
記住我

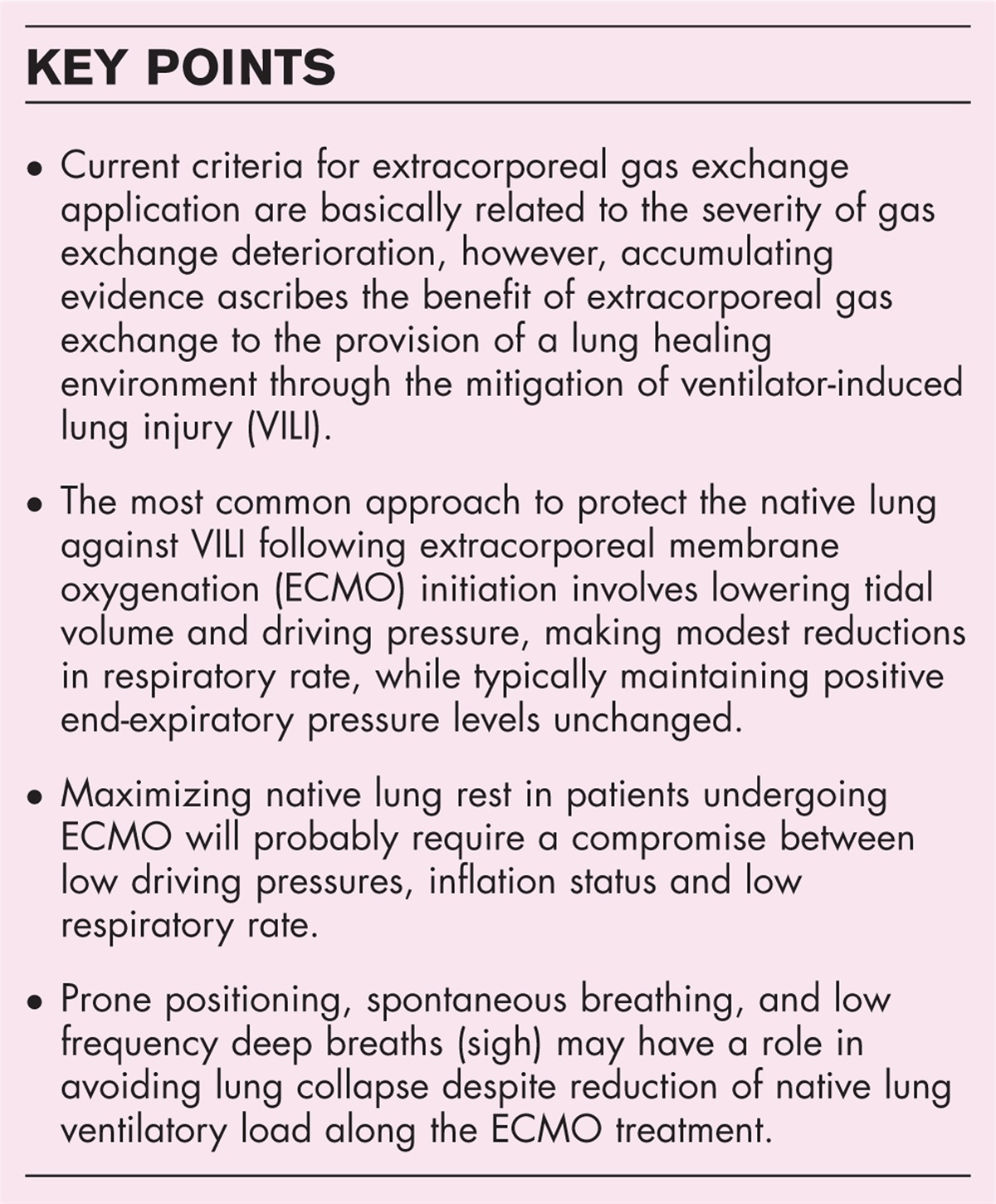
Cardiogenic shock is defined by poor cardiac output resulting in systemic hypoperfusion [1]. Traditionally, the majority of cardiogenic shock presentations occurred in the context of acute myocardial infarction (AMI) resulting in in-hospital mortality that may often exceed 50% [2▪,3,4,5▪▪,6–8,9▪,10▪]. However, the proportion of non-AMI cardiogenic shock has become increasingly prevalent in the last decade due to two reasons: first, incidence of cardiogenic shock from ST-elevation myocardial infarction (STEMI) has been declining due to early recognition and intervention of AMI mediated events to reverse cardiogenic shock [11,12▪] and; second, the increasing prevalence of chronic heart failure with the advancement of guideline-directed medical therapy along with improvement in post-AMI management [11]. To date, only early revascularization in the context of AMI has been demonstrated to improve mortality in cardiogenic shock [3,13–15].
