
記住我



Eighty-four patients with suspected DA were identified of which 52 patients met the inclusion criteria, 32 patients were excluded because the final diagnosis was not DA (n = 18), there was no CECT available (n = 4), the time between CECT and surgery was more than 8 weeks (n = 6), there was a simultaneous other malignancy (n = 3), or there was no histopathological prove (n = 1). None of the eligible patients had opted out for use of their data for research. Table 1 summarizes patient characteristics. In most patients endoscopy was the modality on which the diagnosis DA was first suspected, followed by CECT. In 13 patients, the diagnosis was initially missed at endoscopy (6/52, 12%), CECT (4/52, 8%), or both (3/52, 6%). The median delay between missed diagnosis and final diagnosis was 12 weeks (1–49 weeks) for endoscopy and five weeks (1–103 weeks) for CECT.
Table 1 Patient characteristicsCECT parametersScan protocols were variable because the study covers a long time range and 75% (39/52) of patients were referred with a CECT scan from other non-academic hospitals. Additionally, in clinical practice most CECT scans are performed because of a specific symptoms, not targeted at DA specifically, usually resulting in a CECT with only a PVP. In our dataset in 14 cases CECT was not targeted at staging DA specifically, but CECT was performed because of analyses of symptoms like weight loss. In the other 38 cases it was known that a duodenal tumor was present or there was a high suspicion. Thirteen CECT scans dated before 2015 (2000–2004 n = 1; 2005–2009 n = 3; 2010–2014 n = 9) and 39 scans dated after 2015. Table 2 compares parameters between scans dated before and after 2015. Contrast type, concentration, volume, flowrate, and delay were not available in the majority of cases due to the retrospective nature of the study.
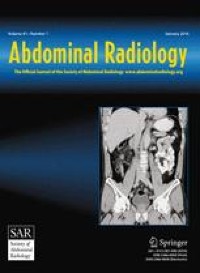
Table 2 Comparison of scan parameters between scans of before and after 2015Tumor characteristics on CECTContrast-enhancement of the tumor compared to normal duodenum on the PVP was classified as; hyperdense, isodense, hypodense, or mixed density. Fifty percent was isodense (26/52) and 10% was not visible on CECT (5/52, Figs. 1 and 2). Tumors mostly involved D2, the descending part (21/52, 40%), with nine of these tumors located in multiple segments including D2.
Fig. 1
Distribution of tumor enhancement on CECT
Fig. 2
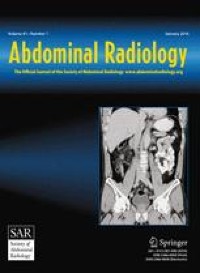
Example for each enhancement pattern on CECT, with the tumor indicated with white arrows. a Axial slice with a hypodense tumor. b Coronal slice with an isodense tumor. c Axial slice with a hyperdense tumor. d Coronal slice with a tumor with mixed density
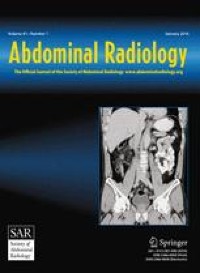
ResectabilityInvolvement of arteries and/or veins that are included in the DPCG criteria for resectability of pancreatic cancer (SMA, coeliac trunk, CHA, SMV, and portal vein) was seen in 11 patients (11/52, 21%). Vascular involvement of jejunal arteries and/or veins, which are not included in the DPCG criteria but, depending on the extent, can render a patient inoperable, occurred in 15 patients (15/52, 29%). Involvement of the inferior caval vein, also not included in the DPCG criteria, occurred in three patients. Examples are shown in Fig. 3. Seventy-three percent (11/15) of the tumors with vascular involvement of the jejunal arteries and veins involved the third or fourth duodenal segment.
Fig. 3
Examples of vascular involvement (indicated with white arrows). a Coronal view of a tumor in D3 with involvement of jejunal arteries and veins in the mesenteric root. b Axial view of the same tumor as a. c Axial view of a tumor in D3 with abutment of inferior caval vein. d Sagittal view of the same tumor as c
Thirty-two patients underwent surgery with a curative intent, of which 26 were resected. Six patients (19%) could not be resected because of unexpected local invasion (4/6) and/or unexpected metastases (3/6). Palliative bypass surgery (gastroenterostomy) was performed in these six patients. On second look in three of these six patients the surgical findings that hampered resection could not be reproduced on preoperative CT scan and in three patients there were in retrospect some indications visible on preoperative CT scan (indeterminate liver lesions or slight vessel induration). Twenty patients received primary palliative treatment, because of metastases (n = 7), locally advanced disease (n = 2), both (n = 2), or insufficient performance status (n = 9). Palliative bypass surgery was performed in five of these 20 patients. Data are displayed in Fig. 4.
