Overview of ICU and HDU system in Japan
There are three major categories of acute hospital beds in Japan depending on the patient-to-nurse ratio: ICUs, HDUs, and general wards (Table 1). Compared with HDUs, ICUs require more nurses and space, resulting in more expensive charges per admission. ICUs were further divided into two categories. ICUs for which “ICU management fee 1” can be charged are located in large, well-equipped hospitals such as university hospitals. They have higher standards for full-time staff and facilities: two or more certified intensivists, certified nurses, and certified clinical engineers. Conversely, the other category of ICUs requires a full-time physician, but not necessarily certified intensivists. HDUs and general wards do not require a full-time physician. In Japan, large hospitals often have both ICU and HDU, while middle-sized hospitals often have only ICU or HDU. Smaller community-based hospitals often do not have intensive care units. The Japanese government’s insurance policy limits ICU admission to critically ill patients, such as those with loss of consciousness, respiratory failure, and shock. However, the actual decision of admission to either ICUs or HDUs depends on the medical system of each region, availability of beds, and judgment of the attending physician. Therefore, critically ill patients in Japan are often admitted to HDUs in Japan.
Table 1 Categories of acute hospital beds in JapanStudy design and data source
We conducted a retrospective cohort study using the diagnostic procedure combination (DPC) database provided by Medical Data Vision Co., Ltd. (MDV; Tokyo, Japan) (MDV). This database has been used in previous epidemiological studies [10, 11]. DPC is a payment system for acute hospital inpatients, in which provider reimbursement is calculated based on a per-diem fee according to the diagnosis category [12].
The MDV database is fully anonymized and includes more than 35 million inpatient data points from 438 acute care hospitals, which account for approximately 25% of all hospitals that have opted for DPC (as of the end of April 2021). The database contains demographic data, medical and pharmacy claims data, clinical diagnoses, and medical procedures. The clinical diagnoses were recorded using the International Classification of Diseases, 10th revision (ICD-10) codes. Medical procedures were recorded using Japanese classification codes and medical billing codes. Unfortunately, this database does not include physiological data such as vital signs or information about hospitals in which each patient was hospitalized. The study protocol was approved by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine (R2653).
Study participants
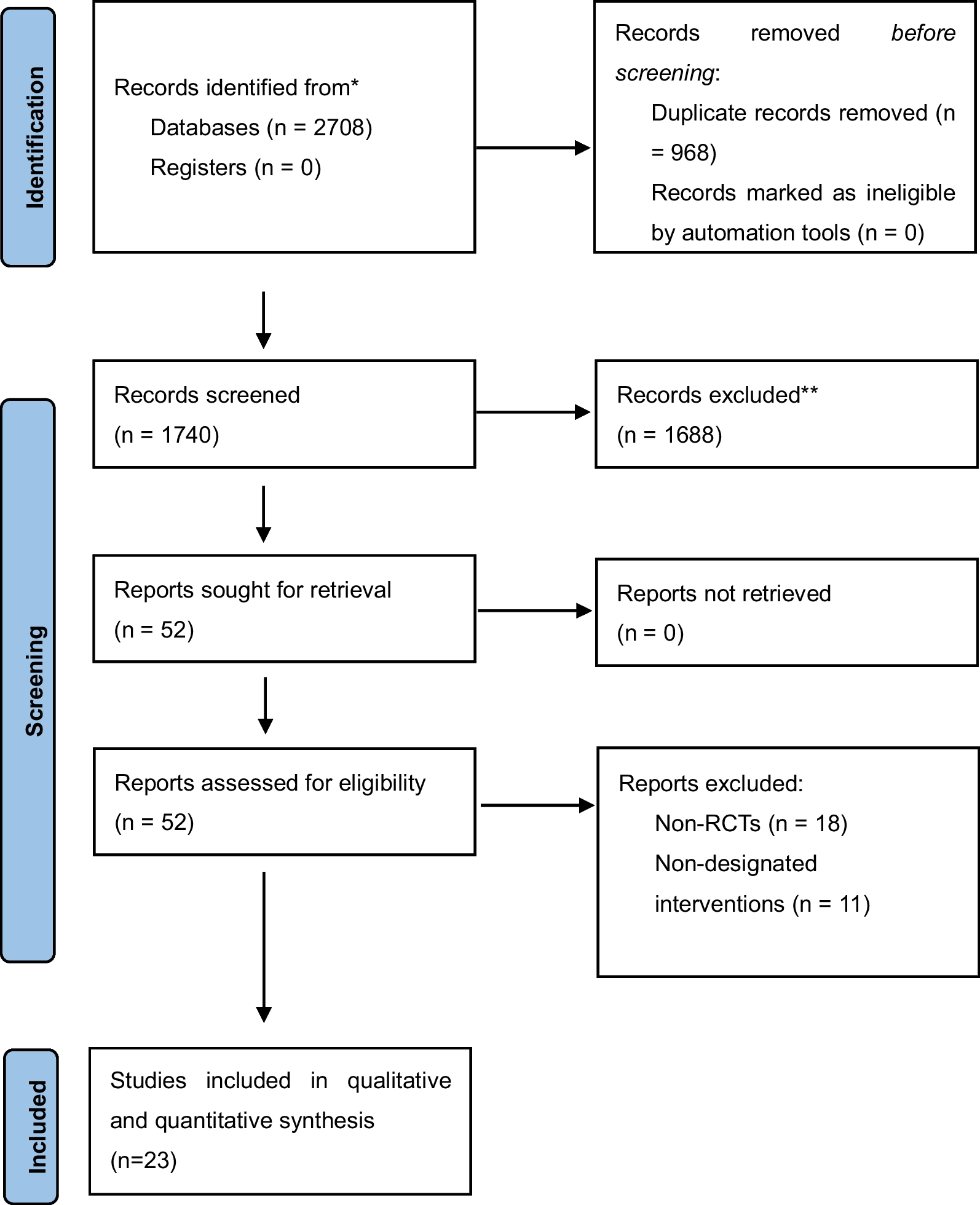