Cardiogenic shock with concurrent valvular heart disease represents a challenging population with limited therapeutic options. Specifically, moderate-to-severe mitral regurgitation (MR) is present in 5–10% of patients with cardiogenic shock [16,17] – and this population is often at prohibitive-risk for surgical interventions due to their requirement for mechanical ventilation, inotropes, vasopressors, or mechanical circulatory support, representing a cohort without established therapies [9▪,18,19]. In the SHOCK trial, patients with AMI complicated by cardiogenic shock and severe mitral regurgitation were treated conservatively with an in-hospital mortality of 55% [14]. Moreover, the cause of mitral regurgitation varies as it may be due to degenerative mitral regurgitation (DMR) in the setting of disease involving the leaflet, chordae tendinae, papillary muscle, or mitral annulus, or functional mitral regurgitation (FMR) in the setting of progressive left ventricular (LV) remodeling and papillary muscle displacement due to ischemic or nonischemic cardiomyopathy resulting in mitral leaflet malcoaptation and mitral regurgitation [20,21]. Traditionally, surgical intervention for mitral regurgitation in cardiogenic shock is reserved for selected DMR patients with unknown benefits in FMR [22,23], whereas transcatheter interventions are being increasingly employed in both DMR and FMR.
Transcatheter mitral valve edge-to-edge repair (TEER) was first approved by the Food and Drug Administration in 2013 and is increasingly being used in FMR in the setting of LV remodeling leading to mitral leaflet mal-coaptation – though, notably, these studies did not include patients with cardiogenic shock [21,24–27]. Moreover, TEER may be utilized in those with significant symptomatic DMR deemed high-risk for mitral valve surgery. The role of TEER as a salvage therapy in patients with cardiogenic shock and MR has been described in many observational studies, demonstrating the feasibility of TEER as a safe alternative [5▪▪,18,28,29,30▪▪,31▪]. Herein, we review the available evidence regarding the patient characteristics, management, impact of TEER on hemodynamics, and clinical outcomes of patients with cardiogenic shock and mitral regurgitation.
 Box 1:
Box 1: no caption available
PATIENT CHARACTERISTICSThe clinical presentation for heart failure and cardiogenic shock varies from ambulatory asymptomatic to hemodynamically unstable patients requiring mechanical circulatory support, inotrope/vasopressors, and possibly cardiac transplantation. The Society for Cardiovascular Angiography and Interventions (SCAI) released a consensus statement for classification of cardiogenic shock to indicate shock severity and mortality risk prediction [32], with stage A (at-risk), stage B (beginning), stage C (classic), stage D (deteriorating), and stage E (extremis) cardiogenic shock [32,33]. Traditionally, the evidence of outcomes in patients with cardiogenic shock and valvular heart disease has been limited to small case series and observational studies as seen in Table 1[18,28,29,34–46] as they were often excluded in randomized clinical trials owing to high in-hospital mortality ranging between 55 and 58% [16,47].
