens Lens size (diameter) 13.0–14.0 mm 15.0–23.0 mm Location of lens edge resting Limbus Sclera Lens movement while blinking Moves up and down Less movement Retention and lacrimal fluid exchange through lens movement Smooth tear fluid exchange beyond the lens Retention of tear fluid beyond the lens Moisture retaining Provide constant hydration on the ocular surface Provide constant hydration on the ocular surface Midday fogging None Occurs when debris accumulates between the lens and cornea Fitting process Time consuming: Diagnostic lens fitting Time consuming: Empirical fitting (impression-based technique and eye profilometry) and diagnostic lens fitting Indication Visual rehabilitation in corneal irregularities and therapeutic treatment of ocular surface diseases Visual rehabilitation in corneal irregularities and therapeutic treatment of ocular surface diseases, ocular drug delivery system Eye with fornix shortening or symblepharon Possible to use Unable to useUnlike the fitting procedure clinically applied for the use of a Prosthetic Replacement of the Ocular Surface Ecosystem (PROSE) lens, which is individually customized and involves the use of high-cost fitting software, the procedure used for the fitting of the limbal-rigid CL is far simpler.14–16 Although the procedure is similar to that used for the fitting of a large-diameter rigid gas-permeable CL to the corneal surface, it does not fully rely on an examination of the patient's corneal topography. In addition, in patients afflicted with severe OSDs, the corneal topography does not provide adequate information for proper fitting of the lens. For example, based on the average lens prescription, the fitting begins with the use of a trial set of lenses with the following specifications: a 7.90-mm base curve, a 14.0-mm diameter, an 8.50-mm optical zone, and a flat peripheral edge design. The fluorescein staining pattern is then used to evaluate the centration, the dynamic fit of the lens, and the pooling of the tears (Fig. 2).
 FIG. 2.:
FIG. 2.: Limbal-rigid CL fitting algorithm. The fitting begins with a 7.90-mm base curve, a 14.0-mm diameter, an 8.50-mm optical zone, and a flat peripheral edge design (N). The fluorescein staining pattern is used to evaluate the centration, the dynamic fit of the lens, and the pooling of the tears. A 13.0-mm diameter lens is used if the lens is found to be too large of a size to properly fit on the eye. A best-fit lens is defined as the lens parallel to the cornea with a moderate tear layer in the sclera. If the sagittal depth is deep, change the lens to a 9.00-mm optical zone. Then re-evaluate the fluorescein staining pattern. After confirming the lens, evaluate the peripheral edge of the lens. If the peripheral edge is lifted, change the peripheral edge lens type into tight type (T). Then continue with subjective visual acuity examination. T, tight peripheral edge design; N, flat peripheral edge design; OZ, optical zone; SAG, sagittal depth.
It should be noted that before the fitting and subsequent use of a limbal-rigid CL, it is important to monitor microorganism colonization through the evaluation of microorganisms observed in a conjunctival swab culture. For example, in cases in which there is a positive detection of microorganism colonization on the ocular surface, the patient should first be treated with an antibiotic and the use of the CL should be postponed until negative findings are observed on subsequent microorganism cultures. In ocular Stevens–Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN), methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-resistant Staphylococcus epidermidis (MRSE) were detected higher than other OSDs.17 Prompt treatment shall be started after the detection of these microorganisms.