Fig. 4
Stacked bar chart representing all patients (n = 52). In the left bar, all patients that underwent surgery with a curative intent (n = 32) and in the right bar patients with primary palliative treatment (n = 20) are displayed. If patients were resected and the reasons patients were not resected are displayed within the bars
Of the patients that underwent surgery with a curative intent (n = 32) the radiologist and surgeon, that individually evaluated resectability, agreed in 88% (n = 28) and disagreed in four cases (1 × radiologist irresectable vs surgeon resectable; 2 × radiologist borderline vs surgeon resectable; 1 × radiologist resectable vs surgeon borderline). Most disagreements (n = 3) were due to a difference in opinion whether the jejunal vein or artery contact would technically allow a resection or not. In one case there was some induration around the AMS, that the radiologist thought not to be tumor contact but inflammation and the surgeon thought it was tumor contact (at surgery there was involvement of the AMS and of several surrounding organs). Of both experts five patients classified as resectable and one patient as borderline, could unexpectedly not be resected during surgery. One patient classified as irresectable by the radiologist was resected. Data are displayed in Fig. 5.
Fig. 5
Nested pie chart representing patients that underwent surgery with curative intent (n = 32). In the outer circle resection (n = 26) vs no resection (n = 6). In the middle circle the prediction of the resectability on CECT of the radiologist and in the inner circle of the surgeon
TNM-staging on CECTT- and N-stage on CECT of resected patients (n = 26) was correlated to histopathology. The T-stage was correctly classified with CECT in 14 patients (54%), underestimated in seven (27%), overestimated in three (12%), and could not be determined in two patients (8%) (Table 3). In patients with an incorrect T-stage the tumor was more often isodense compared to a correct T-stage (8/10 vs 7/14, p = 0.21).
Table 3 Correlation of T-stage on CECT with T-stage at histopathology of resected patients, n = 26Of the resected patients on CECT, there were four patients with N0, eight patients with N1, and 14 patients with N2 and at histopathology there were nine patients with N0, eight patients with N1, and nine patients with N2. The presence (N1 or N2) or absence (N0) of LN metastases was correctly predicted in 11 patients (42%), false positive in two (8%), and false negative in 13 (50%). Sensitivity and specificity for detecting LN metastases on CECT was 24% and 78%, respectively (Table 4).
Table 4 Correlation of N-stage using the conventional definition (≥ 10 mm considered malignant) and alternative definition on CECT with N-stage at histopathology of resected patients, n = 26The results of M-staging for all 52 patients are provided in Table 5. Ten patients were suspected of having metastases: in the liver (n = 7), peritoneal (n = 2), or at multiple sites (n = 1). These were all confirmed by histopathology, 18FDG-PET-CT, or follow-up. Additionally, in one patient peritoneal metastases were not visible on CECT. Nine patients showed indeterminate lesions (Mx) on CECT: in the liver (n = 7), the lung (n = 1), or both (n = 1). In one patient, these lesions were confirmed to be metastases; five patients had no metastases according to the reference standard; and in three patients it remained indeterminate. The M-stage was correct on CECT in 42 patients (81%), underestimated in one patient (2%) and unclear in nine patients (17%).
Table 5 Correlation of M-stage on CECT to the final M-stage of all patients, n = 52, based on histopathology, 18FDG-PET-CT, or follow-upProblem solving tools (18FDG-PET-CT, MRI, and EUS)In 23 patients MRI, in 16 patients 18FDG-PET-CT, and in five patients EUS was performed. In seven patients (7/23, 30%), MRI provided useful additional information: detection of primary tumor (n = 1), confirmation of (suspected) liver metastases (n = 3), detection of liver metastases (n = 1), and better assessment of tumor extension (n = 2). In two patients ,the MRI was false positive for liver metastases. In eight patients (8/16, 50%), 18FDG-PET-CT provided useful additional information: detection of primary tumor (n = 2), confirmation of (suspected) liver metastases (n = 5), and confirmations that suspect liver lesions on CECT were not metastases (n = 1). EUS was mainly used to obtain histopathology (n = 4) and in one patient the tumor was detected during EUS.
留言 (0)