Table 1 - Studies evaluating mortality in the setting of cardiogenic shock and mitral regurgitation Conservative Surgery TEER First author Year Study type Age Male (%) Intervention performed N In-hospital mortality 1-year mortality Hospitalization N In-hospital mortality 1-year mortality Hospitalization N In-hospital mortality 1-year mortality Hospitalization MR grade ≤2 (%) Pleger (1) 2013 Acute MR (n = 6) 69 ± 7 5 (83) TEER N/A N/A N/A N/A N/A N/A N/A N/A 6 N/A 3 (50) N/A 6 (100) Estevez-Loureiro (2) 2015 Acute MR (n = 5) 68 ± 10 N/A TEER N/A N/A N/A N/A N/A N/A N/A N/A 5 1 (20) 1 (20) N/A 5 (100) Adamo (3) 2015 Cardiogenic shock (n = 16) 69 ± 13 12 (75) TEER N/A N/A N/A N/A N/A N/A N/A N/A 16 1 (6) 3 (19) N/A 13 (81) Flint (4) 2018 Acute MR – cardiogenic shock (n = 12) 71.7 ± 12.8 9 (75) TEER N/A N/A N/A N/A N/A N/A N/A N/A 12 1 (8) 30-days: 2 (17) N/A 12 (100) Kesler (5) 2018 Both DMR and FMR (n = 34) 67.3 25 (74) TEER N/A N/A N/A N/A N/A N/A N/A N/A 34 0 (0) 6 months: 3 (9) 6 months: 9 (27) N/A Medvedovsky (6) 2019 Functional MR (n = 6) 69.2 4 (67) TEER N/A N/A N/A N/A N/A N/A N/A N/A 6 1 (13) 3 (50) N/A 5 (83) Chan (7) 2019 Functional MR (n = 27) 71.0 ± 13.0 17 (63) TEER N/A N/A N/A N/A N/A N/A N/A N/A 27 8 (30) 6 months: 17 (63) N/A 25 (93) Eliaz (8) 2019 Acute MI (n = 4) 75.8 ± 4.6 0 (0) TEER N/A N/A N/A N/A N/A N/A N/A N/A 4 N/A 1 (25) N/A N/A Benito-Gonzalez (9) 2021 Both DMR and FMR (n = 17) 76.7 10 (59) TEER N/A N/A N/A N/A N/A N/A N/A N/A 17 0 (0) 30-days: 1 (6) N/A 17 (100) Farwati (10) 2021 AMI versus no-AMI (n = 639) 73 (63–81) 383 (59.9) TEER N/A N/A N/A N/A N/A N/A N/A N/A 639 147 (23) N/A 30 days: 113 (26.3) N/A Tang (11) 2021 DMR and FMR (n = 1192) N/A 688 (57.7) TEER 596 211 (35.4) N/A N/A N/A N/A N/A N/A 596 148 (24.8) N/A N/A N/A Falasconi (12) 2021 DMR and FMR (n = 31) 73 (66–78) 23 (74) TEER N/A N/A N/A N/A N/A N/A N/A N/A 31 7 (23) 6 months: 12 (39) N/A 27 (87) Jung (13) 2021 DMR and FMR (n = 141) 68.9 ± 12.1 78 (55.3) TEER N/A N/A N/A N/A N/A N/A N/A N/A 141 22 (15.6) 55 (42.6) 26 (18.4) 125 (88.7) Haberman (14) 2021 DMR and FMR (n = 471) 73 ± 11 268 (56.9) TEER and Surgery 266 53 (20) 96 (36) N/A 106 17 (16) 32 (31) 6 (6) 99 6 (6) 16 (17) 13 (13) 91 (92) Lorusso (15) 2008 DMR (n = 279) 62.6 ± 14.4 106 (38) Mitral valve repair or replacement N/A N/A N/A N/A 279 N/A 30 days: 63 (22.5) N/A N/A N/A N/A N/A N/A Tavakoli (16) 2002 DMR (n = 21) 62 ± 10 N/A Mitral valve repair or replacement N/A N/A N/A N/A 21 N/A 30 days: 4 (19) N/A N/A N/A N/A N/A N/A Thompson (17) 2000 Acute severe DMR (n = 98) 70.6 (64.4–77.0) 47 (48) Mitral valve repair or replacement 51 36 (71) N/A N/A 43 17 (40) N/A N/A N/A N/A N/A N/A N/A Massimi (18) 2021 Acute DMR (n = 214) 66.9 ± 10.5 156 (72.9) Mitral valve repair or replacement N/A N/A N/A N/A 214 53 (24.8) N/A N/A N/A N/A N/A N/A N/AAge ± standard deviation or (Q1 to Q3).References.1. Pleger ST, Chorianopoulos E, Krumsdorf U et al. Percutaneous edge-to-edge repair of mitral regurgitation as a bail-out strategy in critically ill patients. J Invasive Cardiol 2013;25:69–72.2. Estevez-Loureiro R, Arzamendi D, Freixa X et al. Percutaneous mitral valve repair for acute mitral regurgitation after an acute myocardial infarction. J Am Coll Cardiol 2015;66:91–92.3. Adamo M, Barbanti M, Curello S et al. Effectiveness of MitraClip therapy in patients with refractory heart failure. J Interv Cardiol 2015;28:61–68.4. Flint K, Brieke A, Dominik W, John C. Percutaneous edge-to-edge mitral valve repair may rescue select patients in cardiogenic shock. Circ Conf 2018;138.5. Kesler M, Seeger J, Wohrle J et al. Intra-aortic balloon counterpulsation pump in heart failure patients during MitraClip implantation – a propensity-score matched analysis. Catheter Cardiovasc Interv 2018;92:1433–1438.6. Turyan Medvedovsky A, Tonchev I, Tahiroglu I et al. MitraClip therapy in critically ill patients with severe functional mitral regurgitation and refractory heart