We identified patients with septic shock who were ≥ 18 years and admitted to ICUs or HDUs for intensive care on the day of hospitalization between January 2010 and February 2021. In this study, we defined patients who met the following criteria as having septic shock. First, patients with the diagnosis of both infection (ICD-10 codes A039, A021, A047, A207, A217, A227, A239, A241, A267, A280, A282, A327, A392, A393, A394, A400, A401, A402, A403, A408, A409, A410, A411, A412, A413, A414, A415, A418, A419, A427, B007, B377, J189, J440, N390) and organ dysfunction (ICD-10 codes J960, J969, J80, R092, R570, R571, R578, R579, I951, I959, N170, N171, N172, N178, N179, K720, K729, K763, F050, F059, G931, G934, G938, D695, D696, D65) were identified using the ICD-10 codes that matched the ICD-9 codes used in the previous validation study [13] (Table 2). These diagnoses were identified from the database as main diagnosis, admission diagnosis, diagnosis with the first or second highest medical costs, or comorbidity at admission. Second, patients in whom both intravenous antibiotics and noradrenaline were used on the day of hospitalization. If a patient was hospitalized more than once, we counted each hospitalization as a single hospitalization.
Table 2 ICD-10 codes used for inclusion criteriaPatients who died within 24 h after hospitalization were excluded because they were probably so severely ill they would have died, regardless of the unit type. Patients with the following diseases and procedures at the time of hospitalization were also excluded because they may be incorrectly included by the criteria above: patients complicated with congestive heart failure (ICD-10 code I509), complicated with severe acute pancreatitis (ICD-10 code K859), and patients who underwent the following procedures: percutaneous coronary intervention, coronary artery bypass grafting, valve replacement, valvuloplasty, transcatheter aortic valve implantation, operation for aortic aneurysm or dissection, or endovascular aortic repair.
Exposure and comparison
We defined patients admitted to the ICUs on the day of hospitalization as the exposure group and those admitted to HDUs on the day of hospitalization as the comparison group. We identified admission to the ICUs using Japanese claims codes (classification codes A3002, A3004, A3011, A3012, A3013, A3014) or the HDUs (classification codes A3001, A30011, A3003, A3004, A301-21, A301-22, A301-24). The claims codes present in both groups (classification code A3004) were further distinguished using the accompanying medical billing codes. We excluded the management fee for severe burns from A3003, A3004, A3012, and A3014 to exclude patients with severe burns. If patients with claims codes of both units were identified on the day of hospitalization, we considered them to belong to the first unit group where the initial location they were admitted prior to transfer.