Indications for Limbal-Rigid Contact Lens UseThe use of a limbal-rigid CL is a nonsurgical approach for improvement of VA in patients afflicted with moderate and severe OSDs. In principle, the primary aims of using a limbal-rigid CL are to improve vision, manage corneal irregularities, reduce dry eye symptoms, and prevent the recurrence of symblepharon after surgery.11,13,18 For the treatment of severe OSDs, such as chronic ocular SJS or TEN, chemical injury, ocular cicatricial pemphigoid (OCP), and graft-vs-host disease, proper surgical management involves numerous considerations and preparations for a good postoperative outcome and the improvement of vision. For example, several previous studies have reported a poor prognosis at only a few years postoperatively, and the prognosis of corneal transplantation in cicatrizing OSD cases is often poor because of a persistent epithelial defect after surgery, infection, the risk of immune rejection, and graft-related problems such as melting or perforation.19,20 In fact, cases with end-stage ocular SJS or TEN reportedly tend to have a worse prognosis after keratoprosthesis caused by postoperative complications, device retention, and poor visual outcome.21 Cultivated oral mucosal epithelial transplantation (COMET) is one surgical strategy applied for the management of severe OSDs because it successfully reconstructs the cornea for visual improvement and the fornix for symblepharon release and is also effective for the treatment of persistent epithelial defects. In fact, the findings in several studies have shown that COMET is very effective for the treatment of numerous severe OSDs.18,22–24
For the treatment of patients afflicted with SJS or TEN, it has been shown that the use of a limbal-rigid CL improves visual acuity after only 3 months of continuous daily wear.11 In that study, best-corrected visual acuity (BCVA) improved from 1.61 to 0.86 logMAR in 43 eyes (81.1%), with the mean BCVA improvement being more than 0.2 logMAR. It should be noted that when a limbal-rigid CL is used, subsequent improvement of visual acuity is directly related to the lens properties that preserve the fluid reservoir beneath the posterior surface of the lens because it prevents tear evaporation on the cornea and neutralizes astigmatism caused by ocular surface irregularities. The design of the peripheral area of the lens allows for smooth and consistent tear exchange under the lens during blinking, which helps to wash away any debris and prevent lens clouding.11,13 Thus, the duration of lens use throughout the day is longer than that of when wearing a scleral lens. However, frequent instillation of artificial tears is sometimes necessary to maintain a healthy wetness of the ocular surface.
The limbal-rigid CL can also be used for the treatment of patients with symblepharon or fornix shortening because the diameter of the lens is smaller than that of a scleral lens, thus allowing the patient to enjoy improved vision and far better quality of life.11 However, in cases in which the lens fails to fit properly because of symblepharon or fornix shortening, symblepharon surgery or fornix reconstruction is required, with additional amniotic membrane transplantation or COMET sometimes deemed necessary. When these procedures are performed, adequate anti-inflammatory treatment is needed to prevent a recurrence.18,23,25 It should also be noted that studies have shown that the use of a limbal-rigid CL at 6 months postoperative can reduce the possibility of symblepharon recurrence and progression because it acts as a physical barrier that prevents conjunctival contact and subsequent abrasion.26,27
Adverse EventsIn our previous study involving 53 total eyes, we found that in 3 of those eyes with asymmetrical upper and lower fornix caused by fornix scarring and symblepharon, pain was reported after several hours of CL wear and that in one eye in which a small epithelial erosion developed, the erosion healed after CL wear discontinuation.13 Moreover, CL use was discontinued in seven of the patients because of poor visual acuity. It should be noted that in our recent clinical trial, 2 of the 10 total eyes in the study experienced a small conjunctival erosion.13 However, the erosion in those two eyes healed several days after CL wear discontinuation.
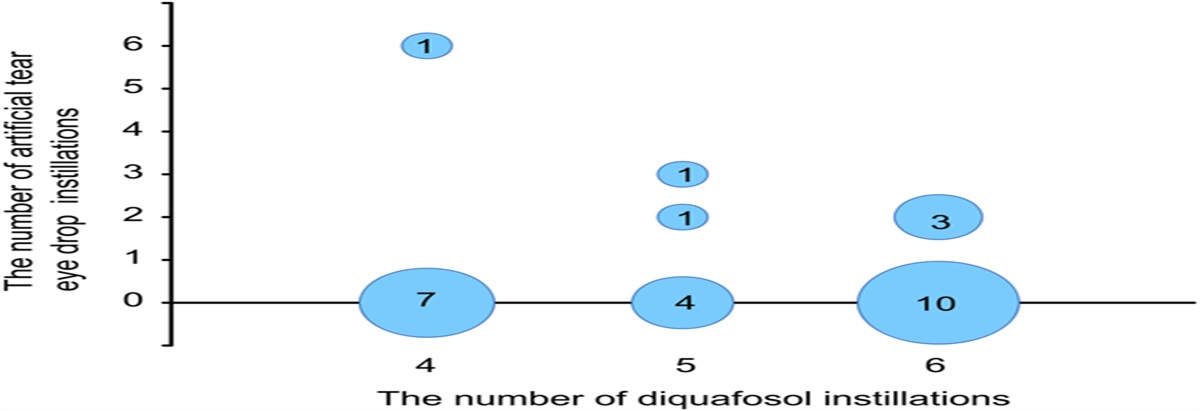
In our recent study on the use of a limbal-rigid CL as a therapeutic modality after COMET for the treatment of severe OSDs, we found that the design of the lens allowed patients to wear the lens for more than 12 hr per day.18 However, it should be noted that extended (i.e., long duration) daily use of a limbal-rigid CL can sometimes induce pain, which usually develops because of a reduction of the frequency of artificial tears instilled by the patient, as the patient feels comfortable and dry eye symptoms are reduced. Thus, it is important to instruct each patient on the proper frequent use of artificial tears when wearing the lens to prevent such pain.