failure. Struct Heart 2019;3:296–301.7. Chan V, Messika-Zeitoun D, Labinaz M et al. Percutaneous mitral repair as salvage therapy in patients with mitral regurgitation and refractory cardiogenic shock. Circ Cardiovasc Interv 2019;12:e008435.8. Eliaz R, Turyan A, Beeri R, Shuvy M. Utilization of intra-aortic balloon pump to allow MitraClip procedure in patients with noncoapting mitral valve leaflets: a case series. Eur Heart J Case Rep 2019;3:01.9. Benito-Gonzalez T, Estevez-Loureiro R, Villablanca PA et al. Percutaneous mitral valve repair vs. stand-alone medical therapy in patients with functional mitral regurgitation and heart failure. Cardiovasc Revasc Med 2019;25:25.10. Farwati M, Saad AM, Abushouk AI et al. Short-term outcomes following urgent transcatheter edge-to-edge repair with MitraClip in cardiogenic shock: a population-based analysis. JACC Cardiovasc Interv 2021;14:2077–2078.11. Tang GHL, Estevez-Loureiro R, Yu Y et al. Survival following edge-to-edge transcatheter mitral valve repair in patients with cardiogenic shock: a nationwide analysis. J Am Heart Assoc 2021;10:e019882.12. Falasconi G, Melillo F, Pannone L et al. Use of edge-to-edge percutaneous mitral valve repair for severe mitral regurgitation in cardiogenic shock: a multicenter observational experience (MITRA-SHOCK study). Catheter Cardiovasc Interv 2021;98:E163–E170.13. Jung RG, Simard T, Kovach C et al. Transcatheter mitral valve repair in cardiogenic shock and mitral regurgitation: a patient-level, multicenter analysis. JACC Cardiovasc Interv 2021;14:1–11.14. Haberman D, Estévez-Loureiro R, Benito-Gonzalez T et al. Conservative, surgical, and percutaneous treatment for mitral regurgitation shortly after acute myocardial infarction. Eur Heart J 2021; 43:641–650.15. Lorusso R, Gelsomino S, De Cicco G et al. Mitral valve surgery in emergency for severe acute regurgitation: analysis of postoperative results from a multicentre study. Eur J Cardiothorac Surg 2008;33:573–582.16. Tavakoli R, Weber A, Brunner-La Rocca H et al. Results of surgery for irreversible moderate to severe mitral valve regurgitation secondary to myocardial infarction. Eur J Cardiothorac Surg 2002;21:818–824.17. Thompson CR, Buller CE, Sleeper LA et al. Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK? J Am Coll Cardiol 2000;36:1104–1109.18. Massimi G, Ronco D, De Bonis M et al. Surgical treatment for postinfarction papillary muscle rupture: a multicentre study. Eur J Cardiothorac Surg 2021; 61:469–476.DMR, degenerative mitral regurgitation; FMR, functional mitral regurgitation; MR, mitral regurgitation; TEER, transcatheter edge-to-edge repair.
In the setting of cardiogenic shock with significant MR, the clinical characteristics of patients differs from isolated LV failure as they were more often likely to be female, with less ischemic ECG findings at presentation, greater prevalence of inferior and posterior MI, and delayed presentation of cardiogenic shock [16]. Moreover, a comprehensive systematic review of TEER in MR highlights the severity of the critically ill population who are often of prohibitive surgical risk with their low INTERMACS score (3.1) along with 28.2% presenting with AMI, 24.8% with acute mitral regurgitation, and over 30% in SCAI stage D or above. Furthermore, 78.7% were inotrope dependent and 50.4% required mechanical circulatory support prior to TEER [5▪▪]. Recently, a retrospective international registry compared TEER and surgical mitral valve repair against conservative management and demonstrated improved survival in both TEER and surgical mitral valve repair [30▪▪]. In this observational study, the authors present data on a similar critically ill population on 471 patients with a mean age of 73, with 50% presenting with Killip class at least 3, 35% in cardiogenic shock, and 49% receiving mechanical circulatory support – supporting the notion that TEER is increasingly being employed in this high-risk cohort.
