
記住我




A skin tear is “a traumatic wound caused by mechanical forces, including removal of adhesives. Severity may vary by depth (but not extending through the subcutaneous layer).”1 The most common causes of skin tears relate to blunt trauma, dressing removal, helping patients perform activities of daily living, and falls.1 Skin tears are expected to follow an acute wound closure trajectory of 14 to 21 days in the absence of comorbidities that could delay healing, such as diabetes or peripheral edema. Most skin tears occur in the upper extremities (arms and hands) followed by the lower extremities.1 When a skin tear occurs, the skin tear decision algorithm should be followed.1
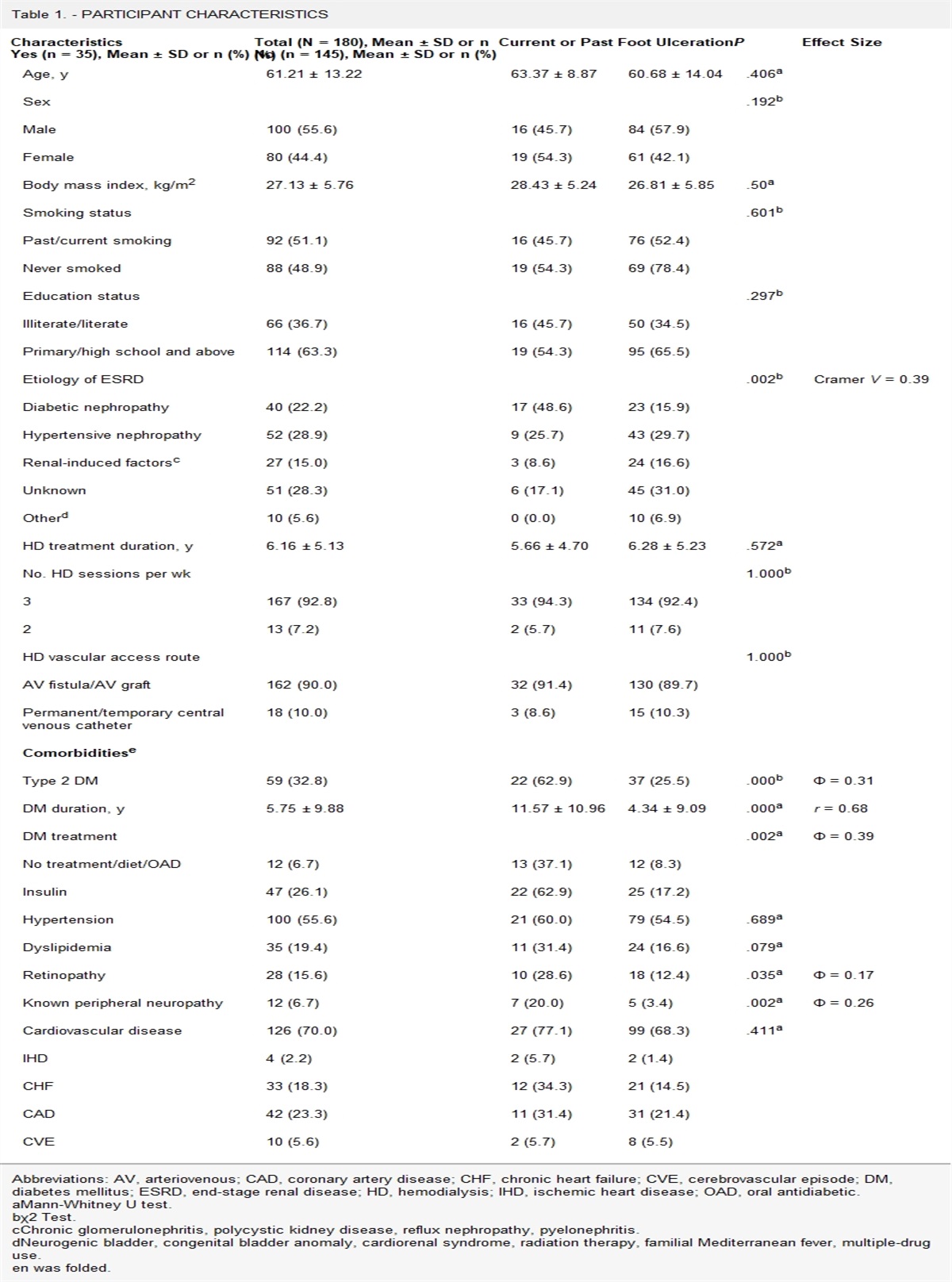
The reported prevalence of skin tears varies across long-term care settings, from 3.0% (Belgium)2 to 9.5% (US),3 14.7% (Canada),4 to as much as 41.2% (Australia).5 Identifying individuals at risk of a skin tear is important. Therefore, clinicians need to take into consideration three main risk categories: (1) the individual’s general health (eg, comorbidities, polypharmacy, impaired cognition, malnutrition), (2) mobility (eg, history of fall, impaired mobility, dependence on assistance for activities of daily living, mechanical trauma), and (3) skin-related issues (eg, extremes of age, dry/fragile skin, previous skin tear).6 Risk assessment should be undertaken on admission and whenever a patient’s condition changes. In addition, healthcare settings should seek to implement a risk-reduction program that includes a skin tear audit, multidisciplinary teamwork, and the use of a validated classification system for skin tears.1
Prior to classifying skin tears, it is essential that any dislodged skin flap be replaced to cover as much of the wound bed as possible (Figure 1). Van Tiggelen et al7 describe a skin flap in the context of a skin tear as “as a portion of the skin (epidermis/dermis) that is unintentionally separated (partially or fully) from its original place due to shear, friction, and/or blunt force. This concept is not to be confused with tissue that is intentionally detached from its place of origin for therapeutic use, e.g., surgical skin grafting.” The International Skin Tear Advisory Panel recommends that the clinician review the patient’s tetanus status and determine the mechanism of injury. If the individual has not received a tetanus toxoid inoculation in the past 10 years, consider inoculation according to individual institutional policy. Inoculate prior to any debridement because exotoxin may be released during wound manipulation.1
STEP 1: Control bleeding. Apply pressure and elevate the limb if appropriate and consider using a dressing such as a calcium alginate until bleeding is controlled.