Clinical Data on Limbal-Rigid Contact Lens Use After PrescriptionIn our above-referenced initial clinical trial study on the safety and efficacy of the Suncon Kyoto-CS limbal-rigid CL that involved 53 eyes of patients with SJS or TEN with ocular sequelae, the subjects were divided into the following 3 groups based on their BCVA before the initial fitting of the lens (i.e., at baseline): group 1 (logMAR BCVA>2.0), group 2 (2≥logMAR BCVA>1), and group 3 (1≥logMAR BCVA).11,18 In that trial, patients with SJS-related or TEN-related ocular disturbance and/or severe DE were included. Additional inclusion criteria were an independent or family-supported ability to properly use the provided lenses and a patient age older than 7 years. The primary and secondary outcomes were BCVA after 3 months of lens wear compared with that at baseline and the recorded composite score of the National Eye Institute Visual Function Questionnaire 25 (NEI VFQ-25, a 25-item questionnaire) in Japanese, respectively.28 The average BCVA changes before CL fitting and after 3 months of CL wear are shown in Figure 3. The largest improvement of BVCA was found in group 1, with 0.95 logMAR changes. The mean NEI VFQ-25 score improved from 37.6±16.0 to 58.4±17.4 (P=0.000001). Moreover, a significant improvement was found in all components of the questionnaire, except that for driving ability. In all three groups, improvement in mental health was found, with the greatest improvement occurring in group 3.11
 FIG. 3.:
FIG. 3.: Average best-corrected visual acuity (BCVA) changes in each group. Graph showing the changes of BCVA between at baseline (i.e., before fitting) and at 3 months after the initiation of CL wear in group 1 (logMAR BCVA>2.0), group 2 (2≥logMAR BCVA>1), and group 3 (1≥logMAR BCVA).
In our nonrandomized, interventional, prospective clinical trial to evaluate the therapeutic benefits of limbal-rigid CL wear in cases of SJS or TEN with ocular sequelae, our findings revealed that chronic ocular disorder was present in 10 of the 10 (100%).13 The inclusion criteria were a decimal BCVA between 0.01 and 0.7, a Schirmer one test finding of less than 5 mm, a patient age from 20 to 75 years, and the ability to undergo regular follow-up examinations. In that clinical trial, written informed consent was obtained from all patients before their involvement in the study. The main outcome measure was BCVA at baseline and at 3 months after initiating CL wear, and the secondary outcome was the NEI VFQ-25 score. Our findings revealed that the daily duration of limbal-rigid CL wear was gradually extended from 4 to 18 hr over a 3-month period. Moreover, at baseline, the average BCVA was 0.99 logMAR, which subsequently improved to 0.47 logMAR after 3 months with CL wear (P=0.0039). In fact, in 8 of the 10 eyes, there was an improvement in BCVA of more than 0.2 logMAR. Although the NEI VFQ-25 scores improved in all patients, statistically significant improvement was found only in regard to ocular pain and mental health. The representative clinical findings on those 10 eyes at baseline and at 3 months after the initiation of CL wear are shown in Figure 4.