PATHOPHYSIOLOGY: HEMODYNAMICSFMR is commonly seen in patients with ischemic and nonischemic cardiomyopathy due to progressive global or regional LV remodeling causing papillary muscle displacement, leading to leaflet maladaptation and chronic mitral regurgitation [23,48]. Patients with an effective orifice area of at least 20 mm2, regurgitant volume at least 30 ml, or vena contracta width more than 0.4 cm are associated with poor prognosis in FMR with 50% mortality at 3 years [23,49]. Similarly, DMR also has an established echocardiographic criteria with effective orifice area of at least 40 mm2, regurgitant volume at least 60 ml, and vena contracta width at least 0.7 cm [23]. The physiological effects of percutaneous or surgical repair leads to a reduction of MR subsequently causing a decrease in left atrial pressure, pulmonary arterial pressure, and right ventricular afterload while reducing the LV volume and dilation and increasing forward cardiac output to improve hemodynamic status [50,51▪]. Thus, TEER may serve as a salvage therapy in both FMR and DMR to reduce dependence on vasopressors and/or inotropes but also functions as a bridge for long-term management in the form of cardiac transplantation.
INTERVENTIONS Surgical mitral valve repair or replacementHistorically, patients with cardiogenic shock and severe MR following AMI are at prohibitive risk for surgical intervention with over 40% in-hospital mortality despite mitral valve replacement or repair [16]. Surgical mitral valve repair and replacement has been described in the context of AMI and DMR [23,52]. The registry analysis by Lorusso et al. demonstrate that mitral valve surgery was associated with an in-hospital mortality of 26%, similar to prior studies ranging from 22 to 24% [52]. In contrast, surgical interventions remains poorly studied in the setting of FMR, and studies have not demonstrated an improvement in mortality nor shown to affect the natural history of the underlying disease [23,53,54].
More recently, a registry analysis from 2001 to 2019 shed additional light of urgent (undergoing surgery during the same hospitalization) compared with emergent (surgery occurring within 24 hours of admission) and salvage (surgery requiring cardiopulmonary resuscitation en route to the operating room) mitral valve replacement/repair in the setting of papillary muscle rupture [55]. In this cohort, over 64.5% of patients underwent emergent/surgical repair and the in-hospital mortality rates remained consistent with the historical findings of 24.8%, though without significant temporal changes in mortality over the previous two decades. Importantly, the authors demonstrate worse prognosis with acute presentations of cardiac arrest and severe LV dysfunction being associated with 47.4% and 31.1% in-hospital mortality, respectively [55]. Despite significant improvement in supportive therapy in cardiogenic shock, it has not affected mortality rates in mitral valve surgery. Moreover, postoperative complications following DMR repair remains frequent with 26% acute kidney injury, 8% requiring dialysis, 15% atrial fibrillation, 22% infection, and 8% with cerebrovascular accident [55].
Cautious interpretation of studies demonstrating potential benefit of surgery for DMR is required as majority are limited to observational studies often subject to selection bias including inclusion of patients with better LV function and smaller index infarctions [16]. Moreover, despite advancements in supportive therapy, no improvements in mortality has been observed and postoperative complications remain frequent. Except for one study [52], majority of studies are inherent to biases as they failed to describe the setting in which mitral valve surgery was performed specifically raising concerns of selection bias as surgery is delayed until clinical improvement. Finally, FMR remains poorly studied in surgical intervention despite poor prognosis with guideline-directed medical therapy and interventions in cardiogenic shock.