STEP 2: Cleanse the wound well with an antiseptic cleanser as per local protocol and remove any residual debris or hematoma. Gently pat the surrounding skin to reduce the risk of friction injury.1
STEP 3: Moisten sterile cotton-tip applicators with sterile normal saline and use a gloved finger or sterile tweezers to gently reapproximate the skin flap. The flap should be repositioned to cover as much of the wound bed as possible without applying tension. Applying the flap under tension can result in further tissue damage and possible flap death (Figure 1). If flap death occurs, debridement of necrotic tissue may be required.1
 Figure 1:
Figure 1: REAPPROXIMATING A SKIN TEAR FLAPA, Skin tear on first assessment. B, Skin flap being approximated. C, Flap repositioned; type 1 skin tear. The patient provided consent for these photographs to be published.
STEP 4: Classify the skin tear based on the reapproximated flap.
Once the skin tear flap has been approximated, it is important to choose a dressing that will decrease risk of further trauma (particularly protecting the tissue flap), provide a moist wound healing environment, and manage pain.1 Sutures or staples are not a viable option in older adults because the surrounding tissue is too fragile. Traditionally, skin tears have been treated with skin closure strips. However, the International Skin Tear Advisory Panel maintains that skin closure strips present an increased risk of additional skin injury upon removal. Further, if the flap is not completely approximated, the use of skin closure strips can allow bacteria to enter the wound.1
Instead, type 1 skin tears can be secured with a topical cyanoacrylate, a silicone contact layer, silicone foam dressing, or an acrylic dressing. Figures 2A and 2B show a skin tear flap that has been approximated and secured with a topical cyanoacrylate. The skin tears in Figures 1C and 2B would be classified as type 1. LeBlanc and Woo8 conducted a clinical study to evaluate the use of silicone dressings for the treatment of skin tears. They concluded that skin tears closed almost 50% faster when treated with a soft silicone dressing compared with nonadherent dressings. In addition, consider indicating on the dressing the position of the skin flap and the best direction to remove the dressing without adding additional trauma. If the skin tear is on the lower limb and any underlying arterial disease has been excluded, consider compression therapy to manage edema and promote healing.1 Implement preventive measures to reduce the risk of further skin tears occurring.
 Figure 2:
Figure 2: USE OF A TOPICAL CYANOACRYLATE TO SECURE A SKIN TEAR FLAPA, Skin tear on first assessment. B, Flap repositioned using a topical cyanoacrylate. The patient provided consent for these photographs to be published.
Skin tears can cause pain, complications, and delayed healing, and their prevention and appropriate management where required is of paramount importance. Ensuring a consistent approach to the initial management of a skin tear will improve patient care based on evidence-based recommendations.
1. LeBlanc K, Campbell KE, Wood E, et al. Best practice recommendations for prevention and management of skin tears in aged skin: an overview. J Wound Ostomy Continence Nurs. 2018;45:540–2. 2. Van Tiggelen H, Van Damme N, Theys S, et al. The prevalence and associated factors of skin tears in Belgian nursing homes: a cross-sectional observational study. J Tissue Viability 2019;28:100–6. 3. Hawk J, Shannon M. Prevalence of skin tears in elderly patients: a retrospective chart review of incidence reports in 6 long-term care facilities. Ostomy Wound Manage 2018;64(4):30–6. 4. Woo K, LeBlanc K. Prevalence of skin tears among frail older adults living in Canadian long-term care facilities. Int J Palliat Nurs 2018;24:288–94. 5. Parker CN, Finlayson KJ, Edwards HE, MacAndrew M. Exploring the prevalence and management of wounds for people with dementia in long-term care. Int Wound J 2020;17:650–9. 6. LeBlanc K, Baranoski S, Holloway S, Langemo D, Regan M. A descriptive cross-sectional international study to explore current practices in the assessment, prevention and treatment of skin tears. Int Wound J 2014;11:424–30. 7. Van Tiggelen H, LeBlanc K, Campbell K, et al. Standardizing the classification of skin tears: validity and reliability testing of the International Skin Tear Advisory Panel Classification System in 44 countries. Br J Dermatol 2020;183:146–54. 8. LeBlanc K, Woo K. A pragmatic randomised controlled clinical study to evaluate the use of silicone dressings for the treatment of skin tears. Int Wound J 2022;19(1):125–34.
留言 (0)