 FIG. 4.:
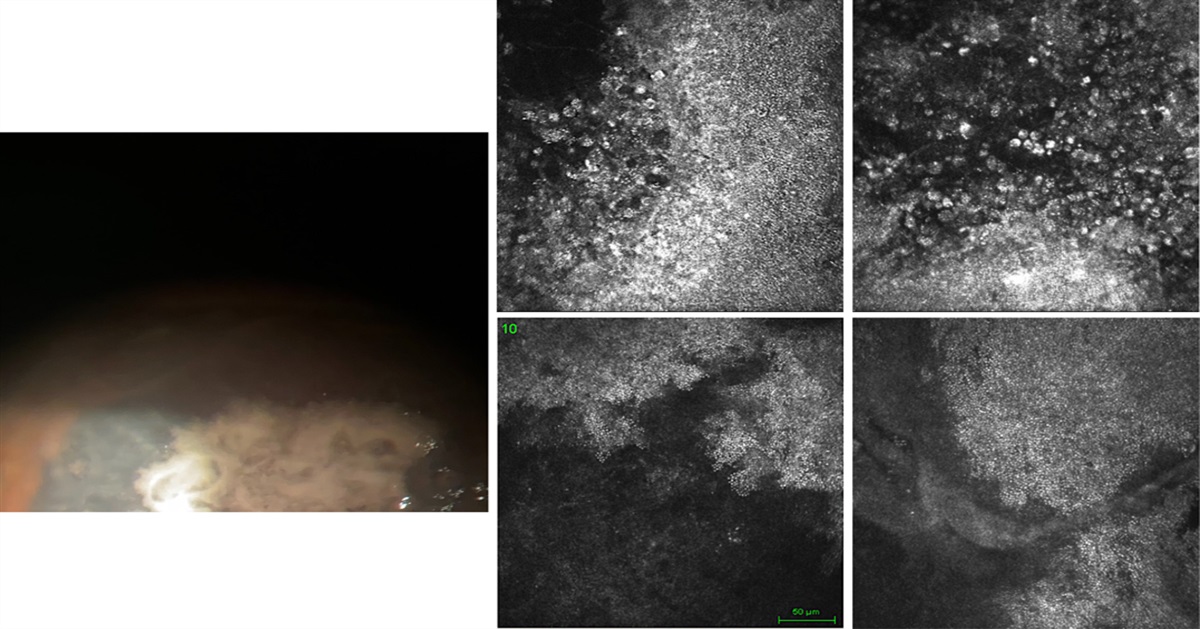
FIG. 4.: Representative clinical findings on the eyes at baseline and at 3 months after the initiation of CL wear. Clinical findings on the eyes treated with limbal-rigid CL wear only, in combination with amniotic membrane transplantation, and in combination with cultivated oral mucosal epithelial transplantation (COMET).
CONCLUSIONIn summary, severe OSDs are conditions that threaten vision and lessen each patient's quality of life. In such cases, the use of a limbal-rigid CL is a very promising nonsurgical therapeutic option for the improvement of visual acuity. Our findings revealed that the best strategy for improving visual acuity in severe OSD cases is to prescribe the use of the limbal-rigid CL itself, or in combination with amniotic membrane transplantation or COMET after surgery, as it improves vision and ocular comfort, reduces dry eye symptoms, and prevents the progression and recurrence of symblepharon. The further enhancement of this lens is promising. As the time-consuming fitting process is still one of the main issues for this kind of lens, stepping forward by using empirical fitting may become an option in the near future.
REFERENCES 1. Porcar E, Montalt JC, España-Gregori E, et al. Fitting scleral lenses less than 15 mm in diameter: A review of the literature. Eye Contact Lens 2020;46:63–69. 2. Nau CB, Harthan J, Shorter E, et al. Demographic characteristics and prescribing patterns of scleral lens fitters: The scope study. Eye Contact Lens 2018;44:S265–S272. 3. Van der Worp E, Bornman D, Ferreira DL, et al. Modern scleral contact lenses: A review. Cont Lens Anterior Eye 2014;37:240–250. 4. Michaud L, Lipson M, Kramer E, et al. The official guide to scleral lens terminology. Cont Lens Anterior Eye 2020;43:529–534. 5. Barnett M, Courey C, Fadel D, et al. Clear—Scleral lenses. Cont Lens Anterior Eye 2021;44:270–288. 6. Moon J, Lee SM, Hyon JY, et al. Large diameter scleral lens benefits for Asians with intractable ocular surface diseases: A prospective, single-arm clinical trial. Sci Rep 2021;11:2288. 7. Harthan JS, Shorter E. Therapeutic uses of scleral contact lenses for ocular surface disease: Patient selection and special considerations. Clin Optom 2018;10:65–74. 8. Schornack MM. Scleral lenses: A literature review. Eye Contact Lens 2015;41:3–11. 9. Gomes JAP, Tan D, Rapuano CJ, et al.; Group of Panelists for the Global Delphi Panel of Keratoconus and Ectatic Diseases. Global consensus on keratoconus and ectatic diseases. Cornea 2015;34:359–369. 10. Schornack MM, Fogt J, Nau A, et al. Scleral lens prescription and management practices: Emerging consensus. Cont Lens Anterior Eye 2021;26:101501. 11. Sotozono C, Yamauchi N, Maeda S, et al. Tear exchangeable limbal rigid contact lens for ocular sequelae resulting from Stevens-Johnson syndrome or toxic epidermal necrolysis. Am J Ophthalmol 2014;158:983–993. 12. Pharmaceuticals Medical Devices Agency. Report on the Deliberation Results [PMDA Web Site]. Available at: https://www.pmda.go.jp/files/000225088.pdf. Accessed January 15, 2016. 