Transcatheter edge-to-edge repair: emerging role in cardiogenic shockGiven the lack of mortality benefits in surgical interventions for FMR, transcatheter interventions were developed to manage FMR. Landmark trials demonstrated the safety and efficacy of TEER in the setting of severe functional and degenerative mitral regurgitation [24–26], specifically with the COAPT trial demonstrating survival benefits in FMR. Despite the evidence for TEER in both DMR and FMR, its utility in the setting of cardiogenic shock and MR remains unclear. Nonetheless, TEER is being increasingly utilized as a therapeutic option in cardiogenic shock and MR in the United States from 2014 to 2019 [51▪]. Small case series and observational studies [18,28,29,34–46] have shown the potential of TEER as a salvage therapy in patients with cardiogenic shock and significant MR (Table 1). This population is often at prohibitive risk for surgery given high Society of Thoracic Surgeons scores (>15%), low INTERMACS score, and dependence on temporary mechanical circulatory support (i.e., intra-aortic balloon pump) and/or inotropes [5▪▪,36].
TEER for cardiogenic shock and MR has been associated with lower than anticipated in-hospital mortality with low periprocedural complication rates. The largest pooled patient-level analysis of 141 patients demonstrated both the procedural safety and efficacy in DMR and FMR following successful MR reduction with a decrease in in-hospital mortality of 15.6% and improvement in heart failure hospitalization (Fig. 1) [5▪▪]. This finding was further confirmed by subsequent registry analyses and systematic reviews resulting in 12–20% in-hospital mortality following successful TEER [31▪,51▪,56]. Compared with historical in-hospital mortality in this population (40% with mitral valve surgery and 60% with conservative management) [16,31▪], TEER appears to be a promising salvage therapy with improvement in both in-hospital and short-term clinical outcomes in a cohort with limited therapeutic options. Despite an absolute reduction in in-hospital mortality, a registry analysis revealed only ∼33% of patients were discharged home following cardiogenic shock admission, highlighting the long recovery process for this critically ill population [51▪].
 FIGURE 1: Impact of transcatheter edge-to-edge repair in cardiogenic shock and mitral regurgitation on in-hospital mortality and heart failure hospitalization following successful reduction in mitral regurgitation grade. Cumulative incidence of in-hospital mortality and composite of 90-day mortality and heart failure hospitalization among patients who underwent transcatheter edge-to-edge repair were stratified by device success. Reproduced with permission Jung et al. [5▪▪].
FIGURE 1: Impact of transcatheter edge-to-edge repair in cardiogenic shock and mitral regurgitation on in-hospital mortality and heart failure hospitalization following successful reduction in mitral regurgitation grade. Cumulative incidence of in-hospital mortality and composite of 90-day mortality and heart failure hospitalization among patients who underwent transcatheter edge-to-edge repair were stratified by device success. Reproduced with permission Jung et al. [5▪▪].Several procedural advantages favor TEER as a salvage therapy in SCAI stage C–E cardiogenic shock and MR. Specifically, the absence of need for cardiopulmonary bypass and a significantly lower complication profile may outweigh superior MR reduction achievable with surgical repair. Prior studies have shown significant reductions in major postprocedural complications (composite of MI, stroke, cardiac tamponade, reintervention, acute kidney injury requiring renal replacement therapy, sepsis, or blood transfusion) with TEER compared to surgery [30▪▪]. Finally, TEER has previously been shown to improve mortality in FMR [24], a cohort with limited evidence in the surgical population. All these factors make TEER an attractive emerging therapy in patients with cardiogenic shock.
Nonetheless, despite the promising improvement in short-term mortality, cardiogenic shock patients whom have undergone TEER continue to accrue adverse events after discharge with an estimated rate of 50% 1-year mortality following successful TEER [5▪▪,31▪,51▪]. With successful TEER implantation, 1-year mortality rate was reduced to 39.7% compared with 69.2% in those without device success [5▪▪]. The high rate of mortality at 1-year likely reflects the highly comorbid cohort at baseline prevalent with chronic kidney disease, chronic pulmonary disease, peripheral arterial disease, type 2 diabetes, and underlying cardiomyopathy [5▪▪,31▪]. Amongst those who survive, significant improvement in New York Heart Association (NYHA) class and quality of life was observed at the time of follow-up. Though cautious interpretation of the available data needs to be made, TEER appears to be a promising hypothesis-generating intervention to consider as a bridge or adjunct therapy to cardiac transplantation or ventricular assist devices [31▪]. Beyond the initial hospitalization – ongoing aggressive therapies need to be instituted to continue to reduce long-term mortality.