Outcomes
The primary outcome of this study was 30-day all-cause mortality. We identified patient deaths using the discharge outcomes recorded in the DPC database. The secondary outcomes were the length of ICU or HDU stay, length of hospital stay, discharge destination, and Barthel index at discharge. The Barthel index (BI) was calculated based on the activities of daily living (ADL) scores recorded in the DPC database. The cumulative BI score ranges from 0 to 100 points, with 0 indicating complete dependence in activities of daily living and 100 indicating complete independence.
Covariates
The covariates for adjusting confounding factors were age, sex, Charlson comorbidity index [14], admission year, ambulance use, emergency charge, admission from the nursing home, and facility information, such as teaching hospital and number of hospital beds. The following procedures and treatments performed on the day of hospitalization were also identified from the database: emergency surgery or drainage procedures performed for infectious source control, mechanical ventilation, continuous renal replacement therapy, polymyxin B-immobilized fiber column direct hemoperfusion (PMX-DHP), venoatrial extracorporeal membrane oxygenation (VA-ECMO), use of two or more vasoactive agents (dopamine, noradrenaline, dobutamine, epinephrine, and vasopressin), blood transfusion (red blood cells, platelets, fresh frozen plasma), albumin preparations infusion, sedative drugs, narcotic drugs, recombinant thrombomodulin, antithrombin III preparations, low-dose glucocorticoids, and intravenous immunoglobulin. Each patient’s infection source was identified using ICD-10 codes recorded at admission, combined with emergency surgery or drainage procedures performed.
Statistical analysis
Categorical and ordinal variables were summarized using numbers and percentages. If normally distributed continuous variables were summarized using mean and standard deviation, or median and interquartile range if not normally distributed.
We compared 30-day mortality between the ICU and HDU groups using the Kaplan–Meier method and log-rank test and estimated the hazard ratio using multivariable Cox proportional hazard models, adjusting for the covariates mentioned above. Patients who were transferred to other hospitals and discharged within 30 days of hospitalization were censored. The survival period was calculated from the date of hospitalization to the date of death from any cause within 30 days. Secondary outcomes were analyzed using a logistic regression model to evaluate the association between ICU admission and in-hospital mortality. A linear regression model was used to assess the length of ICU (or HDU) stay, length of hospital stay, and Barthel index on discharge. We adjusted all secondary outcomes for the same covariates as those in the survival analysis.
Subgroup analyses were performed for age, procedures performed on the day of hospitalization, and the source of infection. Sensitivity analyses were performed for limited populations as follows: (a) population which include the patients who met the exclusion criteria; (b) population with ICD-9 codes for infection and organ dysfunction from a previous study that did not match ICD-10 codes, supplemented with the corresponding ICD-10 codes (supplement ICD-9 codes: A41.50, A41.51, A41.52, A41.58 with ICD-10 code: A498, supplement ICD-9 code: R572 with ICD-10 code: A419); (c) admission to hospitals with both ICUs and HDUs; (d) 14-day all-cause mortality, and (e) in-hospital mortality. We conducted sensitivity analyses by changing the definition of exposure and comparison (f): (1) “ICU management fee 1” vs. “ICU management fee 3” and “Emergency and critical care unit management fee 2” to examine whether “ICU management fee 1” had better outcomes in ICUs; (2) “ICU management fee 1” vs. “Emergency and critical care unit management fee 1”, to compare outcomes for the most resource-rich ICUs and HDUs, respectively; (3) “ICU management fee 3” and “Emergency and critical care unit management fee 2” vs. “Emergency and critical care unit management fee 1”, to compare outcomes in more resource-poor ICUs to those in the most resource-rich HDUs. We also performed propensity score matching analyses using the nearest neighbor matching (g): (1) caliper width of 0.1 of the standard deviation; (2) caliper width of 0.2 of the standard deviation. A multivariable logistic regression model using all the covariates same as the primary analysis was employed to compute the propensity scores for patients admitted to the ICUs on the day of hospitalization. The statistical significance level was set at a two-tailed p < 0.05, and all statistical analyses were conducted using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).


留言 (0)