13. Itoi M, Ueta M, Ogino K, et al. Clinical trial to evaluate the therapeutic benefits of limbal-supported contact lens wear for ocular sequelae due to Stevens-Johnson syndrome/toxic epidermal necrolysis. Cont Lens Anterior Eye 2020;43:535–542. 14. Lee JC, Chiu GB, Bach D, et al. Functional and visual improvement with prosthetic replacement of the ocular surface ecosystem scleral lenses for irregular corneas. Cornea 2013;32:1540–1543. 15. Shepard DS, Razavi M, Stason WB, et al. Economic appraisal of the Boston ocular surface prosthesis. Am J Ophthalmol 2009;148:860–868.e2. e.2. 16. Weiner G. Update on scleral lenses. [American Academy of Ophthalmology Web site]. Available at: https://www.aao.org/eyenet/article/update-on-scleral-lenses. Accessed February 1, 2022. 17. Sotozono C, Inagaki K, Fujita A, et al. Methicillin-resistant Staphylococcus aureus and methicillin-resistant Staphylococcus epidermidis infections in the cornea. Cornea 2002;21:S94–S101. 18. Sotozono C, Inatomi T, Nakamura T, et al. Oral mucosal epithelial transplantation and limbal-rigid contact lens: A therapeutic modality for the treatment of severe ocular surface disorders. Cornea 2020;39:S19–S27. 19. Tugal-Tutkun I, Akova YA, Foster CS. Penetrating keratoplasty in cicatrizing conjunctival diseases. Ophthalmology 1995;102:576–585. 20. Wakamatsu TH, dos Santos MS, Barreiro TP, et al. Clinical aspects of Stevens-Johnson syndrome and toxic epidermal necrolysis with severe ocular complications in Brazil. Front Med (Lausanne) 2021;8:649369. 21. Metcalfe D, Iqbal O, Chodosh J, et al. Acute and chronic management of ocular disease in Stevens Johnson syndrome/toxic epidermal necrolysis in the USA. Front Med (Lausanne) 2021;8:662897. 22. Sotozono C, Inatomi T, Nakamura T, et al. Visual improvement after cultivated oral mucosal epithelial transplantation. Ophthalmology 2013;120:193–200. 23. Komai S, Inatomi T, Nakamura T, et al. Long-term outcome of cultivated oral mucosal epithelial transplantation for fornix reconstruction in chronic cicatrizing diseases. Br J Ophthalmol 2021;0:1–8. 24. Sotozono C, Inatomi T, Nakamura T, et al. Cultivated oral mucosal epithelial transplantation for persistent epithelial defect in severe ocular surface diseases with acute inflammatory activity. Acta Ophthalmol 2014;92:e447–453. 25. Nakamura T, Inatomi T, Sotozono C, et al. Ocular surface reconstruction using stem cell and tissue engineering. Prog Retin Eye Res 2016;51:187–207. 26. Schornack MM, Baratz KH. Ocular cicatricial pemphigoid: The role of scleral lenses in disease management. Cornea 2009;28:1170–1172. 27. Malooley M, Sonsino J. Scleral lenses in action: Solving problems with specialty lenses. [Review of Cornea & Contact Lenses Web site]. Available at: https://www.reviewofcontactlenses.com/article/scleral-lenses-in-action-solving-problems-with-specialty-lenses. Accessed February 1, 2022. 28. Suzukamo Y, Oshika T, Yuzawa M, et al. Psychometric properties of the 25-item National Eye Institute Visual Function questionnaire (NEI VFQ-25), Japanese version. Health Qual Life Outcomes 2005;3:65.
留言 (0)