On the contrary, despite the promising short-term outcomes of TEER, there remains several questions which remain unanswered. Observational studies fail to address the optimal timeline from hospital admission to TEER implantation. Martinez-Gomez et al.[31▪] estimates the median time from admission to implantation was 22 days [interquartile range (IQR) = 9–45 days], which may be explained by TEER being performed following stabilization of patients with mechanical circulatory support and inotrope/vasopressors. One may speculate that following the initial stabilization, there remains a cohort of cardiogenic shock patients with persistent backward failure due to significant mitral regurgitation where TEER will promote pulmonary decongestion and allow weaning of inotropy [57]. It also remains unknown whether severe mitral regurgitation is the primary mediator or consequence of cardiogenic shock. Moreover, the group demonstrated a median time to wean from cardiac and/or respiratory support of 2 days (IQR = 1–4 days) [31▪]. Though TEER appears to demonstrate in-hospital and short-term clinical benefits, more research is required in this field to identify the optimal patient characteristics, clinical presentation, hemodynamic parameters, and time from admission prior to TEER to fully understand the population and mechanism to which TEER benefits this cohort in cardiogenic shock and mitral regurgitation.
Future directionsThe utility of TEER in the context of cardiogenic shock with significant MR may be associated with mortality benefits as seen observational studies [5▪▪,30▪▪,31▪,51▪]. Randomized trials are needed to confirm these observations and to establish MR as a bonafide therapeutic target. The safety and efficacy of TEER in patients with significant mitral regurgitation (3+) and cardiogenic shock (SCAI stage C or D) will be studied in a multicenter randomized control trial of TEER and medical management (CAPITAL-MINOS) compared with medical management in patients with the primary outcome of in-hospital all-cause mortality. Pending results of this study, the current literature demonstrate the association between TEER and short-term survival in this cohort.
CONCLUSIONCardiogenic shock with significant mitral regurgitation portends a poor prognosis and there are limited therapeutic options. In this review, we highlight the evidence for TEER in cardiogenic shock and mitral regurgitation as it is technically feasible and is associated with improvement in both in-hospital and short-term clinical outcomes. Observational studies highlight the potential of TEER as a salvage therapy – though, future randomized controlled trials are focusing on the potential benefit of TEER against medical management.
AcknowledgementsR.G.J. was funded by the Vanier Canadian Institutes of Health Research (CIHR) Canada Graduate Scholarship for his graduate studies.
Financial support and sponsorshipThe current work was not financially supported by any granting agencies.
Conflicts of interestB.H. reports funding as a clinical trial investigator from Abbott, Boston Scientific, and Edwards Lifesciences outside of the submitted work. The other authors report no conflicts.
REFERENCES AND RECOMMENDED READINGPapers of particular interest, published within the annual period of review, have been highlighted as:
▪ of special interest
▪▪ of outstanding interest
REFERENCES 1. Van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation 2017; 136:e232–e268. 2▪. Samsky MD, Morrow DA, Proudfoot AG, et al. Cardiogenic shock after acute myocardial infarction. JAMA 2021; 326:1840. 3. Jung RG, Di Santo P, Mathew R, et al. Implications of myocardial infarction on management and outcome in cardiogenic shock. J Am Heart Assoc 2021; 10:e021570. 4. Thiele H, Akin I, Sandri M, et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med 2017; 377:2419–2432. 5▪▪. Jung RG, Simard T, Kovach C, et al. Transcatheter mitral valve repair in cardiogenic shock and mitral regurgitation: a patient-level, multicenter analysis. JACC Cardiovasc Interv 2021; 14:1–11. 6. Thiele H, Ohman EM, de Waha-Thiele S, et al. Management of cardiogenic shock complicating myocardial infarction: an update. Eur Heart J 2019; 40:2671–2683. 7. Russo JJ, Aleksova N, Pitcher I, et al. Left ventricular unloading during extracorporeal membrane oxygenation in patients with cardiogenic shock. J Am Coll Cardiol 2019; 73:654–662. 8. Harjola VP, Lassus J, Sionis A, et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17:501–509. 9▪. Mathew R, Di Santo P, Jung RG, et al. Milrinone as compared with dobutamine in the treatment of cardiogenic shock. N Engl J Med 2021; 385:516–525. 10▪. Di Santo P, Mathew R, Jung RG, et al. Impact of baseline beta-blocker use on inotrope response and clinical outcomes in cardiogenic shock: a subgroup analysis of the DOREMI trial. Crit Care 2021; 25:289.
留言 (0)